Patients › Rehabilitation
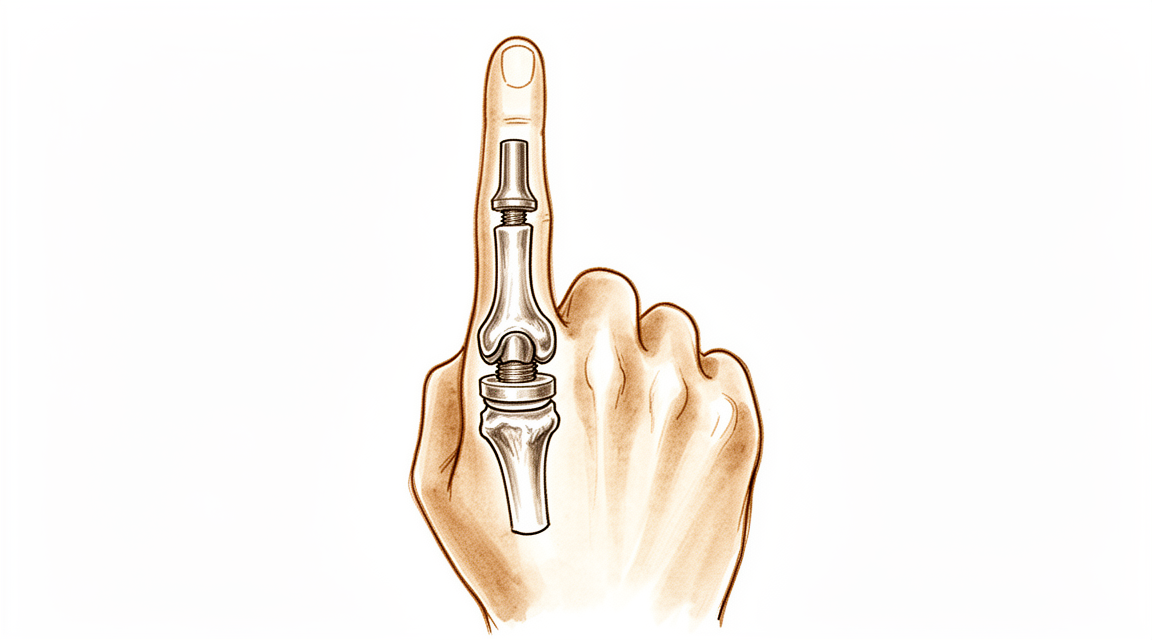
Substituição da Articulação da PIP
Um plano de recuperação protegido após a substituição por silicone da articulação média desgastada de um dedo (articulação interfalangeana proximal, PIP), em que a velocidade para iniciar os movimentos depende de o cirurgião ter realizado a abordagem pela frente (lado da palma) ou pela parte posterior do dedo.
Este protocolo orienta a sua recuperação após a substituição da articulação média desgastada de um dedo (a articulação interfalângica proximal (PIP), a articulação média do dedo) com um espaçador flexível de silicone, realizada pelo Dr. Kieran Hirpara no Mater Private Hospital Rockhampton. Inicia-se com o seu programa de exercícios em casa, seguido pelo protocolo clínico estruturado, redigido para o seu fisioterapeuta da mão. Traga esta página ou o seu PDF para a sua primeira consulta de terapia, para que a sua reabilitação seja coordenada. O seu terapeuta pode ajustar o plano, dependendo da evolução da sua recuperação.
Se tiver alguma preocupação sobre a sua ferida após a cirurgia, entre em contacto com a clínica. É frequentemente útil tirar uma fotografia da ferida e enviá-la por e-mail para avaliação.
O que esperar¶
A articulação média do seu dedo desgastou-se devido à artrite, o que causa dor e rigidez. Nesta operação, as superfícies articulares desgastadas são removidas e um espaçador de silicone flexível (um implante do tipo Swanson) é colocado entre os dois ossos. O espaçador não é uma articulação mecânica rígida; é um espaçador flexível que mantém os ossos afastados, permite a flexão do dedo e possibilita que o seu próprio tecido cicatricial forme uma nova bainha de suporte à sua volta. O benefício principal e mais fiável é o alívio da dor. Deve também esperar um arco útil e modesto de flexão (geralmente entre 40 e 60 graus) em vez de uma amplitude de movimento completa e normal. A maioria das pessoas fica muito satisfeita porque a dor desaparece e o dedo torna-se confortável para utilizar.
O aspeto mais importante da sua recuperação é a via de acesso cirúrgica utilizada, pois isso determina a rapidez com que pode começar a mover o dedo:
- Pela frente (lado da palma, abordagem volar): o tendão extensor na parte dorsal do dedo é deixado completamente íntegro. Como nada na parte de trás precisa de cicatrizar, pode geralmente começar a mover o dedo dentro de alguns dias.
- Pelo dorso (abordagem dorsal): o tendão extensor (o deslizamento central) tem de ser dividido ou levantado para aceder à articulação, sendo depois reparado. Essa reparação deve ser protegida inicialmente, pelo que o dedo é imobilizado em extensão precocemente e a flexão é introduzida de forma mais gradual, sob orientação do seu terapeuta da mão.
O seu terapeuta da mão seguirá o plano correspondente à sua via de acesso cirúrgico. O Dr. Hirpara informará o terapeuta sobre qual abordagem foi utilizada, e os prazos abaixo estão adaptados a essa abordagem. Independentemente da abordagem utilizada, a nova articulação funciona como uma dobradiça: beneficia da flexão e extensão numa linha reta, mas não tolera empurrões ou torções laterais. Protegê-la de tensões laterais é o que mantém a sua estabilidade a longo prazo.
Precauções e limitações¶
- Mova o dedo apenas em linha reta (flexão e extensão) e evite qualquer força lateral ou de torção no dedo operado. A nova articulação é uma dobradiça, e a tensão lateral pode afrouxá-la ou deformá-la.
- Use a tala conforme prescrito e utilize imobilização com o dedo adjacente durante as atividades para manter o alinhamento reto do dedo.
- Se a sua cirurgia foi na parte dorsal do dedo, NÃO force a extensão além do limite estabelecido inicialmente: o tendão extensor está em processo de cicatrização.
- NÃO realize preensão firme, pinçamento intenso ou tarefas pesadas ou de torção até que o terapeuta da mão autorize o fortalecimento (comumente a partir de seis semanas).
- Mantenha as outras articulações dos dedos, o punho e o ombro em movimento desde o início, e utilize a mão para tarefas leves do dia a dia, dentro dos limites do conforto.
Para o manejo da ferida, edema e cicatriz, consulte as orientações da clínica sobre cuidados com a ferida.
Os seus exercícios¶
Estes são os exercícios do seu folheto informativo. Inicie-os apenas conforme orientado pelo Dr. Hirpara e pelo seu terapeuta da mão, mantendo-se dentro da amplitude e dos limites que lhe foram indicados. O trabalho inicial mantém o dedo em movimento numa linha reta, sem tensão lateral: flexão protegida, extensão suave, imobilização em buddy (tala de buddy) e deslizes tendinosos. Se a sua cirurgia foi realizada na parte dorsal do dedo, o exercício de extensão ativa é aquele que deve ser protegido nas fases iniciais e progressivamente incrementado. O fortalecimento da preensão pertence a uma fase posterior e não deve ser iniciado até que receba autorização específica para tal. Interrompa qualquer atividade que cause dor aguda ou que faça o dedo parecer instável.
Seu protocolo clínico¶
O restante desta página é o protocolo clínico em fases para reabilitação após artroplastia da articulação interfalangiana proximal (PIP) com implante de silicone. Esta seção deve ser fornecida ao seu terapeuta da mão, e cada fase inicia-se com uma explicação em linguagem simples do que está ocorrendo. O protocolo depende da abordagem cirúrgica, sendo este o ponto central de decisão: uma abordagem volar (palmar) preserva o mecanismo extensor e permite movimento ativo precoce em poucos dias; uma abordagem dorsal divide ou fraciona o deslizamento central, portanto, a cicatrização do extensor deve ser protegida inicialmente com órteses de extensão e flexão graduada. Ao longo de todo o processo, o implante de silicone atua como um espaçador flexível, cuja estabilidade a longo prazo depende da cápsula peri-implantar, portanto, o estresse coronal (lateral) é evitado e o movimento é mantido em um arco puramente sagital.
Antes do início do tratamento, confirme com o cirurgião assistente a abordagem cirúrgica (volar versus dorsal), a integridade/reparo do deslizamento central e dos ligamentos colaterais, bem como qualquer arco de movimento intraoperatório. O Dr. Hirpara especificará a abordagem; selecione a via volar (movimento ativo precoce) ou dorsal (proteção da extensão) conforme o caso. O alvo funcional esperado é um arco de movimento livre de dor de aproximadamente 40–60°, e não amplitude total.
Fase I — proteger e iniciar o movimento (semanas 0 a 3)¶
As primeiras semanas protegem os tecidos moles enquanto previnem a rigidez, com o ritmo definido exclusivamente pela abordagem cirúrgica. O implante é estável em flexão-extensão, mas vulnerável a cargas laterais, portanto, todo o movimento é mantido num plano sagital puro e o dedo é suportado por imobilização buddy (taping ao dedo adjacente) e uma talas.
Para o seu terapeuta da mão:
Educação e precauções - Identificar a abordagem cirúrgica e seguir o protocolo correspondente: - Abordagem volar: mecanismo extensor íntegro → iniciar movimento ativo do PIP/DIP aos 3–5 dias. Ajustar uma talas de bloco de extensão volar / modelo que permita um arco curto de flexão (comumente ~30° inicialmente), aumentado progressivamente. - Abordagem dorsal (fenda/reparo do deslizamento central): proteger a extensão. PIP imobilizado em extensão quase total durante todo o tempo; introduzir flexão ativa num arco curto limitado sob supervisão, respeitando o reparo do deslizamento central. (Um esquema de movimento relativo / extensão dinâmica pode ser utilizado conforme a preferência do cirurgião.) - Evitar estritamente o stress coronal (lateral/rádio-ulnar) na articulação operada: imobilização buddy ao dígito adjacente para orientar um rastreamento puramente sagital. - Sem preensão, pinçamento ou uso resistido/carregado.
Gestão - Ferida: curativos cirúrgicos conforme indicado; monitorizar infeção - Edema: elevação, massagem retrograde suave, bandagem compressiva leve - Exercícios: flexão-extensão ativa do PIP/DIP protegida dentro do arco definido; deslizamentos tendinosos; movimento ativo das articulações não envolvidas (DIP, MCP, punho, polegar); iniciar imobilização buddy para atividades - Talas usadas durante todo o tempo entre as sessões de exercício
Critérios para progressão - Cicatrização satisfatória da ferida; sem desenvolvimento de lag extensor (via dorsal); movimento confortável e controlado dentro do arco atual
Fase II — avanço do movimento (semanas 3 a 6)¶
O arco de flexão é ampliado e, para os dedos com abordagem dorsal, a proteção contra a extensão é progressivamente relaxada à medida que o deslizamento central se consolida. O objetivo desta janela é consolidar o arco útil (≈40–60°) antes que a maturação da cicatriz fixe a amplitude de movimento.
Para o seu terapeuta da mão:
Avaliações - Arco de PIP ativo e passivo; lag extensor (via dorsal); estabilidade coronal; dor e edema; revisão da ferida/cicatriz
Educação e precauções - Aumentar progressivamente o arco de flexão permitido em direção ao alvo funcional (≈40–60°) - Volar: avançar a flexão ativa conforme tolerado; adicionar flexão passiva suave se a extensão estiver completa e estável - Dorsal: reduzir gradualmente o uso da tala de extensão de acordo com a cicatrização do deslizamento central (comumente, reduzir o suporte diurno entre as semanas 4 e 6); prevenir o lag extensor: não buscar flexão à custa da extensão ativa - Continuar a evitação rigorosa de carga lateral/torcional; ainda sem fortalecimento resistido
Conduta - Exercícios: flexão-extensão de PIP ativa e ativa-assistida graduada; exercícios de bloqueio para focar o movimento de PIP; continuar os deslizes tendinosos e a imobilização em grupo; iniciar massagem cicatricial apenas após a cicatrização da ferida - Manter a amplitude de movimento completa das articulações adjacentes
Critérios para progressão - Ferida cicatrizada; articulação estável no plano coronal; arco funcional e sem dor estabelecido; lag extensor mínimo (dorsal)
Fase III — fortalecimento e retorno (semanas 6 a 12 e além)¶
Uma vez estabelecido o movimento e os tecidos moles estiverem íntegros (por volta das seis semanas), inicia-se o fortalecimento leve, que é progressivamente intensificado. O fortalecimento é mantido na direção axial (pegada e carga em linha reta), respeitando-se a longo prazo a tensão lateral/torcional sobre o implante.
Para o seu terapeuta da mão:
Avaliações - Pegada e pinça em comparação com o lado contralateral; arco final da articulação interfalangiana proximal (PIP); estabilidade coronal; testes funcionais e específicos de tarefas
Educação e precauções - Iniciar fortalecimento leve da pegada por volta das seis semanas, com progressão gradual - Introduzir a carga por pinça com cautela e continuar a evitar cargas laterais/torciais vigorosas na articulação operada indefinidamente (para preservar a longevidade do implante) - Estabelecer expectativas realistas: o ganho primário é o alívio da dor duradouro; o arco final é modesto (≈40–60°) e está praticamente definido por volta dos 3 meses
Conduta - Exercícios: trabalho progressivo de pegada/com massa de modelar; carga funcional e específica para o trabalho de forma graduada; continuar qualquer trabalho residual de mobilidade e cicatriz - Considerar a alta quando um dedo estável, confortável e funcional, com um arco útil sem dor, for alcançado - Encaminhar de volta ao médico assistente se a recuperação estagnar, a articulação se tornar instável/desviar, ou se houver suspeita de falha do implante
Critérios para alta / retorno - Articulação confortável, sem dor e estável na coroa, com um arco funcional; pegada adequada; capacidade de atender às demandas diárias e laborais
Retorno ao trabalho e às atividades¶
O uso leve das mãos nas atividades diárias (comer, escrever, cuidados pessoais leves) é incentivado desde o início, dentro dos limites do conforto, desde que o movimento seja mantido em linha reta e se evite força lateral ou de torção no dedo operado. A direção de veículos geralmente é possível quando você consegue segurar o volante com conforto e controlar o carro com segurança, estiver fora do talhe restritivo e não estiver mais fazendo uso de analgésicos potentes, o que normalmente ocorre após algumas semanas, sendo confirmado na sua consulta de acompanhamento.
As tarefas que exigem preensão mais firme e carga aguardam até aproximadamente seis semanas, sendo então progressivamente intensificadas. O trabalho manual mais pesado ou com movimentos de torção é o último a ser retomado, e depende da recuperação de um dedo confortável e estável, com preensão adequada, avaliada pelo Dr. Hirpara e pelo seu terapeuta da mão, e não apenas pelo calendário. Lembre-se do resultado duradouro desta cirurgia: alívio confiável da dor e um arco útil de aproximadamente 40 a 60 graus, evitando-se, a longo prazo, esforços laterais na articulação para proteger o implante.
Após o seu protocolo¶
Este protocolo complementa as orientações gerais de recuperação da clínica; consulte o manejo da dor pós-operatória, o cuidado com a ferida e o manejo da cicatriz. O plano em fases acima reflete as orientações publicadas de reabilitação após artroplastia da articulação interfalangeana proximal (PIP) com implante de silicone, e a sua recuperação contínua é orientada individualmente pelo Dr. Hirpara e pelo seu terapeuta da mão, de acordo com a abordagem cirúrgica utilizada e com a evolução do seu dedo.
Evidence & references
Silicone PIP Joint Replacement — Procedure Outcomes & Post-operative Rehabilitation (Swanson-type Arthroplasty for PIP Osteoarthritis)¶
Topic scope: post-operative rehabilitation after silicone (Swanson-type) proximal interphalangeal (PIP) joint arthroplasty for primary osteoarthritis. The worn joint surfaces are excised and a flexible silicone spacer is implanted; this is an interposition / encapsulation arthroplasty, not a rigidly-fixed mechanical hinge. The implant works as a flexible spacer around which a peri-implant fibrous capsule forms to provide stability. The dominant, reliable benefit is pain relief; the functional gain is a modest active arc (~40–60°), not restoration of normal range.
Defining principle of the rehab here: the rehabilitation pathway is dictated by the surgical approach, because the rate-limiting tissue is the extensor mechanism, not the implant. A volar (palmar) approach leaves the central slip and extensor mechanism intact → it permits immediate / early active motion (within 3–5 days). A dorsal approach must split or reflect the central slip to reach the joint → the extensor repair must be protected first with extension orthotics and a graded, short-arc flexion programme. Across both pathways the silicone spacer is stable in the sagittal (flexion–extension) plane but vulnerable in the coronal plane, so the programme deliberately avoids lateral / torsional load and tracks the joint in a pure sagittal arc (buddy strapping). Therapy aims to bank the useful arc before scar maturation fixes it while protecting extension and the implant — it is not an immobilise-to-heal construct in the volar case.
A. PROCEDURE OUTCOMES (silicone PIP arthroplasty for osteoarthritis)¶
Silicone PIP arthroplasty is a reliable pain-relieving operation with predictable but modest motion; the principal debates are over surgical approach and implant choice (silicone vs surface-replacement/pyrocarbon), not whether arthroplasty relieves pain.
- Pain relief is high and durable; motion gains are modest. A long-term series of Swanson silicone PIP arthroplasty for osteoarthritis (mean ~10-year follow-up) reported excellent pain relief (mean VAS ~0.4) with essentially unchanged arc (≈55° pre-op → ≈50° post-op) and high patient satisfaction — patients would have the surgery again despite limited motion gain [Bales, Wall & Stern, J Hand Surg Am 2014]. Moderate (level-IV long-term cohort).
- The volar approach can improve the active arc. A volar-approach silicone PIP series reported the active arc improving from ~33° to ~72°, with good function and satisfaction, by preserving the extensor mechanism and enabling early motion [Proubasta et al., J Hand Surg Am 2014]. Moderate–weak (level-IV).
- Radiographic implant deformation/fracture is common but poorly correlated with symptoms. In the long-term Swanson series most implants deformed and many fractured radiographically, yet clinical revision was uncommon (survivorship ~90% at ~10 years) and there was no correlation between radiographs and satisfaction [Bales, Wall & Stern 2014]. Strong natural-history signal within a cohort.
- Silicone vs surface-replacement and pyrocarbon implants give broadly comparable clinical results; no implant is clearly superior. Systematic review across implants/approaches found comparable outcomes with implant-/approach-specific complication profiles [Yamamoto et al., Plast Reconstr Surg 2017; Carlson Strother, Moran & Rizzo, JAAOS 2023]. Moderate (SR + narrative review).
- Pyrocarbon and resurfacing implants carry their own failure modes (subsidence, squeaking, intra-operative periprosthetic fracture, instability), informing implant choice rather than rehab [Watts et al., J Hand Surg Am 2012; Wagner et al. medium-term 2018 & intra-op fractures 2015; Branam et al. resurfacing-vs-silicone 2007]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE¶
The central rehab questions are (1) how soon to move and (2) how to splint, and the answer to both is set by the surgical approach and the extensor mechanism. The evidence base is low-level (expert consensus / single-cohort therapy series) — there are no RCTs comparing PIP arthroplasty rehab pathways.
- Approach dictates the timeline (the core principle). Surgical reviews establish that a volar approach preserves the central slip and permits immediate active and passive motion, while a dorsal approach requires post-operative protection of the split/repaired central slip before flexion is advanced [Renfree, Bone Joint J 2022 (surgical approaches); Herren, Hand Clin 2017; Yamamoto et al. 2017]. Moderate (surgical evidence) — strong mechanistic basis.
- A structured 12-week, splint-based therapy programme is the consensus framework (dorsal pathway). Feldscher's hand-therapy protocol for PIP (pyrocarbon, central-slip-splitting dorsal approach) uses a volar static finger orthosis allowing a limited short-arc PIP/DIP active arc that is increased over the rehab course, with a hand-based resting splint (MCP flexed, PIP/DIP near 0°) for full-time use except during template-splint exercise [Feldscher, J Hand Ther 2010]. Weak (expert-consensus protocol).
- A defined controlled-motion program exists and reports good arcs. A controlled-motion rehabilitation program for PIP arthroplasty reported favourable range-of-motion outcomes, supporting graded controlled motion over rigid immobilisation [Ramanathan, Koludrovich & Evans, J Hand Ther 2021]. Weak (cohort / programme description).
- Static and dynamic extension splinting give similar results. A comparison of static vs dynamic splinting after PIP pyrocarbon arthroplasty found comparable outcomes, favouring static splinting for simplicity and patient convenience [Jennings & Livingstone / static-vs-dynamic cohort, J Hand Ther 2011]. Weak–moderate (comparative cohort).
- Coronal-plane protection is the durable, lifelong caveat. Collateral integrity and avoidance of lateral stress underpin long-term implant stability; collateral compromise drives instability/deviation [Carlo et al., collateral reconstruction, J Hand Surg Am 2016; Carlson Strother et al. 2023]. Consensus / mechanistic.
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint (by approach) | Hand-therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect & initiate motion | Week 0–3 | Volar: active motion at 3–5 days, short flexion arc (~30°) in template/extension-block splint. Dorsal: PIP splinted near extension full-time; supervised short-arc flexion only | Protected sagittal PIP/DIP motion; tendon glides; buddy strapping; uninvolved-joint motion; no lateral/torsional load | None (no grip/pinch) | Implant stable in flexion–extension, vulnerable coronally |
| II — Advance motion | Week 3–6 | Progressively increase flexion arc toward ~40–60°. Dorsal: wean extension splint as central slip consolidates (≈wk 4–6); guard against extensor lag | Graded active/AAROM flexion–extension; blocking; scar massage once healed; continue buddy strapping | Still no resisted strengthening | Bank the useful arc before scar maturation fixes it |
| III — Strengthen & return | Week 6–12+ | Lifting/grip restrictions progressively lifted; lateral/twisting load avoided indefinitely | Light grip → cautious pinch; functional & work-specific loading | Grip from ~6 wk, graded | Pain relief is the durable gain; final arc (~40–60°) largely set by ~3 months |
(Phase windows mirror the precautions in the patient protocol; they are typical guides — not trial-derived deadlines — and the volar vs dorsal split is the dominant variable.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Volar vs dorsal approach (the rehab-defining question). The volar approach spares the extensor mechanism and permits early active motion (and a better reported arc), at the cost of being more technically demanding; the dorsal approach is more familiar but mandates extensor protection and a slower, splint-led flexion programme. Choice is surgeon-dependent and drives the entire rehab pathway. Moderate surgical evidence; no head-to-head rehab RCT.
- Implant choice (silicone vs surface-replacement vs pyrocarbon). No implant is clearly superior on clinical outcomes; silicone is durable for pain relief with high radiographic deformation/fracture that poorly predicts symptoms, while pyrocarbon/resurfacing trade different complication profiles (subsidence, instability, intra-operative fracture). Moderate (SR + cohorts).
- Static vs dynamic splinting (dorsal pathway). Comparable outcomes; static splinting is favoured for simplicity and convenience. Weak–moderate.
- Motion gain is modest and that is expected, not failure. Patients reliably lose pain but gain little arc (especially via dorsal/silicone); mislabelling the modest arc as a poor result misframes a successful pain-relieving operation. Counsel the ~40–60° expectation up front. Strong natural-history signal.
- Lifelong coronal-stress avoidance. Long-term stability depends on the peri-implant capsule and collaterals; forceful lateral/twisting load risks deviation, instability and implant failure. Consensus.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (mechanistic / natural-history): the surgical-approach principle (volar preserves extensor mechanism → early motion; dorsal splits central slip → protect extension first); the modest-arc / reliable-pain-relief outcome pattern; radiographic implant deformation poorly predicting symptoms.
- MODERATE: procedure outcomes are level-IV case series (long-term Swanson silicone series; volar approach series); implant-comparison systematic review/narrative review; surgical-approach reviews.
- WEAK / EXPERT CONSENSUS: the specific rehabilitation regimen — short-arc controlled motion, 12-week splint-based programme, static-vs-dynamic splinting equivalence, exact phase timings. These are low-level, expert-consensus / single-cohort therapy descriptions, not trial-derived; individualise to the operative approach and tissue quality.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2013.11.008
- Proubasta IR, Lamas CG, Natera L, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014;39(6). DOI: 10.1016/j.jhsa.2014.03.033
- Weistra K, Kan HJ, van Alebeek VAHJ, et al. Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex in 72 cases. HAND. 2022. DOI: 10.1177/15589447221122829
- Branam BR, Tuttle HG, Stern PJ, et al. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007. DOI: 10.1016/j.jhsa.2007.04.006
- Yamamoto M, Malay S, Fujihara Y, et al. A systematic review of different implants and approaches for proximal interphalangeal joint arthroplasty. Plast Reconstr Surg. 2017. DOI: 10.1097/prs.0000000000003260
- Renfree KJ. Surgical approaches for proximal interphalangeal joint arthroplasty. Bone Joint J. 2022;104-B(12). DOI: 10.1302/0301-620x.104b12.bjj-2022-0946
- Herren DB. Current European practice in the treatment of proximal interphalangeal joint arthritis. Hand Clin. 2017. DOI: 10.1016/j.hcl.2017.04.002
- Carlson Strother CR, Moran SL, Rizzo M. Small joint arthroplasty of the hand: an update on indications, outcomes, and complications. J Am Acad Orthop Surg. 2023;31(15). DOI: 10.5435/jaaos-d-23-00034
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. DOI: 10.1016/j.jht.2009.10.011
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. DOI: 10.1016/j.jht.2019.04.003
- Watts AC, Hearnden AJ, Trail IA, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: minimum two-year follow-up. J Hand Surg Am. 2012. DOI: 10.1016/j.jhsa.2012.02.012
- Wagner ER, Weston JT, Houdek MT, et al. Medium-term outcomes with pyrocarbon proximal interphalangeal arthroplasty: a study of 170 consecutive arthroplasties. J Hand Surg Am. 2018. DOI: 10.1016/j.jhsa.2018.06.020
- Wagner ER, Van Demark R, Kor DJ, et al. Intraoperative periprosthetic fractures in proximal interphalangeal joint arthroplasty. J Hand Surg Am. 2015. DOI: 10.1016/j.jhsa.2015.06.101
- McGuire DT, White CD, Carter SL, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: outcomes of a cohort study. J Hand Surg Eur Vol. 2011;37(6). DOI: 10.1177/1753193411434053
- Carlo J, Dell PC, Matthias R, et al. Collateral ligament reconstruction of the proximal interphalangeal joint. J Hand Surg Am. 2016;41(1). DOI: 10.1016/j.jhsa.2015.10.007
- Aversano FJ, Calfee RP. Salvaging a failed proximal interphalangeal joint implant. Hand Clin. 2018. DOI: 10.1016/j.hcl.2017.12.011
PIP arthroplasty rehabilitation literature (URLs)¶
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. https://pubmed.ncbi.nlm.nih.gov/20036511/
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/31481342/
- Static versus dynamic splinting for proximal interphalangeal joint pyrocarbon implant arthroplasty: a comparison of current and historical cohorts. J Hand Ther. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143198/
- Proubasta IR, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24799141/
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for PIP joint osteoarthritis. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24559624/
- The dorsal approach to silicone implant arthroplasty of the proximal interphalangeal joint. J Hand Surg Am. 2007. https://www.sciencedirect.com/science/article/abs/pii/S0363502307004662
- Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex. HAND. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC10953532/