Patients › Wrist
腕关节部分融合术(四角融合及头钩骨融合术)
Patient-facing topic for four-corner and capitolunate (two-corner) fusion of the wrist — joint-preserving alternative to total wrist fusion that retains some bending motion.
为何建议进行此手术¶
您的外科医生建议您进行部分腕关节融合术(也称为四角融合术或头钩骨融合术),以治疗腕部严重的磨损性关节炎。当非手术治疗未能提供足够的缓解,且您的特定关节损伤涉及头钩骨区域时,通常会提供此手术。该手术旨在通过将剩余的骨骼融合在一起,从而缓解疼痛并提供稳定性。
此手术的主要目标是为您提供可靠、持久的功能,并确保长期稳定。通过移除受损骨骼并连接其他骨骼,该手术旨在消除导致疼痛的摩擦,同时尽可能保留活动度。与全腕关节置换术或更广泛的融合术相比,这种方法提供了一种强有力的替代方案,有助于您在减少不适的情况下恢复日常活动。
手术前¶
您的外科医生可能会在手术前安排X光、血液检查或MRI,以检查您的手腕和整体健康状况。您需要在手术前禁食数小时,并停止服用某些药物,具体请遵循外科医生的指示。请安排朋友或家人开车送您回家,因为您不能自己开车。请携带一份当前所有药物的完整清单,并穿着舒适、宽松的衣服前往医院。该手术通过手腕背侧的单一切口进行。您的手术团队将直接与您在所有具体指示方面进行详细讨论。
手术当天¶
您将抵达医院,并与麻醉医师会面,讨论您的治疗方案。该手术将在全身麻醉下进行。在手术过程中,您将完全处于睡眠状态。部分患者可能还会接受区域神经阻滞以缓解术后疼痛;麻醉医师将根据您的具体情况在手术当天决定是否需要。
您的外科医生将通过手腕处的单个开放切口进行手术。随后,您将被移至复苏区,安全地苏醒。在麻醉效果逐渐消退期间,您将接受密切监测。
手术内容¶
您的外科医生将在手腕背侧做一个切口以到达关节。这种开放入路可直接进入内部骨骼。根据您的具体关节炎类型,外科医生可能会切除舟骨,或使用特殊植入物对头状骨进行表面置换。
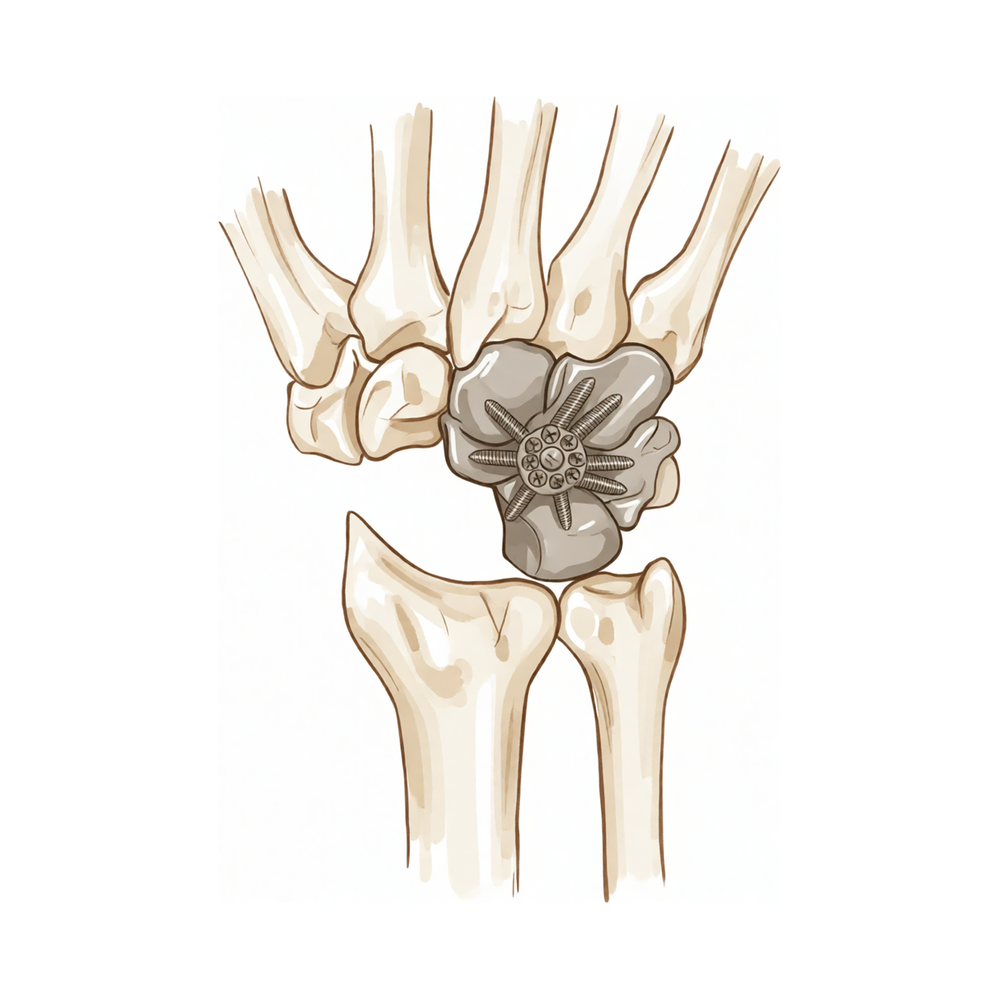
接下来,外科医生将准备用于融合的关节面。如果您接受的是四角融合术,外科医生会切除舟骨,并将剩余的腕骨连接在一起。对于头状骨-月骨融合术,仅连接头状骨和月骨。外科医生会使用螺钉、 staples 或金属板将这些骨骼牢固固定,以促进愈合。可能会添加局部骨移植以帮助骨骼融合。
最后,外科医生用缝线闭合切口并敷上敷料。该手术的目标是在尽可能保留剩余关节活动度的同时,创建一个稳定且无痛的手腕。此手术适用于其他治疗无效的晚期关节炎手腕。
术后¶
您将在恢复室苏醒,您的医疗团队将为您管理疼痛。您的外科医生将在您的手腕处做一个单一的开放切口。您将带着厚厚的敷料和吊带或支具离开,以保护您的手腕。大多数患者在此手术后需要在医院过夜,但有些人可以在当天回家。您必须有人在最初的24小时内陪伴您,以帮助您。您将立即开始轻柔地活动手指。您的外科医生将指导您如何护理伤口以及何时重新开始使用您的手。
恢复¶
开放手术后,您的手腕和手部可能会出现疼痛和肿胀。这是身体愈合过程中的正常现象。您的外科医生将指导您如何通过药物和冰敷来管理这种不适。您将佩戴石膏或夹板,以保护正在融合的骨骼。
在术后初期,您需要抬高患肢以减轻肿胀。在室内活动时,您将使用吊带提供支撑。小心谨慎的情况下,可以进行吃饭或刷牙等简单日常活动。您的物理治疗师将教您轻柔的练习,以保持手指活动并防止僵硬。随着肿胀消退和活动度恢复,您将逐渐开始更多地使用手部。
您的外科医生和物理治疗师将指导您何时停止使用夹板以及如何增强握力。您的恢复时间可能与他人不同;您的外科医生和物理治疗师将根据您的愈合情况提供指导。随着疼痛减轻和手腕变得稳定,您将感到更加自信。
可能出现的问题¶
大多数患者恢复良好,但偶尔也会出现并发症。您的外科医生和医疗团队会密切监测您,以便尽早发现任何问题。
有时骨骼未能按预期愈合。您可能会感到剧烈疼痛,且普通止痛药无法缓解,或感觉手腕仍然不稳定。如果出现这种情况,请联系您的外科医生讨论后续步骤。
存在较小的可能性,关节日后可能需要完全融合。您可能会感到僵硬或疼痛逐渐加重,或在一段改善期后疼痛复发。您的外科医生将复查您的X光片,并在必要时与您讨论转为全腕关节融合术。
在某些情况下,骨移植材料或螺钉可能未能达到预期效果。您可能会感到手腕内有咔哒声或研磨感,或注意到突然出现的肿胀和压痛。请在下次复诊时提出此情况,以便您的外科医生检查内固定物。
如果您使用的是热解碳植入物,其长期效果可能难以预测。您可能会随着时间的推移出现疼痛或活动度丧失。如果植入物失效,融合手术仍是解决问题的可选方案。
本页面底部的并发症表格列出了典型的发生率,如需具体数据请查阅。
何时联系我们¶
如果您出现发热、伤口红肿加重或渗出,请立即联系我们。若出现突发剧烈疼痛或手部感觉丧失,请立即联系您的外科医生。如发现小腿肿胀或呼吸困难,请前往急诊就医。这些症状可能提示存在需要紧急处理的血栓或感染。
Evidence & references
Overview¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- The use of a pyrocarbon capitate resurfacing implant may represent a good alternative to total and partial wrist arthrodesis [3].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up [4].
- There are no comparative series or randomized studies for the treatment of midcarpal instability [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- The reduction and association of the scaphoid and lunate procedure should be abandoned due to a majority of patients experiencing early radiographic failure in the short term [7].
- It is difficult to predict long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, but the outcome so far is encouraging [9].
- Conversion to midcarpal fusion remains a salvage option for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis [9].
- Radioscapholunate arthrodesis with compression screws and local autograft is an effective method to perform the procedure in appropriately selected patients with a preserved midcarpal joint [11].
- Radioscapholunate arthrodesis with compression screws and local autograft achieves a 100% union rate at mean follow-up of 12 months with no complications [11].
- Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions [13].
- The use of magnesium-based headless bone screws for partial wrist arthrodesis is not supported due to premature mechanical instability [15].
- Radial wrist hemiarthroplasty implants are not approved by the FDA for use in humans in the United States [23].
- Radial wrist hemiarthroplasty implants must be performed as off-label use with full patient understanding and appropriate institutional review board approval [23].
Anatomy & Pathophysiology¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- A dart-throwing motion (DTM) at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion [10].
- Surgical groups for scapholunate advanced collapse demonstrate decreased wrist kinematic motion and functional performance compared with individuals with normal wrists [16].
- Scaphoid nonunions partially uncouple the proximal and distal carpal rows [17].
- Computed fiber elongations of the dorsal carpal ligaments vary linearly with wrist position [29].
- During simple unresisted wrist motions, force in the scapholunate interosseous ligament does not exceed 20 N [30].
- Kinematic changes in scapholunate instability may predict the development of radioscaphoid arthritis [31].
- Comprehending carpal dysfunctions and instabilities hinges on understanding carpal anatomy and normal biomechanics [32].
- The distal carpal row has negligible intercarpal motion while the proximal row drives motion [33].
- More than half the motion of the carpus when the wrist was loaded in extension occurred at the midcarpal joint [34].
- Static imaging techniques may accurately depict major wrist ligamentous injury, while dynamic ultrasound and videofluoroscopy may demonstrate dynamic instability and kinematic dysfunction [35].
- A pattern of kinematic changes was established after scapholunate ligament injury despite individual variance [38].
- Accurate identification of carpal bone morphology is required to improve understanding of carpal mechanics and pathology [39].
- A wide range of dart-throwing motion planes exists [40].
- Midcarpal arthrodesis adversely affects dart-throwing motion compared with radiocarpal arthrodesis [40].
- During forearm rotation, the contact site of the scaphoid and the lunate on the distal radial articular surface changed minimally [41].
- Reconstruction of both volar and dorsal limbs of the scapholunate interosseous ligament aims to approximate original anatomy and restore normal carpal mechanics [42].
Classification¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- The use of a pyrocarbon capitate resurfacing implant may represent a good alternative to total and partial wrist arthrodesis [3].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up [4].
- There are no comparative series or randomized studies for midcarpal instability treatment options including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- Functional results were good at long-term follow-up for 4-corner fusion for SLAC and SNAC wrist despite radiographic changes in the radiolunate joint in 73% of patients [8].
- Scaphoid nonunions have a dramatic impact on carpal kinematics, partially uncoupling the proximal and distal carpal rows [17].
- Simulated radiocarpal fusion and simulated partial carpal fusion decreased range of motion compared with the intact wrist [53].
- The principal direction of wrist motion along the path of dart-thrower's motion was not significantly altered by simulated radiocarpal fusion or partial carpal fusion [53].
- The LFT and MFT demonstrate similar congruity to the proximal capitate in the sagittal and coronal planes of the wrist [56].
- Simulated radioscapholunate fusion confirmed the dart-thrower's hypothesis as wrist motion was primarily preserved from radial-extension toward ulnar-flexion [59].
- Midcarpal stabilisation and scaphoid and triquetrum excision retains most wrist motion [60].
Clinical Presentation¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- Treatment options for midcarpal instability include partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage [4].
- There are no comparative series or randomized studies regarding treatment options for midcarpal instability [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse [6].
- The reduction and association of the scaphoid and lunate procedure experiences early radiographic failure in the majority of patients in the short term [7].
- Functional results for 4-corner fusion for SLAC and SNAC wrist are good at long-term follow-up despite radiographic changes in the radiolunate joint in 73% of patients [8].
- It is difficult to predict long-term survival for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, though outcomes are currently encouraging [9].
- Conversion to midcarpal fusion remains a salvage option for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis [9].
- A dart-throwing motion (DTM) at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion [10].
- Lunate excision without midcarpal fusion resulted in a disease-free state with good painless range of motion at 6 years [12].
- Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions [13].
- Radiographic carpal collapse and ulnar translocation occurred in scaphocapitate arthrodesis for Kienböck disease, but patients were not symptomatic [19].
- From an 8- to 11-year perspective, patients with distal scaphoid fractures report normal self-assessed hand function as well as good wrist motion and strength [20].
- Parallel K-wire placement across the midcarpal joints with scaphoid leads to a high rate of fusion with good patient outcomes long term [21].
- Ulnar-sided wrist pain is a common cause of upper extremity disability with a complex differential diagnosis [43].
- Both trigger wrist and avascular necrosis of the capitate are rare disorders [49].
- Excision arthroplasty for scapho-trapezial-trapezoid (STT) arthritis can provoke severe malalignment and midcarpal instability [50].
- Midcarpal instability following excision arthroplasty for STT arthritis can lead to an intercarpal arthrodesis with an outcome potentially worse than STT fusion [50].
Investigations¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up [4].
- There are no comparative series or randomized studies regarding treatment options for midcarpal instability [4].
- A dynamic CT scan of the wrist is a user-friendly way of measuring the scapholunate distance, which is minimal in the normal wrist below 40 years of age [57].
- Measurements in the middle of the scapholunate joint in neutral and 30° of ulnar deviation under fluoroscopic imaging best capture all stages of ligamentous disruptions [63].
- Plain radiographs, CT, 3D-CT, and MRI are suboptimal modalities to assess capitate type [64].
- A scaphoid fracture was by far the most common injury in patients with posttraumatic radial wrist tenderness, but it is not clear whether diagnosis of subtle injuries only demonstrated on MRI improves outcomes [62].
- Delayed diagnosis and late reconstructive surgery for traumatic nondissociative carpal instability were associated with no improvement in radiolunate angle [58].
- Delayed diagnosis of intercarpal injuries can result in persistent median nerve dysfunction [27].
Treatment¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- The use of a pyrocarbon capitate resurfacing implant may represent a good alternative to total and partial wrist arthrodesis [3].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up, but there are no comparative series or randomized studies [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- The reduction and association of the scaphoid and lunate procedure should be abandoned due to a majority of patients experiencing early radiographic failure in the short term [7].
- It is difficult to predict long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, but the outcome so far is encouraging, and conversion to midcarpal fusion remains a salvage option [9].
- Radioscapholunate arthrodesis with compression screws and local autograft is an effective method in appropriately selected patients with a preserved midcarpal joint, achieving a 100% union rate at mean follow-up of 12 months with no complications [11].
- Lunate excision without midcarpal fusion resulted in a disease-free state with good painless range of motion at 6 years, avoiding the recurrence associated with curettage and the motion loss associated with fusion [12].
- Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions [13].
- The results after total wrist joint arthroplasty vary probably as the result of different patient groups, implant types and evolution of prosthetic designs, and are not comparable with the present study [14].
- The authors cannot support the use of magnesium-based screws for partial wrist arthrodesis due to premature mechanical instability [15].
- Load is preferentially transferred to the radiolunate joint after scaphoid excision with four-corner fusion [22].
- Radial wrist hemiarthroplasty implants are not approved by the FDA for use in humans in the United States and must be performed as off-label use with full patient understanding and appropriate institutional review board approval [23].
- Arthroscopic resection of the proximal capitate with tendon interposition for isolated capitolunate osteoarthritis does not preclude the possibility of secondary arthrodesis in case of failure [24].
- Better results were seen when arthrodesis fused in cases of avascular necrosis of the capitate [25].
- The technique of wrist arthrodesis combining proximal row carpectomy and rigid internal fixation has proved to be a highly predictable operation with much less morbidity and fewer complications than with older techniques using distant bone graft [48].
- Radiocarpal fusion aims to alleviate pain and improve range of motion in patients with isolated radiolunate or radioscapholunate arthritis who have failed non-surgical treatment [51].
- Pyrocarbon interposition arthroplasty is an alternative to total wrist arthrodesis when marked degenerative changes exist at the radiolunate joint, capitate head or both, and increases operative options for challenging clinical scenarios [52].
- Locking screws are important in improving the longevity of total wrist arthroplasty by imitating external or internal fixation for bridging large bony defects, allowing the carpal component to remain stable despite complete asymptomatic avascular bone necrosis around the capitate peg [55].
- Arthroscopic interposition tendon arthroplasty for stage 2 scapholunate advanced collapse preserves motion, yields acceptable functional outcome, and reduces pain [61].
- Arthroscopic partial capitate resection for type Ia avascular necrosis provided adequate pain relief and improved the range of wrist motion and grip strength during short-term follow-up [67].
Complications¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients receiving vascularized bone graft with capitate shortening and radial shortening [2].
- Treatment options for midcarpal instability, including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage, are described in small case series with limited follow-up without comparative series or randomized studies [4].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse [6].
- The reduction and association of the scaphoid and lunate procedure experiences early radiographic failure in the majority of patients in the short term [7].
- Radiographic changes in the radiolunate joint occur in 73% of patients at long-term follow-up despite good functional results after 4-corner fusion for SLAC and SNAC wrist [8].
- Long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis is difficult to predict, though conversion to midcarpal fusion remains a salvage option [9].
- Radioscapholunate arthrodesis with compression screws and local autograft achieves a 100% union rate at a mean follow-up of 12 months with no complications in appropriately selected patients [11].
- Magnesium-based headless bone screws can result in premature mechanical instability and implant failure in partial wrist fusion [15].
- Parallel K-wire placement across the midcarpal joints with scaphoid leads to a high rate of fusion with good long-term patient outcomes [21].
- Arthroscopic resection of the proximal capitate with tendon interposition does not preclude the possibility of secondary arthrodesis in case of failure [24].
- While some intercarpal arthrodeses yield good, predictable outcomes, others are infrequently used due to unpredictable results and high complication rates [68].
- Wrist fusion rates are higher in the 4-corner fusion group compared to proximal row carpectomy without a significant difference in readmission rates [70].
- Conversion rates to total wrist arthrodesis are significantly higher with partial wrist arthrodesis (19.2%) than with proximal row carpectomy (4.9%) [71].
- Partial wrist arthrodesis has a greater associated direct cost than proximal row carpectomy [71].
- High complication rates following four-corner arthrodesis with a nonlocking plate have led to the recommendation for fixation with a locking screw plate [74].
Recovery¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- Pyrocarbon capitate resurfacing may represent a good alternative to total and partial wrist arthrodesis [3].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- The reduction and association of the scaphoid and lunate procedure should be abandoned due to a majority of patients experiencing early radiographic failure in the short term [7].
- Functional results were good at long-term follow-up for 4-corner fusion for SLAC and SNAC wrist despite radiographic changes in the radiolunate joint in 73% of patients [8].
- It is difficult to predict long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, but the outcome so far is encouraging [9].
- Conversion to midcarpal fusion remains a salvage option for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis [9].
- A dart-throwing motion at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion [10].
- Both surgical groups demonstrated decreased wrist kinematic motion and functional performance compared with individuals with normal wrists [16].
- Further studies need to be performed to address differences in anatomy and wrist movement among patients with different lunate shapes regarding the dart-splint [18].
- From an 8- to 11-year perspective, patients with distal scaphoid fractures report normal self-assessed hand function as well as good wrist motion and strength [20].
- Delayed diagnosis of intercarpal injuries can result in persistent median nerve dysfunction [27].
- Research underscores the importance of considering forearm rotation when developing rehabilitation protocols for scapholunate joint instability [44].
- Radiocapitate range of motion after proximal row carpectomy was sufficient for activities of daily living [45].
- A patient with complex carpal dissociation regained satisfactory function and returned to work at six months with stable carpus on radiographs [46].
- Multicomponent exercise is important in the treatment of wrist instability [47].
- Four-corner bone wrist arthrodesis by dorsal rectangular plating achieves an acceptable preservation of range of motion with good pain relief, an excellent consolidation rate and minimal complications [66].
Key Evidence¶
- [L5] Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics. [1] (10.1177/1558944720966717)
- [L4] Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening. [2] (10.1016/j.jhsg.2019.09.012)
- [L4] This surgical procedure may represent a good alternative to total and partial wrist arthrodesis. [3] (10.1177/1753193413501730)
- [L5] Treatment options including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up, but there are no comparative series or randomized studies. [4] (10.1177/1753193415617756)
- [L4] Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time. [5] (10.1016/j.jhsa.2014.06.118)
- [L4] There is a low rate of conversion to total wrist arthrodesis. [6] (10.1016/j.jhsa.2010.01.025)
- [L4] With a majority of patients experiencing early radiographic failure of the procedure in the short term, our experience suggests that the reduction and association of the scaphoid and lunate procedure should be abandoned despite the relatively low outcomes measures scores. [7] (10.1016/j.jhsa.2014.07.014)
- [L4] Functional results were good at long-term follow-up despite radiographic changes in the radiolunate joint in 73% of patients. [8] (10.1177/1558944716681949)
- [L5] It is difficult to predict long-term survival, but the outcome so far is encouraging, and conversion to midcarpal fusion remains a salvage option. [9] (10.1007/s11552-014-9698-7)
- [L5] Clinically, a DTM at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion. [10] (10.1016/j.jhsa.2007.08.014)
- [L4] This technique is an effective method to perform radioscapholunate arthrodesis in appropriately selected patients with a preserved midcarpal joint, achieving a 100% union rate at mean follow-up of 12 months with no complications. [11] (10.1016/j.jhsa.2013.01.026)
- [L4] Lunate excision without midcarpal fusion resulted in a disease-free state with good painless range of motion at 6 years, avoiding the recurrence associated with curettage and the motion loss associated with fusion. [12] (10.1177/1753193413488303)
- [L4] Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions. [13] (10.1177/1753193410395357)
- [L4] The results after total wrist joint arthroplasty vary probably as the result of different patient groups, implant types and evolution of prosthetic designs, and are not comparable with the present study. [14] (10.1186/s12891-018-2172-x)
- [Case_report] Due to this disappointing result of the operation with premature mechanical instability, the authors cannot support the use of magnesium-based screws for partial wrist arthrodesis, at least not in dual use. [15] (10.1155/2016/7049130)
- [L2] Both surgical groups demonstrated decreased wrist kinematic motion and functional performance compared with individuals with normal wrists. [16] (10.1016/j.jhsa.2015.04.035)
- [L4] Scaphoid nonunions have a dramatic impact on carpal kinematics, partially uncoupling the proximal and distal carpal rows. [17] (10.1016/j.jhsa.2008.03.008)
- [L5] Further studies need to be performed to address differences in anatomy and wrist movement among patients with different lunate shapes. [18] (10.1016/j.jht.2015.01.007)
- [L4] Although radiographic carpal collapse and ulnar translocation occurred, patients were not symptomatic. [19] (10.1016/j.jhsa.2014.12.013)
- [L2] From an 8- to 11-year perspective, patients with distal scaphoid fractures report normal self-assessed hand function as well as good wrist motion and strength. [20] (10.1016/j.jhsa.2017.06.016)
- [L4] Parallel K-wire placement across the midcarpal joints with scaphoid leads to a high rate of fusion with good patient outcomes long term. [21] (10.1177/15589447211057302)
- [L5] Our findings suggest that load is preferentially transferred to the radiolunate joint after scaphoid excision with four-corner fusion. [22] (10.1007/s11552-007-9048-0)
- [L5] Radial wrist hemiarthroplasty implants are not approved by the FDA for use in humans in the United States and must be performed as off-label use with full patient understanding and appropriate institutional review board approval. [23] (10.1016/j.jhsa.2012.10.050)
- [L4] This approach does not preclude the possibility of secondary arthrodesis in case of failure. [24] (10.1016/j.jhsa.2025.06.004)
- [L4] Better results were seen when the arthrodesis fused. [25] (10.1177/1753193414524876)
- [Case_report] This case illustrates the importance of careful review of radiographs for evidence of intercarpal injuries, as delayed diagnosis resulted in persistent median nerve dysfunction. [27] (10.1007/s11552-013-9545-2)
- [L5] Despite complex carpal bone anatomy and kinematics, computed fiber elongations were found to vary linearly with wrist position. [29] (10.1016/j.jhsa.2012.04.025)
- [L5] However, during simple unresisted wrist motions, the force did not exceed 20 N. [30] (10.1016/j.jhsa.2015.04.007)
- [L3] These kinematic changes may predict the development of radioscaphoid arthritis and help identify a kinematically abnormal wrist. [31] (10.1177/17531934241242676)
- [L4] Comprehending carpal dysfunctions and instabilities hinges on understanding carpal anatomy and normal biomechanics. [32] (10.1016/j.jht.2023.09.011)
- [L5] Advances in 3-dimensional and 4-dimensional imaging have provided clearer insight into carpal kinematics, establishing that the distal carpal row has negligible intercarpal motion while the proximal row drives motion. [33] (10.1016/j.jhsa.2016.07.105)
- [L4] More than half the motion of the carpus when the wrist was loaded in extension occurred at the midcarpal joint. [34] (10.1016/j.jhsa.2012.10.035)
- [L4] Static imaging techniques may accurately depict major wrist ligamentous injury, while dynamic ultrasound and videofluoroscopy may demonstrate dynamic instability and kinematic dysfunction. [35] (10.1177/1753193415610515)
- [L5] Despite individual variance, a pattern of kinematic changes was established after scapholunate ligament injury. [38] (10.1177/1753193415600669)
- [L5] Accurate identification of carpal bone morphology is required to improve our understanding of carpal mechanics and pathology. [39] (10.1016/j.jhsa.2009.03.002)
- [L5] This report updates information on wrist dart-throwing motion based on recent research regarding its kinematics, kinetics, and clinical applications, noting that a wide range of DT planes exists and that midcarpal arthrodesis adversely affects DT motion compared with radiocarpal arthrodesis. [40] (10.1016/j.jhsa.2014.02.035)
- [L5] During forearm rotation, the contact site of the scaphoid and the lunate on the distal radial articular surface changed minimally. [41] (10.1016/j.jhsa.2013.01.021)
- [L4] The technique aims to approximate the original anatomy and restore normal carpal mechanics to prevent progression to scapholunate advanced collapse arthritis. [42] (10.1016/j.jhsa.2013.05.026)
- [L5] Ulnar-sided wrist pain is a common cause of upper extremity disability with a complex differential diagnosis. [43] (10.1016/j.jhsa.2012.04.036)
- [L5] This research underscores the importance of considering forearm rotation when developing rehabilitation protocols for scapholunate joint instability and provides a valuable perspective in line with current rehabilitation principles. [44] (10.1016/j.jht.2023.09.012)
- [L5] Radiocapitate range of motion after PRC was sufficient for activities of daily living. [45] (10.1016/j.jhsa.2006.10.014)
- [Case_report] The patient regained satisfactory function and returned to work at six months with stable carpus on radiographs. [46] (10.1016/j.jhsa.2007.07.025)
- [L4] These results highlight the importance of multicomponent exercise in the treatment of wrist instability. [47] (10.1016/j.jht.2023.08.010)
- [L4] This technique of wrist arthrodesis combining proximal row carpectomy and rigid internal fixation has proved to be a highly predictable operation with much less morbidity and fewer complications than with older techniques using distant bone graft. [48] (10.1016/j.jhsa.2012.11.010)
- [Case_report] Both trigger wrist and avascular necrosis of the capitate are rare disorders. [49] (10.1186/s12891-018-2010-1)
- [L4] The procedure can provoke severe malalignment and midcarpal instability, leading to an intercarpal arthrodesis with an outcome potentially worse than STT fusion. [50] (10.1177/1753193408098903)
- [L5] The procedure aims to alleviate pain and improve range of motion in patients with isolated radiolunate or radioscapholunate arthritis who have failed non-surgical treatment. [51] (10.1016/j.jhsa.2022.04.002)
- [L4] Pyrocarbon interposition arthroplasty is an alternative to total wrist arthrodesis when marked degenerative changes exist at the radiolunate joint, capitate head or both, and increases operative options for challenging clinical scenarios. [52] (10.1177/1753193417714400)
- [L5] Although both simulated fusion types decreased ROM compared with the intact wrist, the principal direction of wrist motion along the path of DTM was not significantly altered by simulated RCF or PCF. [53] (10.1016/j.jhsa.2017.10.017)
- [L4] The case highlights the importance of locking screws in improving the longevity of total wrist arthroplasty by imitating external or internal fixation for bridging large bony defects, allowing the carpal component to remain stable despite complete asymptomatic avascular bone necrosis around the capitate peg. [55] (10.1016/j.jhsg.2024.01.002)
- [L4] The LFT and MFT demonstrate similar congruity to the proximal capitate in the sagittal and coronal planes of the wrist. [56] (10.1016/j.jhsa.2022.04.015)
- [L4] This novel dynamic CT scan of the wrist is a user-friendly way of measuring the scapholunate distance, which is minimal in the normal wrist below 40 years of age. [57] (10.1177/1558944717726372)
- [L4] Delayed diagnosis and late reconstructive surgery were associated with no improvement in radiolunate angle. [58] (10.1016/j.jhsa.2021.04.024)
- [L5] The fusion model confirmed the dart-thrower's hypothesis as wrist motion was primarily preserved from radial-extension toward ulnar-flexion. [59] (10.1016/j.jhsa.2007.12.013)
- [L5] Results suggest that midcarpal stabilisation and scaphoid and triquetrum excision retains most wrist motion. [60] (10.1177/1753193408094923)
- [L4] This procedure preserves motion, yields acceptable functional outcome, and reduces pain. [61] (10.1016/j.arthro.2018.10.134)
- [L2] A scaphoid fracture was by far the most common injury, but it is not clear whether diagnosis of subtle injuries only demonstrated on MRI improves outcomes. [62] (10.1016/j.jhsa.2012.09.034)
- [L5] Measurements in the middle of the scapholunate joint in neutral and 30° of ulnar deviation under fluoroscopic imaging best capture all stages of ligamentous disruptions. [63] (10.1177/1558944717729219)
- [L4] Plain radiographs, CT, 3D-CT, and MRI are suboptimal modalities to assess capitate type. [64] (10.1007/s11552-015-9743-1)
- [L4] Four-corner bone wrist arthrodesis by dorsal rectangular plating achieves an acceptable preservation of range of motion with good pain relief, an excellent consolidation rate and minimal complications. [66] (10.1177/1753193409105684)
- [L4] It provided adequate pain relief and improved the range of wrist motion and grip strength during short-term follow-up. [67] (10.1016/j.jhsa.2015.09.010)
- [L5] While some procedures yield good, predictable outcomes, others are infrequently used due to unpredictable results and high complication rates. [68] (10.1016/j.jhsa.2013.09.014)
- [L3] Wrist fusion rates and average costs are higher in the 4CF group without a significant difference in readmission rates. [70] (10.1016/j.jhsa.2019.12.010)
- [L3] Conversion rates to total wrist arthrodesis are significantly higher with PWA (19.2%) than with PRC (4.9%) and have a greater associated direct cost. [71] (10.1016/j.jhsa.2017.07.032)
- [L4] Based on the high complication rate following FCA with a nonlocking plate, the authors no longer use this implant and recommend fixation with a locking screw plate. [74] (10.1016/j.jhsa.2017.10.036)
References¶
[1] How Much Scaphoid Can be Safely Resected? A Biomechanical Analysis of the Effects of Distal Scaphoid Resection. HAND. 2020. DOI: 10.1177/1558944720966717 [2] Vascularized Bone Graft to the Lunate Combined with Shortening of the Capitate and Radius for Treatment of Advanced Kienböck Disease After a Follow-Up for More Than 10 Years. Journal of Hand Surgery Global Online. 2020. DOI: 10.1016/j.jhsg.2019.09.012 [3] The use of a pyrocarbon capitate resurfacing implant in chronic wrist disorders. Journal of Hand Surgery (European Volume). 2013. DOI: 10.1177/1753193413501730 [4] Midcarpal instability. Journal of Hand Surgery (European Volume). 2015. DOI: 10.1177/1753193415617756 [5] Resilience of SLAC 4-Corner Fusion: Long-Term Follow-Up. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2014.06.118 [6] The Outcome of Scaphoid Excision and Four-Corner Arthrodesis for Advanced Carpal Collapse at a Minimum of Ten Years. The Journal of Hand Surgery. 2010. DOI: 10.1016/j.jhsa.2010.01.025 [7] Reduction and Association of the Scaphoid and Lunate Procedure: Short-Term Clinical and Radiographic Outcomes. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2014.07.014 [8] Ten-Year Minimum Follow-Up of 4-Corner Fusion for SLAC and SNAC Wrist. HAND. 2016. DOI: 10.1177/1558944716681949 [9] Pyrocarbon Interposition Arthroplasty for Proximal Capitate Avascular Necrosis. HAND. 2014. DOI: 10.1007/s11552-014-9698-7 [10] 2007 IFSSH Committee Report of Wrist Biomechanics Committee: Biomechanics of the So-Called Dart-Throwing Motion of the Wrist. The Journal of Hand Surgery. 2007. DOI: 10.1016/j.jhsa.2007.08.014 [11] Radioscapholunate Arthrodesis With Compression Screws and Local Autograft. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.01.026 [12] Three-dimensional analysis of the proximal articulating surfaces of the lunate and capitate. Journal of Hand Surgery (European Volume). 2013. DOI: 10.1177/1753193413488303 [13] A new plate for partial wrist fusions: results in midcarpal arthrodesis. Journal of Hand Surgery (European Volume). 2011. DOI: 10.1177/1753193410395357 [14] Radiocarpal fusion and midcarpal resection interposition arthroplasty: long-term results in severely destroyed rheumatoid wrists. BMC Musculoskeletal Disorders. 2018. DOI: 10.1186/s12891-018-2172-x [15] A Case of Implant Failure in Partial Wrist Fusion Applying Magnesium-Based Headless Bone Screws. Case Reports in Orthopedics. 2016. DOI: 10.1155/2016/7049130 [16] Surgical Treatments for Scapholunate Advanced Collapse Wrist: Kinematics and Functional Performance. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2015.04.035 [17] Interfragmentary Motion in Patients With Scaphoid Nonunion. The Journal of Hand Surgery. 2008. DOI: 10.1016/j.jhsa.2008.03.008 [18] Dart-Splint: An innovative orthosis that can be integrated into a scapho-lunate and palmar midcarpal instability re-education protocol. Journal of Hand Therapy. 2015. DOI: 10.1016/j.jht.2015.01.007 [19] Scaphocapitate Arthrodesis for Kienböck Disease. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2014.12.013 [20] Long-Term Outcomes After Distal Scaphoid Fractures: A 10-Year Follow-Up. The Journal of Hand Surgery. 2017. DOI: 10.1016/j.jhsa.2017.06.016 [21] Parallel K-Wire Placement Leads to Fusion and Midcarpal Settling in Scaphoid Excision Four-Corner Fusion. HAND. 2021. DOI: 10.1177/15589447211057302 [22] Scaphoid Excision with Four-Corner Fusion: A Biomechanical Study. HAND. 2007. DOI: 10.1007/s11552-007-9048-0 [23] “Off-Label” Use of Orthopedic Implants in the Wrist. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.10.050 [24] Arthroscopic Resection of the Proximal Capitate With Tendon Interposition for Isolated Capitolunate Osteoarthritis: A Retrospective Series of Six Cases. The Journal of Hand Surgery. 2026. DOI: 10.1016/j.jhsa.2025.06.004 [25] Avascular necrosis of the capitate: report of six cases and review of the literature. Journal of Hand Surgery (European Volume). 2014. DOI: 10.1177/1753193414524876 [27] Volar Capitate Dislocation: A Case Report. HAND. 2013. DOI: 10.1007/s11552-013-9545-2 [29] Elongation of the Dorsal Carpal Ligaments: A Computational Study of In Vivo Carpal Kinematics. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.04.025 [30] Force in the Scapholunate Interosseous Ligament During Active Wrist Motion. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2015.04.007 [31] Radiocarpal and midcarpal kinematics in scapholunate instability: a four-dimensional CT study in vivo. Journal of Hand Surgery (European Volume). 2024. DOI: 10.1177/17531934241242676 [32] Scapholunate and lunotriquetral joint dynamic stabilizers and their role in wrist neuromuscular control and proprioception. Journal of Hand Therapy. 2024. DOI: 10.1016/j.jht.2023.09.011 [33] Carpal Kinematics and Kinetics. The Journal of Hand Surgery. 2016. DOI: 10.1016/j.jhsa.2016.07.105 [34] In Vivo Kinematics of the Scaphoid, Lunate, Capitate, and Third Metacarpal in Extreme Wrist Flexion and Extension. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.10.035 [35] Imaging in carpal instability. Journal of Hand Surgery (European Volume). 2015. DOI: 10.1177/1753193415610515 [38] Impact of scapholunate dissociation on human wrist kinematics. Journal of Hand Surgery (European Volume). 2015. DOI: 10.1177/1753193415600669 [39] Imaging Recognition of Morphological Variants at the Midcarpal Joint. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2009.03.002 [40] International Federation of Societies for Surgery of the Hand 2013 Committee's Report on Wrist Dart-Throwing Motion. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2014.02.035 [41] Changes in Contact Site of the Radiocarpal Joint and Lengths of the Carpal Ligaments in Forearm Rotation: An In Vivo Study. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.01.021 [42] Reconstruction of Both Volar and Dorsal Limbs of the Scapholunate Interosseous Ligament. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.05.026 [43] Ulnar-sided Wrist Pain: Evaluation and Treatment of Triangular Fibrocartilage Complex Tears, Ulnocarpal Impaction Syndrome, and Lunotriquetral Ligament Tears. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.04.036 [44] Influence of forearm rotation on the kinetic stabilizing efficiency of the muscles that control the scapholunate joint. Clinical application in proprioceptive and neuromuscular rehabilitation programs. Journal of Hand Therapy. 2024. DOI: 10.1016/j.jht.2023.09.012 [45] Carpal Kinematics After Proximal Row Carpectomy. The Journal of Hand Surgery. 2007. DOI: 10.1016/j.jhsa.2006.10.014 [46] Complex Carpal Dissociation With Open, Complete, and Divergent Trapezium, Capitate, and Hamate Dislocation: A Case Report. The Journal of Hand Surgery. 2007. DOI: 10.1016/j.jhsa.2007.07.025 [47] Exercise-based intervention as a nonsurgical treatment for patients with carpal instability: A case series. Journal of Hand Therapy. 2024. DOI: 10.1016/j.jht.2023.08.010 [48] Modified AO Arthrodesis of the Wrist (With Proximal Row Carpectomy). The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.11.010 [49] Trigger wrist caused by avascular necrosis of the capitate: a case report. BMC Musculoskeletal Disorders. 2018. DOI: 10.1186/s12891-018-2010-1 [50] Midcarpal instability after excision arthroplasty for scapho-trapezial-trapezoid (STT) arthritis. Journal of Hand Surgery (European Volume). 2009. DOI: 10.1177/1753193408098903 [51] Radiocarpal Fusion: Indications, Technique, and Modifications. The Journal of Hand Surgery. 2022. DOI: 10.1016/j.jhsa.2022.04.002 [52] Vascular anatomy of the capitate determined by micro-computed tomography angiography. Journal of Hand Surgery (European Volume). 2017. DOI: 10.1177/1753193417714400 [53] Relative Contributions of the Midcarpal and Radiocarpal Joints to Dart-Thrower’s Motion at the Wrist. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2017.10.017 [55] The Crucial Role of Locking Screws in Total Wrist Arthroplasty: Should We Always Revise or Not?. Journal of Hand Surgery Global Online. 2024. DOI: 10.1016/j.jhsg.2024.01.002 [56] Lateral Femoral Trochlea Flap Reconstruction of the Proximal Capitate: An Assessment of Congruity and Description of Technique. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.04.015 [57] Dynamic CT Scan of the Normal Scapholunate Joint in a Clenched Fist and Radial and Ulnar Deviation. HAND. 2017. DOI: 10.1177/1558944717726372 [58] Traumatic Nondissociative Carpal Instability: A Case Series. The Journal of Hand Surgery. 2022. DOI: 10.1016/j.jhsa.2021.04.024 [59] Simulated Radioscapholunate Fusion Alters Carpal Kinematics While Preserving Dart-Thrower's Motion. The Journal of Hand Surgery. 2008. DOI: 10.1016/j.jhsa.2007.12.013 [60] Effect of scaphoid and triquetrum excision after limited stabilisation on cadaver wrist movement. Journal of Hand Surgery (European Volume). 2009. DOI: 10.1177/1753193408094923 [61] Arthroscopic Interposition Tendon Arthroplasty for Stage 2 Scapholunate Advanced Collapse. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2018.10.134 [62] The Benefit of Magnetic Resonance Imaging for Patients With Posttraumatic Radial Wrist Tenderness. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.09.034 [63] The Optimal Location to Measure Scapholunate Diastasis on Screening Radiographs. HAND. 2017. DOI: 10.1177/1558944717729219 [64] Common Radiographic Imaging Modalities Fail to Accurately Predict Capitate Morphology. HAND. 2015. DOI: 10.1007/s11552-015-9743-1 [66] Four-corner bone arthrodesis with dorsal rectangular plate: series and personal technique. Journal of Hand Surgery (European Volume). 2009. DOI: 10.1177/1753193409105684 [67] Arthroscopic Partial Capitate Resection for Type Ia Avascular Necrosis: A Short-Term Outcome Analysis. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2015.09.010 [68] Intercarpal Arthrodeses. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2013.09.014 [70] Proximal Row Carpectomy Versus 4-Corner Fusion: Incidence, Conversion to Fusion, and Cost. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2019.12.010 [71] A Comparative Analysis of Resource Utilization Between Proximal Row Carpectomy and Partial Wrist Fusion: A Population Study. The Journal of Hand Surgery. 2017. DOI: 10.1016/j.jhsa.2017.07.032 [74] Treatment Outcomes of 4-Corner Arthrodesis for Patients With Advanced Carpal Collapse: An Average of 4 Years’ Follow-Up Comparing 2 Different Plate Types. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2017.10.036