Patients › Shoulder
肩锁关节骨关节炎
AC joint osteoarthritis causes localized shoulder pain with cross-body movements; treatment ranges from activity modification to surgery.
您的感受¶
您可能会在肩膀最顶端感到疼痛,即锁骨与肩胛骨相接处。这是您的肩锁关节。这种酸痛可能会持续多年且程度轻微。事实上,在7年的时间里,90%在X光片上显示出早期迹象的人完全没有疼痛感。然而,如果症状确实出现,它们通常遵循可预测的模式。
当您把胳膊横过身体时,疼痛通常会加重。当您伸手去够高处的架子或在背后扣文胸时,您可能会感到疼痛。把衬衫塞进裤子里也可能引发尖锐的刺痛。举起物体,尤其是举过头顶,会对这个关节产生直接压力。许多患者发现,将手臂放在身体侧面休息可以缓解疼痛。轻微的活动通常比完全静止感觉更好。
夜间疼痛是一个常见的抱怨。如果您侧卧压到患侧肩膀,可能会醒来。身体的重量压在发炎的关节上,使得很难找到一个舒适的姿势。有些人注意到,他们在早晨刚醒来时疼痛更严重。在活动一段时间之前,关节可能会感觉僵硬。
重要的是要知道,影像学发现并不总是与您的症状相符。区分有症状和无症状的X光肩锁关节炎是没有必要的。无论X光片显示什么,所有患者对术前肩锁关节注射结果的满意度都是相同的。这意味着您的不适程度是治疗的真正指南,而不仅仅是扫描中关节的外观。
如果您之前做过肩膀手术,例如肩袖修复术,该关节未治疗的关节炎与较低的失败率相关。它很少单独引起重大问题。然而,如果您经历持续疼痛,干扰穿衣或睡眠等日常任务,您的外科医生可能会讨论注射或切除磨损骨端的微创手术等选择。这些手术可为有症状的病例提供可预测的疼痛缓解。
实际发生了什么¶
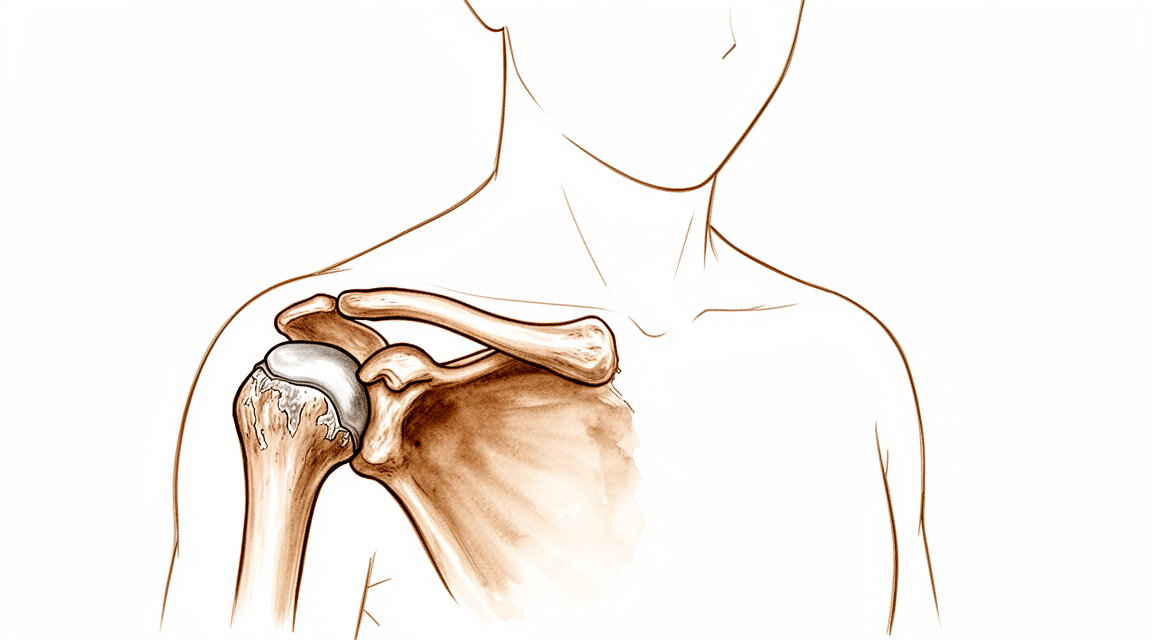
您的肩锁(AC)关节位于肩膀的最顶端,即锁骨与肩胛骨相接之处。可以将此关节视为一个小铰链,使您的手臂能够顺畅地举过头顶。关节内部,光滑的软骨充当减震器,缓冲骨骼,防止它们相互摩擦。
在肩锁关节炎中,这种保护性软骨会随时间推移而磨损。这本质上是磨损性关节炎。随着缓冲层变薄,骨骼之间的直接接触摩擦增加。这种摩擦会导致炎症和疼痛,尤其是在您横跨身体或举臂过头时。包裹关节的关节囊也可能变得僵硬或受刺激,从而加重不适。
有时,固定锁骨的韧带会拉伸或撕裂。这可能导致锁骨位置高于正常水平,形成可见的隆起。当这种情况发生时,肩胛骨的正常运动模式会发生改变。这些运动学改变可能是肩关节疼痛和功能障碍的潜在来源。即使X光片显示关节外观正常,运动模式的改变仍可能引起症状。
重要的是要知道,X光片上的所有改变并不意味着您会出现疼痛。在7年的观察期内,90%的无症状肩锁关节炎患者保持无症状。这意味着许多人在影像检查中可见磨损迹象,但完全没有疼痛感。在关节镜下肩袖修复术中遇到的未治疗的肩锁关节骨关节炎(无论是否有症状)与较低的失败率相关。
然而,如果关节炎变得严重,可能会导致其他问题。严重的肩锁关节骨关节炎与反式肩关节置换术后肩峰应力性骨折相关。您的外科医生将结合您的症状和影像学检查来判断关节是否确实是您疼痛的来源。
治疗的目标是减少这种摩擦并恢复顺畅的运动。开放性和关节镜下切除成形术技术均能为有症状的肩锁关节炎提供可预测的疼痛缓解。这些手术涉及切除锁骨的一小部分以创造更多空间,使骨骼能够滑动而不发生摩擦。这一简单的改变可以显著改善您的肩关节功能并减轻疼痛。
我们能采取的措施¶
您可以从自我管理和物理治疗开始。这种保守疗法是许多肩部损伤和关节疾病的有效初始治疗方案。如果您患有骨溶解(即骨质磨损),您的外科医生可能会建议您调整活动方式。物理治疗的目的是增强肩部周围的肌肉,以提供关节支持。保守治疗和手术治疗对于管理肩锁关节骨关节炎均有效。请给予这种非手术治疗充分的机会,因为它对大多数患有该区域疼痛症状的患者都有帮助。
如果疼痛持续存在,您的外科医生可能会讨论药物治疗方案。这通常包括使用止痛药和抗炎药来减轻肿胀和不适。您也可以考虑进行肩锁关节注射。对于肩锁关节骨关节炎患者,这些注射的1年成功率为47%。注射可直接在关节部位减轻炎症和疼痛。目前仍在研究比较不同类型的类固醇注射,以确定哪种对孤立性关节疼痛最有效。虽然部分患者能获得持久的缓解,但如果注射效果消退,其他患者可能需要探索其他选择。
当保守治疗达到极限且疼痛继续影响您的日常生活时,就会考虑手术治疗。开放和关节镜下切除成形术技术均能为有症状的肩锁关节骨关节炎提供可预测的疼痛缓解。该手术涉及切除锁骨的一小部分,以创造更多空间并减少摩擦。对于对保守治疗无反应的患者,有限的远端锁骨切除术可在中期随访中减轻疼痛并改善肩部功能。您的外科医生将根据您的具体症状和影像学结果判断您是否适合该手术。对某些患者而言,这种简单的骨组织切除足以恢复舒适感和活动度,而无需进行更复杂的重建。
预期情况¶
如果您被诊断为肩锁(AC)关节的退行性关节炎但无疼痛,这种情况很可能保持不变。在90%的患者中,无症状的AC骨关节炎在7年期间保持无症状。如果这一发现并未给您带来困扰,您无需为此担心。即使没有症状,在影像学检查中看到关节炎的迹象也很常见。
如果您有疼痛,预后取决于您如何管理它。关节内注射的成功率在1年内为47%。这意味着近一半的患者通过这种治疗获得了持久的缓解。如果注射无效,您的外科医生可能会建议进行切除部分锁骨的手术。对于对保守治疗无反应的患者,这种有限的远端锁骨切除术可在中期随访中减轻疼痛并改善肩部功能。
如果您选择手术,可以预期获得可预测的疼痛缓解。开放和关节镜切除技术均可提供这种缓解。然而,每种方法都有其独特的潜在并发症组合。您的外科医生将根据您的具体解剖结构和生活方式讨论哪种方法最合适。
如果不治疗有症状的关节炎,它可能会持续存在。一些患者经历持续的不适,限制了日常活动。如果您接受其他肩部手术,如肩袖修复术,未治疗的AC关节骨关节炎与较低的失败率相关。然而,骨关节炎通常与肩袖修复术后较差的最终临床结果相关。未愈合或再次撕裂的肩袖也会增加患此关节炎的风险。
对于严重病例,特别是如果您正在进行反式肩关节置换术,严重的AC关节骨关节炎与肩峰应力性骨折相关。接受此类手术的患者中,影像学上的AC关节骨关节炎很常见。您的外科医生将密切监测这些风险。
总体而言,AC关节关节炎的病程各不相同。它可能通过保守治疗得到缓解,尽管治疗仍持续存在,或缓慢进展。大多数患者发现,针对性治疗可显著改善功能和舒适度。
何时就医¶
若休息后疼痛仍持续不缓解,请咨询您的全科医生。若发现肩部无力或不稳,请要求专科医生评估。若关节出现交锁或错动感,请及时就医。若症状干扰您的睡眠或工作,请联系您的外科医生。疼痛突然加重也是寻求医疗帮助的理由。请注意,无症状的磨损性关节炎通常可在七年内保持无痛。然而,未经治疗的问题有时可能影响其他肩部修复手术的效果。您的医生将检查是否有压痛,并讨论注射治疗是否可能带来帮助。早期评估可确保您在病情进展前获得适当的治疗。
Evidence & references
Overview¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis [8].
- Open and arthroscopic resection arthroplasty techniques have unique sets of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique [8].
- Limited distal clavicle excision reduced pain and improved shoulder function at midterm follow-up in patients with AC joint osteoarthritis resistant to conservative treatment [9].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair [3].
- Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results [5].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete AC dislocations [21].
Anatomy & Pathophysiology¶
- Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation [10].
- None of the reconstruction strategies completely restored the shoulder girdle to its preinjured state [26].
- Kinematic changes resulting from AC joint dislocation could be a potential source of pain and dysfunction in the shoulder [27].
- Scapular and clavicular kinematics were affected in AC separation models [28].
- The position of the hook portion of a clavicle hook plate can predispose anatomic structures to post-operative complications of subacromial impingement and bony erosion [29].
- Future research should focus on addressing horizontal and rotational instability to restore native physiological and biomechanical properties of the AC joint [35].
- Coracoclavicular reconstruction with augmentation of the acromioclavicular joint provides improved horizontal stability compared to isolated coracoclavicular reconstruction [41].
- Adding a fixation of the AC joint minimizes lateral tilting of the scapula and maintains a more anatomic reposition result over time [45].
Classification¶
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Mild arthroscopic findings of acromioclavicular joint osteoarthritis may be clinically significant and warrant resection, but further characterization of such patients is needed [1].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic acromioclavicular joint osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity of the joint but did not correlate with clinical results [11].
- The acromial center line to dorsal clavicle radiographic measurement and the use of the Alexander view provide a more realistic appreciation of true acromioclavicular joint displacement, especially in defining watershed cases (Rockwood types IIIA, IIB, and IV) [12].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the acromioclavicular joint is reproducible and provides additional information on the severity of the injury [24].
- Injuries to the sternoclavicular joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae [16].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
Clinical Presentation¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Osteolytic changes seemed to be associated with incongruity of the AC joint, but did not correlate with clinical results [11].
- Additional research is needed to determine the main cause of pain in isolated acromioclavicular osteoarthritis and to compare clinical outcomes of intra-articular versus extra-articular injections [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness to palpation, female sex, dominant side surgery) [18].
- Recurrence of the initial dislocation after arthroscopically assisted reduction appears to be related to the onset of degenerative ACJ arthropathy [14].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder [4].
Investigations¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection (DCR) is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterization is needed to determine which patients with mild arthroscopic findings of AC joint OA are clinically significant and warrant resection [1].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty (RSA) [7].
- Severe ACJ osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Osteolytic changes in the AC joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Patients with edema on MRI were more likely to present with pain than patients without edema [43].
- Subchondral bone edema on histologic examination was more frequent in patients with pain [43].
- The outcomes of a preoperative AC injection suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome [6].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated AC osteoarthritis [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness, female sex, dominant side) [18].
- The arthroscopic approach offers an advantage in diagnosing and treating occult intra-articular pathology during distal clavicle excision [20].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder using arthroscopy [4].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and provides additional information on injury severity, which may influence treatment decisions [24].
- The AC-DC measurement and use of the Alexander view provide a more realistic appreciation of true AC joint displacement, particularly in defining watershed cases (IIIA/IIB/IV) [12].
- Radiological failures were observed in 41% of cases in a prospective multicenter study of arthroscopic acute AC dislocation fixation [50].
Treatment¶
Non-Operative Management¶
- Conservative therapy is a valid initial treatment option for Rockwood Type V acromioclavicular dislocations [15].
- Non-operative reduction and stabilization is a valuable treatment option for acute high-grade acromioclavicular joint separations [33].
- Nonoperative treatment is helpful for most patients with painful conditions of the acromioclavicular joint, although those with osteolysis may need to modify their activities [44].
- Conservative and surgical treatments are both effective in the management of acromioclavicular joint osteoarthritis [17].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated acromioclavicular osteoarthritis [13].
Operative Management¶
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic acromioclavicular osteoarthritis [8].
- Limited distal clavicle excision reduces pain and improves shoulder function at midterm follow-up in patients with acromioclavicular joint osteoarthritis resistant to conservative treatment [9].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Further characterization is needed to identify patients in whom mild arthroscopic findings of acromioclavicular joint osteoarthritis are clinically significant and warrant resection [1].
- Conversion to anatomic coracoclavicular ligament reconstruction shows similar clinical outcomes compared to successful non-operative treatment in chronic primary type III to V acromioclavicular joint injuries at a minimum 5-year follow-up [49].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete acromioclavicular dislocations [21].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair, and an unhealed or re-torn cuff increases the risk of osteoarthritis [23].
Diagnostic Considerations¶
- A distinction between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis appears unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year course [2].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in the revision of failed open anterior stabilization of the shoulder [4].
Complications¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair [23].
- An unhealed or re-torn rotator cuff increases the risk of developing osteoarthritis [23].
- Severe AC joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in revision of failed open anterior stabilization of the shoulder [4].
- Recurrence of the initial dislocation after arthroscopically assisted reduction of acute AC joint dislocation appears to be related to the onset of degenerative ACJ arthropathy [14].
- Treatment of acute grade III and IV AC dislocations by synthetic ligament reconstruction carries a risk of significant early osteolysis [25].
- Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, complication rate, or revision rate [38].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis but each has a unique set of potential complications [8].
Recovery¶
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Limited distal clavicle excision for acromioclavicular joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up [9].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- A preoperative acromioclavicular injection study suggested that distinguishing between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis is unnecessary, as all patients were equally satisfied with the outcome [6].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Recurrence of initial acromioclavicular joint dislocation appears to be related to the onset of degenerative acromioclavicular joint arthropathy [14].
- Treatment of acute grade III and IV acromioclavicular dislocations using synthetic ligament reconstruction gave satisfactory results in terms of recovery of strength, but evolution is not risk-free due to the onset of significant early osteolysis [25].
- Arthroscopic coracoclavicular ligament reconstruction with double-bundle soft tissue allograft for chronic type V acromioclavicular dislocations showed sustained and statistically significant improvements in functional outcomes, high rates of return to sport, and maintenance of active-duty military status at minimum 10-year follow-up [39].
- Minimally invasive coracoclavicular ligament augmentation with a flip button/polydioxanone repair for total acromioclavicular joint dislocation revealed excellent radiologic and clinical results with no subluxations or dislocations noted in short-term follow-up [48].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
- Type V acromioclavicular dislocations may be given a trial of conservative therapy [15].
Key Evidence¶
- [L2] Further characterisation of patients in whom mild arthroscopic findings of OA of AC joint are clinically significant and warrant resection is needed. [1] (10.1007/s00167-014-3114-2)
- [L2] Asymptomatic AC-OA remained asymptomatic in 90% over 7 years. [2] (10.1016/j.jse.2019.04.004)
- [L2] Untreated ACJ osteoarthritis, symptomatic or not, encountered during arthroscopic RCR is associated with a low percentage of failure. [3] (10.1007/s00167-020-06098-y)
- [L4] Some persistent pain and osteoarthritis progression remain concerns. [4] (10.1016/j.arthro.2009.04.073)
- [L3] Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results. [5] (10.1177/0363546519862850)
- [L4] The outcomes of this study seem to suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome. [6] (10.5397/cise.2023.00073)
- [L3] Radiographic ACJ osteoarthritis is common in patients undergoing RSA. [7] (10.1016/j.jseint.2021.11.008)
- [L5] Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis, though each has a unique set of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique. [8] (10.1177/0363546513485359)
- [L4] Limited distal clavicle excision of patients with AC joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up. [9] (10.1016/j.otsr.2016.01.008)
- [L5] Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation. [10] (10.1016/j.arthro.2019.01.038)
- [L4] The AC-DC measurement and use of the Alexander view provides the clinician with a more realistic appreciation of true AC joint displacement, especially in defining watershed cases (ie, IIIA/IIB/IV) and may better inform the decision-making process regarding management options and recommendations. [12] (10.1016/j.jse.2019.12.014)
- [L4] Additional research is needed to determine the main cause of pain and compare clinical outcomes of intra-articular versus extra-articular injections. [13] (10.5397/cise.2023.00311)
- [L4] Recurrence of the initial dislocation appears to be related to onset of degenerative ACJ arthropathy. [14] (10.1016/j.otsr.2017.11.001)
- [L4] This suggests that Type V AC dislocations may be given a trial of conservative therapy. [15] (10.1177/2325967115s00017)
- [L1] Injuries to the SC joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae. [16] (10.1177/0363546513498990)
- [L4] Conservative and surgical treatments are both effective in acromioclavicular joint osteoarthritis management. [17] (10.1007/s00167-020-06377-8)
- [L3] Risk factors for subsequent DCE included tenderness to palpation at the AC joint, female sex, and surgery on the dominant side, with subsequent DCE performed in 40% of cases with a combination of these 3 factors. [18] (10.1177/2325967119844295)
- [L1] Preventive arthroscopic DCR is not recommended in patients with radiological but asymptomatic ACJ arthritis. [19] (10.1177/0363546514547254)
- [L1] The arthroscopic approach offers a unique advantage in diagnosing and treating occult intra-articular pathology. [20] (10.1016/j.jse.2006.10.006)
- [L4] The authors recommend this procedure for the treatment of chronic complete AC dislocations. [21] (10.1016/j.injury.2010.09.023)
- [L4] AC injections offer a 1-year success rate of 47%. [22] (10.5397/cise.2023.00031)
- [L4] Osteoarthritis is associated with poorer final clinical outcomes, and an unhealed or re-torn cuff increases the risk of osteoarthritis. [23] (10.1016/j.otsr.2017.03.007)
- [L1] Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and gives additional information on the severity of the injury, which might also influence the treatment decision. [24] (10.1016/j.jse.2020.10.026)
- [L4] Treatment of ACD by synthetic ligament reconstruction gave satisfactory results, notably in terms of recovery of strength, but evolution is not risk-free with onset of significant early osteolysis. [25] (10.1016/j.otsr.2010.06.004)
- [L5] Although each technique was able to restore different elements of the joint kinematics, none of the strategies completely restored the shoulder girdle to its preinjured state. [26] (10.1177/03635465221095231)
- [L5] The kinematic changes could be a potential source of pain and dysfunction in the shoulder with AC joint dislocation. [27] (10.1177/0363546512458571)
- [L5] Scapular and clavicular kinematics were affected in AC separation models. [28] (10.1016/j.jse.2013.01.004)
- [L5] The observed frequency of hook contact with surrounding subacromial structures in a static shoulder confirms that the position of the hook portion of the implant can predispose anatomic structures to the post-operative complications of subacromial impingement and bony erosion. [29] (10.1016/j.injury.2009.12.012)
- [L4] Non-operative reduction and stabilization of high-grade AC joint separations seems to be a valuable treatment option. [33] (10.1007/s00402-020-03630-0)
- [L5] Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint. [35] (10.1186/s12891-022-05935-0)
- [L1] Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, the complication rate, and the revision rate based on the available literature. [38] (10.1177/0363546518795147)
- [L4] Outcomes after arthroscopic CC reconstruction for chronic, type V AC dislocations in an active-duty military patient population show sustained and statistically significant improvements in functional outcomes as well as high rates of return to sport and maintenance of active-duty military status at long-term follow-up. [39] (10.1016/j.arthro.2025.05.008)
- [L1] Coracoclavicular reconstruction with augmentation of the acromioclavicular joint has been shown to provide improved horizontal stability in both biomechanical and clinical studies compared to isolated coracoclavicular reconstruction. [41] (10.1007/s00167-018-5152-7)
- [L4] Patients with edema on MRI were more likely to present pain than patients without edema, and subchondral bone edema on histologic examination was more frequent in patients with pain. [43] (10.1016/j.jseint.2020.03.007)
- [L5] Nonoperative treatment is helpful for most patients, although those with osteolysis may have to modify their activities. [44] (10.5435/00124635-199905000-00004)
- [L3] The presented data suggest adding a fixation of the AC joint to minimize lateral tilting of the scapula and maintain a more anatomic reposition result over time. [45] (10.1007/s00402-021-03761-y)
- [L4] The short-term follow-up of 15 recently operated patients reveals excellent radiologic and clinical results, with no subluxations or dislocations of the acromioclavicular joint noted. [48] (10.1016/j.arthro.2006.12.015)
- [L4] At a minimum 5-year follow-up, patients with successful non-operative treatment for type III-V ACJ injuries achieved similar clinical outcomes compared to those who were converted to ACCR. [49] (10.1007/s00167-020-06159-2)
- [L4] Surgery for AC dislocations is difficult with radiological results that must still be improved, as radiological failures were observed in 41% of cases. [50] (10.1016/j.otsr.2015.09.012)
References¶
[1] Outcome of distal clavicle resection in patients with acromioclavicular joint osteoarthritis and full‐thickness rotator cuff tear. Knee Surgery, Sports Traumatology, Arthroscopy. 2014. DOI: 10.1007/s00167-014-3114-2 [2] Seven-year course of asymptomatic acromioclavicular osteoarthritis diagnosed by MRI. Journal of Shoulder and Elbow Surgery. 2019. DOI: 10.1016/j.jse.2019.04.004 [3] Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06098-y [4] The Role of Arthroscopy in Revision of Failed Open Anterior Stabilization of the Shoulder. Arthroscopy. 2009. DOI: 10.1016/j.arthro.2009.04.073 [5] Factors Predicting the Outcome After Arthroscopically Assisted Stabilization of Acute High-Grade Acromioclavicular Joint Dislocations. The American Journal of Sports Medicine. 2019. DOI: 10.1177/0363546519862850 [6] Diagnostic value of a preoperative acromioclavicular injection for symptomatic acromioclavicular osteoarthritis: a retrospective study of cross-sectional midterm outcomes. Clinics in Shoulder and Elbow. 2024. DOI: 10.5397/cise.2023.00073 [7] Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty. JSES International. 2022. DOI: 10.1016/j.jseint.2021.11.008 [8] Degenerative Joint Disease of the Acromioclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513485359 [9] Limited distal clavicle excision of acromioclavicular joint osteoarthritis. Orthopaedics & Traumatology: Surgery & Research. 2016. DOI: 10.1016/j.otsr.2016.01.008 [10] Editorial Commentary: Why We Have To Respect The Anatomy In Acromioclavicular Joint Surgery And Why Clinical Shoulder Scores Might Not Give Us The Information We Need!. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2019.01.038 [11] 10.1016-0020-1383-83-90092-x. n.d.. [12] Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.12.014 [13] Isolated acromioclavicular osteoarthritis and steroid injection. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00311 [14] Arthroscopically assisted reduction of acute acromioclavicular joint dislocation using a single double-button device: Medium-term clinical and radiological outcomes. Orthopaedics & Traumatology: Surgery & Research. 2018. DOI: 10.1016/j.otsr.2017.11.001 [15] Successful Conservative Therapy in Rockwood Type V Acromioclavicular Dislocations. Orthopaedic Journal of Sports Medicine. 2015. DOI: 10.1177/2325967115s00017 [16] Instability and Degenerative Arthritis of the Sternoclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513498990 [17] No differences between conservative and surgical management of acromioclavicular joint osteoarthritis: a scoping review. Knee Surgery, Sports Traumatology, Arthroscopy. 2021. DOI: 10.1007/s00167-020-06377-8 [18] Preoperative Factors Associated With Subsequent Distal Clavicle Resection After Rotator Cuff Repair. Orthopaedic Journal of Sports Medicine. 2019. DOI: 10.1177/2325967119844295 [19] Is Arthroscopic Distal Clavicle Resection Necessary for Patients With Radiological Acromioclavicular Joint Arthritis and Rotator Cuff Tears?. The American Journal of Sports Medicine. 2014. DOI: 10.1177/0363546514547254 [20] Arthroscopic versus open distal clavicle excision: Comparative results at six months and one year from a randomized, prospective clinical trial. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.10.006 [21] Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction. Injury. 2010. DOI: 10.1016/j.injury.2010.09.023 [22] Mid- to long-term success rate and functional outcomes of acromioclavicular injections in patients with acromioclavicular osteoarthritis. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00031 [23] Osteoarthritis after rotator cuff repair: A 10-year follow-up study. Orthopaedics & Traumatology: Surgery & Research. 2017. DOI: 10.1016/j.otsr.2017.03.007 [24] The ligamentous injury pattern in acute acromioclavicular dislocations and its impact on clinical and radiographic parameters. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2020.10.026 [25] Acute grade III and IV acromioclavicular dislocations: Outcomes and pitfalls of reconstruction procedures using a synthetic ligament. Orthopaedics & Traumatology: Surgery & Research. 2010. DOI: 10.1016/j.otsr.2010.06.004 [26] Differences between Coracoclavicular, Acromioclavicular, or Combined Reconstruction Techniques on the Kinematics of the Shoulder Girdle. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465221095231 [27] The Function of the Acromioclavicular and Coracoclavicular Ligaments in Shoulder Motion. The American Journal of Sports Medicine. 2012. DOI: 10.1177/0363546512458571 [28] Acromioclavicular joint ligamentous system contributing to clavicular strut function: a cadaveric study. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.004 [29] Subacromial morphometric assessment of the clavicle hook plate. Injury. 2010. DOI: 10.1016/j.injury.2009.12.012 [33] Can an acute high-grade acromioclavicular joint separation be reduced and stabilized without surgery? A surgeon’s experience. Archives of Orthopaedic and Trauma Surgery. 2020. DOI: 10.1007/s00402-020-03630-0 [35] Current concepts in acromioclavicular joint (AC) instability – a proposed treatment algorithm for acute and chronic AC-joint surgery. BMC Musculoskeletal Disorders. 2022. DOI: 10.1186/s12891-022-05935-0 [38] Current Concepts in the Operative Management of Acromioclavicular Dislocations: A Systematic Review and Meta-analysis of Operative Techniques. The American Journal of Sports Medicine. 2018. DOI: 10.1177/0363546518795147 [39] Arthroscopic Coracoclavicular Ligament Reconstruction With Double‐Bundle Soft Tissue Allograft for Chronic Type V Acromioclavicular Dislocations Shows Excellent Patient Outcomes and Return to Duty and Sport at Minimum 10‐Year Follow‐Up. Arthroscopy. 2025. DOI: 10.1016/j.arthro.2025.05.008 [41] Acromioclavicular joint augmentation at the time of coracoclavicular ligament reconstruction fails to improve functional outcomes despite significantly improved horizontal stability. Knee Surgery, Sports Traumatology, Arthroscopy. 2018. DOI: 10.1007/s00167-018-5152-7 [43] Histologic and magnetic resonance image evaluation in acromioclavicular joint osteoarthritis. JSES International. 2020. DOI: 10.1016/j.jseint.2020.03.007 [44] Painful Conditions of the Acromioclavicular Joint. Journal of the American Academy of Orthopaedic Surgeons. 1999. DOI: 10.5435/00124635-199905000-00004 [45] Additional acromioclavicular cerclage limits lateral tilt of the scapula in patients with arthroscopically assisted coracoclavicular ligament reconstruction. Archives of Orthopaedic and Trauma Surgery. 2021. DOI: 10.1007/s00402-021-03761-y [48] Minimally Invasive Coracoclavicular Ligament Augmentation With a Flip Button/Polydioxanone Repair for Treatment of Total Acromioclavicular Joint Dislocation. Arthroscopy. 2007. DOI: 10.1016/j.arthro.2006.12.015 [49] Conversion to anatomic coracoclavicular ligament reconstruction (ACCR) shows similar clinical outcomes compared to successful non‐operative treatment in chronic primary type III to V acromioclavicular joint injuries. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06159-2 [50] Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation. Prospective multicenter study of 116 cases. Orthopaedics & Traumatology: Surgery & Research. 2015. DOI: 10.1016/j.otsr.2015.09.012