Patients › Shoulder
Artritis ng Balikat
Shoulder arthritis causes pain, stiffness, and reduced range of motion — diagnosis and treatment options explored.
Ano ang nararamdaman mo¶
Ang arthritis ng balikat ay isang karaniwang kondisyon. Ito ay nagdudulot ng pinsala dahil sa pagkasira ng mga ibabaw ng kasukasuan. Maaaring mapansin mo na ang pagtaas ng edad ay may kasamang mas maraming sakit at makikita na mga pagbabago sa X-ray. Karaniwang dahan-dahan ang simula ng sakit. Sa ilang kaso, mabilis itong nagiging nakakasira, lalo na sa mga mas matandang babae.
Maaaring mararamdaman mo ang sakit na malalim sa balikat. Karaniwang lumalala ang sakit sa gabi. Maaari ring magpalala ito pagkatapos mong gamitin ang iyong braso o kapag ikaw ay bago pa lamang gumising. Nagiging mahirap ang mga simpleng gawain sa araw-araw. Maaaring mahirapan kang umabot sa likod ng iyong likod upang isara ang bra. Ang pagtutukoy ng isang kamiseta ay maaaring maging awkward o masakit. Ang pagtaas ng mga bagay sa itaas ng ulo ay maaaring mag-trigger ng matulis na kahirapan.
Sisiyasatin ng iyong doktor ang mga partikular na pattern ng pagkasira ng kasukasuan. Halimbawa, ang ulo ng iyong buto ng itaas na braso ay maaaring lumipat pabalik sa socket. Ito ay tinatawag na posterior subluxation. Sa paglipas ng panahon, ang paglipat na ito ay maaaring magbago kung paano nagkasira ang kasukasuan. Humigit-kumulang 20% ng mga balikat na may pattern na ito ay nagdidisenyo ng eccentric wear pattern sa loob ng isang dekada. Hinahanap ng iyong doktor ang mga senyales na ito upang maunawaan ang iyong partikular na sitwasyon.
Maaaring magtanong ka kung ang impeksyon ang nagdudulot ng iyong sakit. Maaaring gumamit ang iyong doktor ng advanced imaging, tulad ng espesyal na PET/CT scan, upang kilalanin ang pagkakaiba sa pagitan ng impeksyon at karaniwang arthritis. Tinitiyak nito na makakakuha ka ng tamang gamutan.
Habang patuloy na nagbabago ang mga estratehiya sa pamamahala, lalo na para sa mga mas batang pasyente, nananatiling isang alalahanin ang tibay ng implant kung ikaw ay napakaaktibo. Usapin ng iyong doktor ang pinakamainam na mga opsyon para sa iyo. Ang anatomic total shoulder replacement ay madalas na ang standard na pagpili kung ang iyong mga rotator cuff tendons ay malusog. Ang reverse total shoulder replacement ay isa pang opsyon, lalo na kung ang cuff ay nasira o sa mga kumplikadong kaso. Layunin ng parehong mga pamamaraan na bawasan ang sakit at mapabuti ang function.
Kung ang iyong mga senyales ng arthritis ay mild sa X-ray, mayroon kang humigit-kumulang pitong beses na mas mataas na odds na hindi mararanasan ang makabuluhang pag-unlad pagkatapos ng anatomic total shoulder replacement kumpara sa mga pasyente na may severe arthritis. Mahalagang konteksto ito para sa iyong pagdedesisyon. Tutulungan ka ng iyong doktor na bigyang-kahulugan ang mga salik na ito laban sa iyong pang-araw-araw na pangangailangan at antas ng aktibidad.
Ano ang nangyayari talaga¶
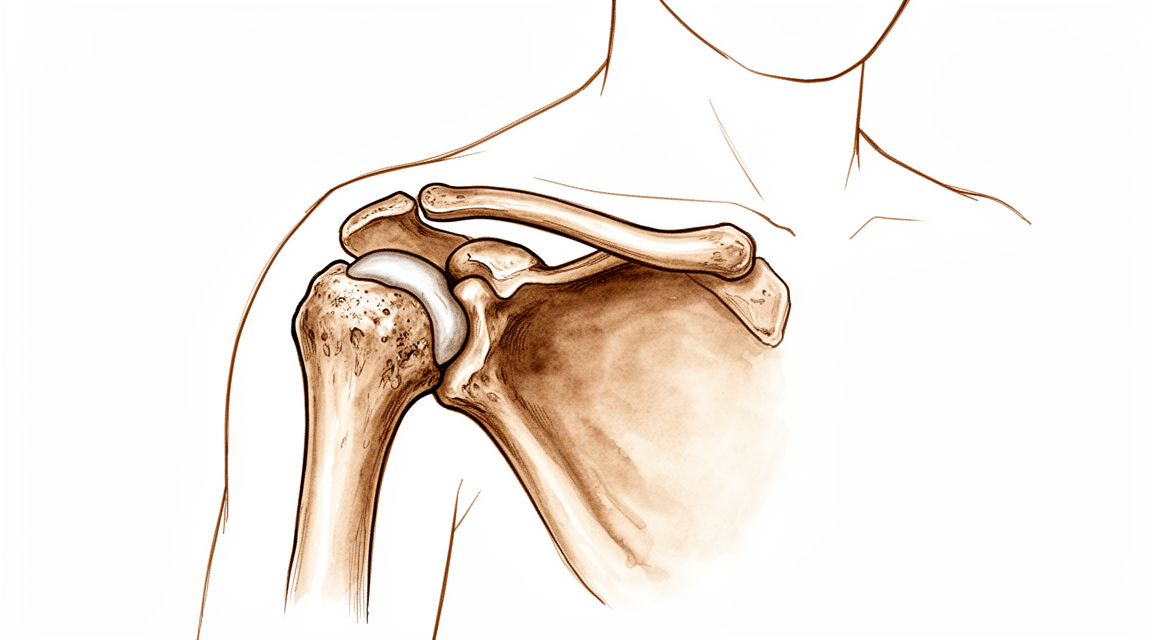
Ang arthritis ng balikat ay isang karaniwang kondisyon ng pagkasira dahil sa paggamit kung saan ang makinis na patong sa dulo ng iyong mga buto ay nababasag. Ang patong na ito, na tinatawag na kartilago, ay gumagana bilang shock absorber. Kapag ito ay naging manipis o nawala, ang mga buto ay magkaka-ikot sa isa’t isa. Ito ang nagdudulot ng sakit at stiffness. Ang iyong joint capsule, ang balat na nakapalibot sa balikat, ay maaari ring maging masikip.
Sa maraming kaso, ang mga tendon ng rotator cuff ay nananatiling buo. Ang mga tendon na ito ay parang mga lubid na tumutulong sa iyo na itaas ang iyong braso. Kapag gumagana nang maayos, ang iyong surgeon ay maaaring gumamit ng anatomic total shoulder replacement. Ang prosedurang ito ay pinalitan ang mga nasirang ibabaw ng buto ng mga artipisyal na bahagi na kumukopya sa likas na hugis ng iyong kasukasuan. Ito ang pamantayang paggamot kapag ang cuff ay malusog.
Minsan, ang rotator cuff ay naputol o mahina. Kung walang mga tendon na ito, ang bola ng kasukasuan ay maaaring lumipat sa maliit na posisyon. Ang iyong surgeon ay maaaring magrekomenda ng reverse total shoulder replacement. Ang operasyong ito ay baligtarin ang bola at socket. Ginagamit nito ang iyong deltoid muscle upang itaas ang iyong braso imbes na ang mga naputol na tendon. Ang disenyo na ito ay tumutulong sa iyo na muling makakuha ng galaw kahit na sira ang cuff.
Ang paraan ng paggalaw ng iyong balikat ay nagbabago pagkatapos ng operasyon. Ang iyong shoulder blade, o scapula, ay gumagana nang mas mahirap upang galawin ang iyong braso. Ito ay normal at inaasahan. Ang bagong disenyo ng kasukasuan ay nagbibigay-daan sa buong saklaw ng galaw, bagama’t magkaiba ang mga pattern ng galaw kumpara sa isang malusog na balikat.
Ang mga disenyo ng implant ay nangungunang umunlad. Ang mga modernong prosthetics ay mas eksaktong angkop at gumagalaw nang mas natural. Gayunpaman, ang tibay ng mga implant na ito ay nananatiling isang alalahanin para sa mga aktibong pasyente. Ang mga mas bata o mas aktibong indibidwal ay maaaring mas mabilis na sira ang mga artipisyal na bahagi. Ang iyong surgeon ay pipili ng pinakamainam na opsyon batay sa iyong partikular na pinsala sa kasukasuan at antas ng aktibidad.
Ano ang maaari naming gawin dito¶
Laging nagsisimula kami sa mga hindi pampasurgical na opsyon, lalo na kung ang iyong arthritis na dulot ng pagkasuot ay katamtaman o mild. Malamang na irekomenda ng iyong surgeon ang isang kursong pamamahala sa sarili at pisyikal na terapiya muna. Ang pamamaraang ito ay nakatuon sa pagpapanatili ng galaw ng iyong balikat at pagpapalakas ng mga kalamnan sa paligid nito upang bawasan ang pressure sa joint. Inaasahan naming bibigyan mo ng makatarungang pagkakataon ang conservative care na ito bago isaalang-alang ang mas invasive na mga hakbang. Ito ang pamantayang unang linya ng depensa upang tulungan kang pamahalaan ang sakit at mapanatili ang function nang hindi kailangang pumasok sa operasyon.
Kung hindi sapat ang banayad na paggalaw at mga ehersisyo, tinitingnan namin ang medikal na pamamahala upang kontrolin ang iyong mga sintomas. Karaniwang kasama nito ang gamot pang-alis ng sakit at anti-inflammatories upang bawasan ang pamamaga at hindi kasiyahan. Maaari ring talakayin ng iyong surgeon ang mga injection. Ang mga cortisone shot ay maaaring magbigay ng malaking pagpapagaan ng sakit sa limitadong panahon, na tumutulong sa iyo na bumalik sa mga araw-araw na gawain. Ang ibang mga opsyon tulad ng mga injection ng hyaluronic acid o platelet-rich plasma (PRP) ay minsan ginagamit upang lubrikahan ang joint o hikayatin ang paggaling, bagama't magkakaiba ang tagal ng epekto nito. Ang mga treatment na ito ay hindi nagpapagaling sa arthritis, ngunit maaari itong magbigay ng oras at mapabuti ang iyong kalidad ng buhay habang pinamamahalaan mo ang kondisyon.
Ang surgery ay itinuturing lamang kapag naabot na ng conservative care ang hangganan nito at nananatiling severe ang iyong sakit. Sa yugtong ito, maaaring irekomenda ng iyong surgeon ang shoulder replacement, kilala rin bilang arthroplasty. Ang prosedurang ito ay pumapalit sa mga sira na bahagi ng iyong joint ng artificial na mga komponente upang ibalik ang makinis na paggalaw at alisin ang sakit. Ang tiyak na uri ng replacement ay nakadepende sa kalusugan ng iyong rotator cuff at sa lawak ng pinsala sa buto. Halimbawa, ang anatomic total shoulder replacement ang benchmark kung intact ang iyong rotator cuff, habang ang reverse total shoulder replacement ay madalas ginagamit para sa mas kumplikadong mga kaso na may kasamang pinsala sa cuff. Ang mga surgical treatment na ito ay itinuturing na epektibo para sa mga severe na kaso at maaaring mag-alok ng malaki at matibay na pagpapabuti sa iyong kakayahang gumamit ng iyong braso.
Ano ang inaasahan¶
Ang arthritis ng balikat ay isang karaniwang kondisyon na nagdudulot ng pagkasira ng mga ibabaw ng kasukasuan. Kung walang gamot, madalas na nananatili at lumalala ang mga sintomas sa paglipas ng panahon. Maraming pasyente ang nakakaranas ng patuloy na sakit at pagkahigpit na nagbabawal sa mga araw-araw na gawain. Kung mayroon kang magaan na mga palatandaan ng arthritis sa mga imahe, humigit-kumulang pito beseng mas malaki ang tsansang maramdaman mong hindi sapat ang tulong ng operasyon kumpara sa mga may malalang arthritis. Ipinapakita nito kung bakit maingat na inaangkop ng iyong doktor ang paggamot sa yugto ng iyong sakit.
Kapag maayos na pinamamahalaan, ang mga opsyon sa operasyon tulad ng pagpapalit ng kasukasuan ay maaaring magbigay ng malaking ginhawa. Karamihan sa mga pasyente ay nakakakita ng malaking pagpapabuti sa sakit at kakayahan. Para sa mga may buong rotator cuff, parehong ang anatomic at reverse joint replacements ay nag-aalok ng magagandang resulta. Ang reverse replacement, partikular, ay nagpapakita ng mababang rate ng komplikasyon sa maikling panahon para sa grupong ito. Kahit na kailangang lumipat ang iyong doktor sa reverse replacement habang nasa operasyon, malamang na katulad ang iyong mga resulta sa mga naka-planong ito mula sa simula.
Iba-iba ang long-term outlook. Habang marami ang nakikinabang ng patuloy na pagpapabuti, nananatiling isang alalahanin ang tibay ng implant, lalo na kung aktibo ka. May ilang pasyente ang patuloy na nakakaranas ng sakit o ng pagkasira ng buto higit sa 10 taon pagkatapos ng ilang uri ng replacement. Bukod dito, humigit-kumulang 16% ng mga pasyente ay nagkakaroon ng arthritis sa acromioclavicular joint (ang bungo sa itaas ng iyong balikat) sa loob ng 12 taon pagkatapos ng anatomic replacement. Ang lakas sa harap na bahagi ng iyong balikat ay maaaring hindi ganap na bumalik sa normal sa loob ng dalawang taon, bagama't malamang na makakakita ka ng pagpapabuti kung saan ka nagsimula.
Ang paggaling ay isang proseso, hindi isang solong pangyayari. Dapat mong inaasahan ang unti-unting pag-unlad sa loob ng mga linggo at buwan. Habang karaniwang bumababa ang sakit, kailangan ng oras upang muling mabuo ang buong lakas. Gabay ng iyong doktor ang iyong paglalakbay sa prosesong ito, ngunit ang pag-unawa na ang ilang limitasyon o hindi komportableng pakiramdam ay maaaring manatili ay tumutulong upang itakda ang makatotohanang inaasahan. Ang layunin ay muling ibalik ang kakayahan at bawasan ang sakit, upang makabalik ka sa mga gawaing pinakamahalaga sa iyo.
Kailan kumonsulta sa doktor¶
Karaniwan ang arthritis ng balikat at madalas itong lumala habang tumatanda. Kumsulta sa iyong doktor kung mayroon kang patuloy na sakit na hindi gumagaling kahit magpahinga. Magpakonsulta sa espesyalista kung nararamdaman mo ang kahinaan, kawalan ng katatagan, o kung nakakabit o bumabagsak ang iyong balikat. Maaaring makapagpahirap ang mga sintomas na ito sa pagtulog o sa trabaho. Ang biglaang paglala ng sakit ay nangangailangan ng pansin. Lalo itong totoo para sa mga matatandang babae na may tahimik na pagsisimula ng sakit sa balikat, na maaaring magpahiwatig ng mabilis na pagkasira ng arthritis. Maaaring gumamit ang iyong surgeon ng imahen upang kilalanin kung ito ay impeksyon o arthritis na dulot ng pagkasira. Ang maagang pagsusuri ay tumutulong sa pamamahala ng mga sintomas at pagpaplano ng paggamot, kabilang ang posibleng pagpapalit ng kasu-kasuan.
Evidence & references
Overview¶
- Standardization of outcome assessment following treatment of shoulder arthritis is needed [1].
- Shoulder arthritis is common [2].
- Management strategies for shoulder arthritis, especially in young patients, continue to evolve [2].
- Significant improvements in implant design have occurred for shoulder arthritis management [2].
- Implant longevity remains a concern in more active patients with shoulder arthritis [2].
- Anatomic total shoulder arthroplasty (ATSA) is the benchmark for surgical treatment of glenohumeral arthritis with an intact cuff [19].
- Reverse total shoulder arthroplasty (RTSA) has gained popularity for rotator cuff arthropathy and other complex indications [19].
- Knowledge of the array of shoulder prostheses currently available and their indications can lead to optimized patient outcomes [11].
- Use of treatment algorithms can lead to optimized patient outcomes in shoulder arthroplasty [11].
- Total shoulder arthroplasty did not provide a clinically important advantage over hemiarthroplasty in terms of patient-reported pain, function, or adverse effects [24].
- The evidence comparing total shoulder arthroplasty to hemiarthroplasty is of low quality [24].
- Patients with glenohumeral osteoarthritis converted intraoperatively to reverse shoulder arthroplasty (RSA) had outcomes comparable to those who underwent total shoulder arthroplasty [3].
- Reverse shoulder arthroplasty provides optimal outcomes with low complication rates across a short term of follow-up for glenohumeral osteoarthritis with an intact rotator cuff [4].
- Patients with mild radiographic signs of arthritis have about sevenfold higher odds of failing to achieve the minimum clinically important difference (MCID) after anatomic total shoulder replacement compared to patients with severe arthritis [5].
- The Western Ontario Osteoarthritis of the Shoulder Index (WOOS) is recommended for continued use in shoulder arthroplasty registries and observational studies [7].
- A clear standardized set of shoulder arthroplasty complication definitions is lacking [8].
- Both augmented and standard anatomic total shoulder arthroplasty can provide satisfactory and sustained improvements in patient-reported outcomes in patients with acquired glenoid retroversion due to glenohumeral osteoarthritis [26].
Anatomy & Pathophysiology¶
- Pathoanatomic metrics with identified threshold values can discriminate glenoid types in shoulders with primary glenohumeral osteoarthritis [6].
- Measurement of humeral subluxation in the glenoid hull plane may be more accurate than measurement in the scapular plane [27].
- Scapular kinematics in patients with shoulder arthroplasty are influenced by the implementation of external loads, but not by the type of load [34].
- Scaption kinematics in reverse shoulder arthroplasty do not change after the sixth postoperative month [35].
- Elliptical and spherical humeral heads show similar obligate glenohumeral translation during axial rotation in total shoulder arthroplasty [37].
- Geometric analysis of the prosthetic shoulder is precise [38].
- Reverse total shoulder arthroplasty (RTSA) shoulders maintain the same anterior and posterior deltoid muscle moment-arm patterns as healthy shoulders but exhibit much greater intersubject variation and larger moment-arm magnitudes [41].
- In RTSA, although the teres minor external rotation moment arm is higher than in a normal shoulder, decreased length could impair force generation [42].
- Reverse total shoulder arthroplasty alters humerothoracic, scapulothoracic, and glenohumeral motion during weighted scaption [43].
- Custom, non-spherical prosthetic heads more accurately replicate head shape, rotational range of motion, and glenohumeral joint kinematics compared with commercially available spherical prosthetic heads when compared to the native humeral head [44].
- The scapulothoracic contribution to overall shoulder movement is significantly increased in patients with reverse total shoulder arthroplasty compared with a healthy shoulder [47].
- Shoulders with rotator cuff tears require considerable compensatory deltoid function to prevent abduction motion loss [51].
- Anatomic total shoulder arthroplasty results in tendon-metal contact and higher tendon contact pressures compared to the native shoulder [52].
- The combination of altered resting scapular posture and restricted scapulothoracic range of motion could prohibit glenohumeral rotation required to reach internal rotation in adduction [55].
- Glenosphere configuration can be modified to increase range of movement in reverse shoulder arthroplasty [56].
Classification¶
- Pathoanatomic metrics with identified threshold values can be used to discriminate glenoid types in shoulders with primary glenohumeral osteoarthritis [6].
- Anatomic patterns of glenoid bone loss exist for different classes of glenohumeral arthritis [14].
- Shoulders presenting with posterior subluxation (B types) remained posteriorly subluxed over a decade [18].
- Concentric arthritis developed an eccentric pattern 20% of the time over a decade [18].
- Measurement of humeral subluxation in the glenoid hull plane may be more accurate than in the scapular plane [27].
- A 3-dimensional classification system using combined humeroscapular alignment and glenoid erosion can be applied to describe degenerative glenohumeral arthritis comprehensively [36].
- A small lateral extension and less posterior rotation of the acromion is associated with shoulder osteoarthritis and is present in almost all types and subtypes of glenoid morphology [40].
- Osteoarthritic humeral head morphology varies significantly from normal, characterized by larger spherical diameters [58].
- Osteoarthritic humeral head morphology does not vary as a function of the Walch classification between symmetric and asymmetric glenoids [58].
Clinical Presentation¶
- Shoulder arthritis is a common condition [2].
- Management strategies for shoulder arthritis, particularly in young patients, continue to evolve with significant improvements in implant design, although longevity remains a concern in more active patients [2].
- Patients with mild radiographic signs of arthritis have about sevenfold higher odds of failing to achieve the minimum clinically important difference (MCID) after anatomic total shoulder replacement compared to patients with severe arthritis [5].
- Pathoanatomic metrics with identified threshold values can be used to discriminate glenoid types in shoulders with primary glenohumeral osteoarthritis [6].
- Rapidly destructive arthrosis of the shoulder joints should be considered in the differential diagnosis of elderly women with insidious shoulder pain [10].
- Increased age is the main determinant of radiological changes in shoulder osteoarthritis, as well as pain [12].
- Shoulders presenting with posterior subluxation (B types) remained posteriorly subluxed, while concentric arthritis developed an eccentric pattern 20% of the time over a decade [18].
- Arthritic B2 glenoids are common, and their maximal erosion is usually posteroinferior [48].
- F-18-FDG PET/CT effectively differentiates septic shoulder arthritis from varying stages of osteoarthritis [22].
Investigations¶
- Standardization of outcome assessment is needed following treatment of shoulder arthritis [1].
- Pathoanatomic metrics with identified threshold values can discriminate glenoid types in shoulders with primary glenohumeral osteoarthritis [6].
- Rapidly destructive arthrosis should be considered in the differential diagnosis of elderly women with insidious shoulder pain [10].
- Increased age is the main determinant of radiological changes in shoulder osteoarthritis [12].
- Increased age is the main determinant of pain in shoulder osteoarthritis [12].
- Anatomic patterns of glenoid bone loss exist for different classes of glenohumeral arthritis [14].
- F-18-FDG PET/CT effectively differentiates septic shoulder arthritis from varying stages of osteoarthritis [22].
- In healthy/nonosteoarthritic shoulders, increased glenoid retroversion is associated with decreased anterior glenoid offset [31].
- Additional research is required to document the clinical value of new technologies to patients with glenohumeral arthritis [32].
- MRI offers a more precise method of determining glenoid version compared with x-ray imaging for preoperative osseous imaging in total shoulder arthroplasty [57].
- The critical shoulder angle is an effective radiographic parameter associated with rotator cuff tears and osteoarthritis [63].
- Three-dimensional CT reconstruction allows for reliable evaluation of the scapulohumeral relationship [64].
- Three-dimensional CT reconstruction reveals significant posterior translation of the humeral head in osteoarthritic shoulders compared to nonpathologic controls [64].
- Significant posterior translation of the humeral head in osteoarthritic shoulders supports the pathomechanism of glenoid component loosening [64].
- A quantitative method for determining medial migration of the humeral head on plain radiographs is inexpensive, practical, and reproducible after shoulder arthroplasty [67].
- Cystic disease in the glenoid did not affect functional outcome after total shoulder arthroplasty with minimum 5-year follow-up [68].
- Cystic disease in the glenoid did not affect the presence of radiographic glenoid loosening after total shoulder arthroplasty with minimum 5-year follow-up [68].
- Three significantly differently oriented posterior erosion patterns (posterior-superior, posterior-central, and posterior-inferior) were distinguished in shoulders demonstrating posterior wear on axillary imaging [69].
Treatment¶
Non-Operative Management¶
- Nonoperative modalities should be utilized before surgical options, particularly for patients with moderate-to-mild shoulder osteoarthritis [17].
Surgical Management: General Principles and Indications¶
- Anatomic total shoulder arthroplasty (ATSA) is the benchmark for surgical treatment of glenohumeral arthritis with an intact rotator cuff [19].
- Reverse total shoulder arthroplasty (RTSA) has gained popularity for rotator cuff arthropathy and other complex indications [19].
- Surgical treatments like arthroplasty are considered effective for severe cases of shoulder osteoarthritis [17].
- Knowledge of the array of shoulder prostheses currently available and the indications for each, as well as the use of treatment algorithms, can lead to optimized patient outcomes [11].
- Shoulder arthritis is common, and management strategies, especially in young patients, continue to evolve with significant improvements in implant design [2].
- Longevity of implants remains a concern in more active patients with shoulder arthritis [2].
Surgical Management: Anatomic Total Shoulder Arthroplasty (ATSA)¶
- Patients with mild radiographic signs of arthritis have about sevenfold higher odds of failing to achieve the minimum clinically important difference (MCID) after anatomic total shoulder replacement compared to patients with severe arthritis [5].
- Both augmented and standard anatomic total shoulder arthroplasty can provide satisfactory and sustained improvements in patient-reported outcomes in patients with acquired glenoid retroversion due to glenohumeral osteoarthritis [26].
- There was no clinically or statistically significant difference in the Oxford Shoulder Score results between groups with and without glenoid cementation in total shoulder arthroplasty for degenerative arthritis of the shoulder [28].
- Total shoulder arthroplasty (TSA) is superior to hemiarthroplasty for treating end-stage glenohumeral arthritis refractory to conservative treatment in patients 30 to 50 years old, resulting in greater cost savings, fewer revision procedures, and greater quality-adjusted life years (QALYs) gained [65].
Surgical Management: Reverse Total Shoulder Arthroplasty (RTSA)¶
- Patients with glenohumeral osteoarthritis converted intraoperatively to reverse shoulder arthroplasty (RSA) had outcomes comparable to those who underwent total shoulder arthroplasty [3].
- Reverse shoulder arthroplasty provides optimal outcomes with low complication rates across a short term of follow-up for glenohumeral osteoarthritis with an intact rotator cuff [4].
Surgical Management: Surface Replacement Arthroplasty¶
- Cemented surface replacement arthroplasty (CSRA) provides good long-term symptomatic and functional results in the treatment of glenohumeral arthropathy in patients aged younger than 50 years in 81.6% of the patients [9].
- Patients undergoing total shoulder arthroplasty with an asymmetric glenoid component for osteoarthritis achieve satisfactory mid-term pain relief and improvement in function; however, instability is not always corrected [50].
Surgical Management: Arthroscopic and Other Procedures¶
- The authors recommend a systematic, inclusive approach to the array of pathologies encountered in the setting of early glenohumeral arthritis known as the Comprehensive Arthroscopic Management (CAM) procedure [16].
- Scapulothoracic fusion resulted in improvements in functional outcomes scores, with most patients meeting or exceeding the minimum clinically important difference for recalcitrant scapular winging [53].
Outcome Assessment and Registry Data¶
- The Western Ontario Osteoarthritis of the Shoulder Index (WOOS) is recommended for continued use in shoulder arthroplasty registries and observational studies [7].
- The PROMIS Global-10 appears to have limited utility in the evaluation of patients with shoulder arthritis both preoperatively and after total shoulder arthroplasty [33].
- A study of 1,270 individual patients from eleven centers demonstrated significant improvement in patient-reported outcomes at 1 and 2 years post-surgery for a polyethylene glenoid with a fluted peg, establishing a benchmark for early clinical value [54].
Standardization and Complications¶
- There is a need for standardization of outcome assessment following treatment of shoulder arthritis [1].
- A clear standardized set of shoulder arthroplasty complication definitions is lacking [8].
Complications¶
- Standardized definitions for shoulder arthroplasty complications are lacking [8].
- Standardization of outcome assessment following treatment of shoulder arthritis is needed [1].
- Longevity of implants remains a concern in more active patients with shoulder arthritis [2].
- Total shoulder arthroplasty is associated with high mid-term complication rates due to instability and loosening in B2 glenoids [45].
- Symptomatic acromioclavicular joint osteoarthritis occurred in 15.9% of patients after total anatomic shoulder replacement with follow-up of up to 12 years [15].
- No case of glenoid loosening occurred at 3 years' follow-up in revision arthroplasty with a hip-inspired computer-assisted design/computer-assisted manufacturing implant for glenoid-deficient shoulders [21].
- Total shoulder arthroplasty did not provide a clinically important advantage over hemiarthroplasty in terms of adverse effects, although the evidence was of low quality [24].
Recovery¶
- Standardization of outcome assessment is needed following treatment of shoulder arthritis [1].
- Implant longevity remains a concern in more active patients with shoulder arthritis [2].
- Patients with glenohumeral osteoarthritis converted intraoperatively to reverse shoulder arthroplasty (RSA) had outcomes comparable to those who underwent total shoulder arthroplasty (TSA) [3].
- Reverse shoulder arthroplasty provides optimal outcomes with low complication rates across a short term of follow-up for glenohumeral osteoarthritis with an intact rotator cuff [4].
- Primary anatomic total shoulder arthroplasty (aTSA) and reverse total shoulder arthroplasty (rTSA) patients with osteoarthritis and an intact rotator cuff with no previous history of shoulder surgery had similar clinical and radiographic outcomes at a mean of 41 months follow-up [23].
- Surgeons may consider using reverse arthroplasty in cases of primary shoulder arthritis with a critical shoulder angle of 35 degrees or greater [29].
- The PROMIS Global-10 has limited utility in the evaluation of patients with shoulder arthritis both preoperatively and after TSA [33].
- Subscapularis strength returned to normal in only a minority of patients at 2 years after shoulder arthroplasty, although significant strength improvement from baseline was observed [60].
- There is a substantive subgroup with continuing pain and a high rate of glenoid bone erosion after 10 years following humeral head replacement for osteoarthritis [70].
Key Evidence¶
- [L1] The present review highlights the need for standardization of outcome assessment following treatment of shoulder arthritis. (10.1177/1758573215622385)
- [L5] Shoulder arthritis is common, and management strategies, especially in young patients, continue to evolve with significant improvements in implant design, though longevity remains a concern in more active patients. (10.1016/j.csm.2018.07.001)
- [L3] Patients with glenohumeral osteoarthritis converted intraoperatively to RSA had outcomes comparable to those who underwent total shoulder arthroplasty. (10.1016/j.jse.2015.01.005)
- [L4] Reverse shoulder arthroplasty provides optimal outcomes with low complication rates across a short term of follow-up for glenohumeral osteoarthritis with an intact rotator cuff. (10.1016/j.jse.2021.06.010)
- [Paper] Patients with mild radiographic signs of arthritis have about sevenfold higher odds of failing to achieve the minimum clinically important difference (MCID) after anatomic total shoulder replacement compared to patients with severe arthritis. (10.1097/corr.0000000000002747)
- [L4] Pathoanatomic metrics with the identified threshold values can be used to discriminate glenoid types in shoulders with primary glenohumeral osteoarthritis. (10.1016/j.jse.2021.03.140)
- [L4] The authors recommend the continued use of WOOS in shoulder arthroplasty registries and observational studies. (10.1186/s12891-023-06578-5)
- [L1] A clear standardised set of shoulder arthroplasty complication definitions is lacking. (10.1007/s00402-017-2635-9)
- [L4] CSRA provides good long-term symptomatic and functional results in the treatment of glenohumeral arthropathy in patients aged younger than 50 years in 81.6% of the patients. (10.1016/j.jse.2014.11.035)
- [L4] This condition should be considered in the differential diagnosis of elderly women with insidious shoulder pain. (10.1016/j.jse.2014.10.020)
- [L5] Knowledge of the array of shoulder prostheses currently available and the indications for each, as well as the use of treatment algorithms, can lead to optimized patient outcomes. (10.5435/00124635-200907000-00002)
- [L3] This study shows that increased age is the main determinant of radiological changes in shoulder OA, as well as pain. (10.1186/s13018-022-03137-x)
- [L4] These data demonstrate an anatomic pattern of glenoid bone loss for different classes of glenohumeral arthritis. (10.1007/s12306-016-0406-3)
- [L4] Symptomatic ACJ OA occurred in 15.9% of patients after total anatomic shoulder replacement with follow-up of up to 12 years. (10.1177/17585732221114796)
- [L4] The authors recommend a systematic, inclusive approach to the array of pathologies encountered in the setting of early glenohumeral arthritis: the Comprehensive Arthroscopic Management (CAM) procedure. (10.1016/j.arthro.2022.01.033)
- [L5] The article provides an overview of available treatments for shoulder osteoarthritis, noting that nonoperative modalities should be utilized before surgical options, particularly for patients with moderate-to-mild disease, while surgical treatments like arthroplasty are considered effective for severe cases. (10.1155/2013/370231)
- [L4] Shoulders presenting with posterior subluxation (B types) remained posteriorly subluxed, while concentric arthritis developed an eccentric pattern 20% of the time. (10.1016/j.jse.2020.05.021)
- [L4] At 3 years' follow-up, pain and clinical scores improved significantly and no case of glenoid loosening occurred. (10.1016/j.jse.2013.05.004)
- [L3] F-18-FDG PET/CT effectively differentiates septic shoulder arthritis from varying stages of osteoarthritis. (10.1016/j.jse.2025.01.047)
- [L3] At a mean of 41 month follow-up, primary aTSA and rTSA patients with OA and an intact rotator cuff with no previous history of shoulder surgery had similar clinical and radiographic outcomes. (10.5435/jaaos-d-22-00014)
- [L1] Total shoulder arthroplasty did not provide a clinically important advantage over hemiarthroplasty in terms of patient-reported pain, function, nor adverse effects; however, the evidence on this topic was of low quality. (10.1097/corr.0000000000001523)
- [L3] Both augmented and standard anatomic total shoulder arthroplasty can provide satisfactory and sustained improvements in patient-reported outcomes in patients with acquired glenoid retroversion due to glenohumeral osteoarthritis. (10.1016/j.jse.2021.12.016)
- [L4] Measurement in the glenoid hull plane may be more accurate than in the scapular plane. (10.1016/j.jse.2017.01.027)
- [L3] There was no clinically or statistically significant difference in the Oxford Shoulder Score results between the two groups. (10.1016/j.jse.2013.08.022)
- [L3] These data suggest that surgeons may consider using reverse arthroplasty in cases of primary shoulder arthritis with a critical shoulder angle of 35 degrees or greater. (10.1016/j.jse.2021.08.003)
- [L4] In healthy/nonosteoarthritic shoulders, an increased glenoid retroversion is associated with a decreased anterior glenoid offset. (10.1016/j.jse.2023.09.031)
- [L4] Additional research is required to document the clinical value of these new technologies to patients with glenohumeral arthritis. (10.2106/jbjs.20.01853)
- [L3] The Global-10 appears to have limited utility in the evaluation of patients with shoulder arthritis both preoperatively and after TSA. (10.1016/j.jse.2020.10.021)
- [L4] Scapular kinematics of patients with shoulder arthroplasty was influenced by implementation of external loads, but not by the type of load. (10.1016/j.clinbiomech.2012.04.009)
- [L4] Scaption kinematics of reverse shoulder arthroplasty do not change after the sixth postoperative month. (10.1016/j.clinbiomech.2018.07.005)
- [L3] The 3D classification system using combined humeroscapular alignment and glenoid erosion can be applied to describe the disease comprehensively. (10.1177/23259671221110512)
- [L5] A gained understanding of the consequences of implant head shape in TSA may guide future surgical implant choice for better recreation of native shoulder kinematics and potentially improved patient outcomes. (10.1186/s12891-023-06273-5)
- [L2] Geometric analysis of the prosthetic shoulder is precise. (10.1007/s00402-012-1580-x)
- [L3] A small lateral extension and less posterior rotation of the acromion is associated with shoulder osteoarthritis and is present in almost all types and subtypes of glenoid morphology. (10.1016/j.jse.2021.01.018)
- [L5] RTSA shoulders maintain the same anterior and posterior deltoid muscle moment-arm patterns as healthy shoulders but show much greater intersubject variation and larger moment-arm magnitudes. (10.1016/j.jse.2015.09.015)
- [L5] Even if TM external rotation moment arm is higher in RTSA than in a normal shoulder, the decreased length could impair its force generation. (10.1016/j.jse.2014.08.019)
- [L5] This commentary highlights that reverse total shoulder arthroplasty alters humerothoracic, scapulothoracic, and glenohumeral motion during weighted scaption, emphasizing the need to integrate biomechanical studies, computer modeling, and dynamic clinical evaluations to develop a roadmap for precision rTSA. (10.1097/corr.0000000000002383)
- [L5] The custom, non-spherical prosthetic head more accurately replicated the head shape, rotational range of motion, and glenohumeral joint kinematics than the commercially available, spherical prosthetic head compared with the native humeral head. (10.1016/j.jse.2013.01.002)
- [L5] Total shoulder arthroplasty may have reasonable short-term results but is associated with high mid-term complication rates due to instability and loosening in B2 glenoids. (10.1016/j.jse.2013.06.017)
- [L4] The ST contribution to overall shoulder movement is significantly increased in patients with an rTSA compared with a healthy shoulder. (10.1016/j.jse.2024.12.018)
- [L4] Arthritic B2 glenoids are common, and their maximal erosion is usually posteroinferior. (10.1016/j.jse.2015.01.007)
- [L4] Patients undergoing total shoulder arthroplasty with an asymmetric glenoid component for osteoarthritis achieve satisfactory mid-term pain relief and improvement in function; however, instability is not always corrected. (10.1007/s11999-007-0104-4)
- [L5] Shoulders with rotator cuff tears require considerable compensatory deltoid function to prevent abduction motion loss. (10.1177/0363546518768276)
- [L5] Anatomic total shoulder arthroplasty results in tendon-metal contact and higher tendon contact pressures compared to the native shoulder. (10.1016/j.jse.2018.04.017)
- [L4] Scapulothoracic fusion resulted in improvements in functional outcomes scores, with most patients meeting or exceeding the minimum clinically important difference. (10.1097/corr.0000000000002673)
- [L4] The study establishes a benchmark for early clinical value of new glenoid components by demonstrating significant improvement in patient-reported outcomes at 1 and 2 years post-surgery across a large multicenter cohort. (10.1007/s00264-018-4213-3)
- [L4] The combination of altered resting scapular posture and restricted scapulothoracic range of motion could prohibit glenohumeral rotation required to reach internal rotation in adduction. (10.1016/j.jse.2022.10.009)
- [L5] Glenosphere configuration can be modified to increase range of movement in reverse shoulder arthroplasty. (10.1302/0301-620x.100b9.bjj-2018-0264.r1)
- [L3] MRI is useful for preoperative osseous imaging for total shoulder arthroplasty because it offers a more precise method of determining glenoid version compared with x-ray imaging. (10.1016/j.jse.2012.10.036)
- [L4] Osteoarthritic humeral head morphology varies significantly from normal, with larger spherical diameters, but does not vary as a function of the Walch classification between symmetric and asymmetric glenoids. (10.1016/j.jse.2015.08.047)
- [L4] Although significant strength improvement from baseline was observed at 2 years after shoulder arthroplasty, subscapularis strength returned to normal in only a minority of patients. (10.1016/j.jse.2014.06.042)
- [L4] The CSA is an effective radiographic parameter that is associated with rotator cuff tears and osteoarthritis. (10.1136/jisakos-2018-000255)
- [L4] The study demonstrates that 3D CT reconstruction allows for reliable evaluation of the scapulohumeral relationship, revealing significant posterior translation of the humeral head in osteoarthritic shoulders compared to nonpathologic controls, which supports the pathomechanism of glenoid component loosening. (10.1016/j.jse.2016.02.035)
- [L2] Treatment of end-stage glenohumeral arthritis refractory to conservative treatment in patients 30 to 50 years old in the United States with TSA, instead of hemiarthroplasty, would result in greater cost savings, avoid a substantial number of revision procedures, and result in greater years of satisfactory or excellent patient outcomes and greater QALYs gained. (10.1007/s11999-016-4991-0)
- [L3] This is an inexpensive, practical, and reproducible method that can be used to determine the rate of medial migration of the humeral head on plain radiographs after shoulder arthroplasty. (10.1016/j.jse.2010.03.010)
- [L3] Cystic disease did not affect functional outcome or the presence of radiographic glenoid loosening. (10.1016/j.jse.2017.10.035)
- [L4] Three significantly differently oriented wear patterns (posterior-superior, posterior-central, and posterior-inferior) were distinguished in shoulders demonstrating posterior wear on axillary imaging. (10.1016/j.jse.2021.04.028)
- [L4] However, there is a substantive subgroup with continuing pain and a high rate of glenoid bone erosion after 10 years. (10.1016/j.jse.2017.10.017)
References¶
[1] Is there sufficient evidence to support intervention to manage shoulder arthritis?. Shoulder & Elbow. 2016. DOI: 10.1177/1758573215622385 [2] Shoulder Arthritis in the Young and Active Patient. Clinics in Sports Medicine. 2018. DOI: 10.1016/j.csm.2018.07.001 [3] Outcome and value of reverse shoulder arthroplasty for treatment of glenohumeral osteoarthritis: a matched cohort. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2015.01.005 [4] Glenohumeral osteoarthritis with intact rotator cuff treated with reverse shoulder arthroplasty: a systematic review. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2021.06.010 [5] Editor’s Spotlight/Take 5: Patients With Mild Osteoarthritis Are Less Likely to Achieve a Clinically Important Improvement in Pain or Function After Anatomic Total Shoulder Arthroplasty. Clinical Orthopaedics & Related Research. 2023. DOI: 10.1097/corr.0000000000002747 [6] Identification of threshold pathoanatomic metrics in primary glenohumeral osteoarthritis. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2021.03.140 [7] Western Ontario Osteoarthritis of the Shoulder Index (WOOS) - a validation for use in proximal humerus fractures treated with arthroplasty. BMC Musculoskeletal Disorders. 2023. DOI: 10.1186/s12891-023-06578-5 [8] Towards standardised definitions of shoulder arthroplasty complications: a systematic review of terms and definitions. Archives of Orthopaedic and Trauma Surgery. 2017. DOI: 10.1007/s00402-017-2635-9 [9] Surface replacement arthroplasty for glenohumeral arthropathy in patients aged younger than fifty years: results after a minimum ten-year follow-up. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2014.11.035 [10] Rapidly destructive arthrosis of the shoulder joints: radiographic, magnetic resonance imaging, and histopathologic findings. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2014.10.020 [11] Shoulder Arthroplasty: Prosthetic Options and Indications. Journal of the American Academy of Orthopaedic Surgeons. 2009. DOI: 10.5435/00124635-200907000-00002 [12] Radiological changes in shoulder osteoarthritis and pain sensation correlate with patients’ age. Journal of Orthopaedic Surgery and Research. 2022. DOI: 10.1186/s13018-022-03137-x [14] Quantitative assessment and characterization of glenoid bone loss in a spectrum of patients with glenohumeral osteoarthritis. MUSCULOSKELETAL SURGERY. 2016. DOI: 10.1007/s12306-016-0406-3 [15] The incidence and treatment of symptomatic acromioclavicular joint osteoarthritis following total shoulder arthroplasty. Shoulder & Elbow. 2022. DOI: 10.1177/17585732221114796 [16] Comprehensive Arthroscopic Management of Shoulder Arthritis. Arthroscopy. 2022. DOI: 10.1016/j.arthro.2022.01.033 [17] Shoulder Osteoarthritis. Arthritis. 2013. DOI: 10.1155/2013/370231 [18] Natural history of glenoid bone loss in primary glenohumeral osteoarthritis: how does bone loss progress over a decade?. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2020.05.021 [19] Chapter 25 Shoulder Arthritis and Arthroplasty. 2020. [21] Revision arthroplasty with a hip-inspired computer-assisted design/computer-assisted manufacturing implant for glenoid-deficient shoulders. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.05.004 [22] 18F-FDG PET/CT for the diagnosis of septic shoulder arthritis: metabolic uptake pattern and diagnostic performance. Journal of Shoulder and Elbow Surgery. 2025. DOI: 10.1016/j.jse.2025.01.047 [23] Comparison of Reverse and Anatomic Total Shoulder Arthroplasty in Patients With an Intact Rotator Cuff and No Previous Surgery. Journal of the American Academy of Orthopaedic Surgeons. 2022. DOI: 10.5435/jaaos-d-22-00014 [24] Cochrane in CORR®: Shoulder Replacement Surgery For Osteoarthritis And Rotator Cuff Tear Arthropathy. Clinical Orthopaedics & Related Research. 2020. DOI: 10.1097/corr.0000000000001523 [26] Mid- to long-term outcomes of augmented and nonaugmented anatomic shoulder arthroplasty in Walch B3 glenoids. Journal of Shoulder and Elbow Surgery. 2022. DOI: 10.1016/j.jse.2021.12.016 [27] Interest in the glenoid hull method for analyzing humeral subluxation in primary glenohumeral osteoarthritis. Journal of Shoulder and Elbow Surgery. 2017. DOI: 10.1016/j.jse.2017.01.027 [28] Effect of glenoid cementation on total shoulder arthroplasty for degenerative arthritis of the shoulder: a review of the New Zealand National Joint Registry. Journal of Shoulder and Elbow Surgery. 2014. DOI: 10.1016/j.jse.2013.08.022 [29] The association between critical shoulder angle and revision following anatomic total shoulder arthroplasty: a matched case-control study. Journal of Shoulder and Elbow Surgery. 2022. DOI: 10.1016/j.jse.2021.08.003 [31] Three-dimensional evaluation of the transverse rotator cuff muscle's resultant force angle in relation to scapulohumeral subluxation and glenoid vault morphology in nonpathological shoulders. Journal of Shoulder and Elbow Surgery. 2024. DOI: 10.1016/j.jse.2023.09.031 [32] Assessing the Value to the Patient of New Technologies in Anatomic Total Shoulder Arthroplasty. Journal of Bone and Joint Surgery. 2021. DOI: 10.2106/jbjs.20.01853 [33] PROMIS Global-10 performs poorly relative to legacy shoulder instruments in patients undergoing total shoulder arthroplasty for glenohumeral arthritis. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2020.10.021 [34] Kinematic evaluation of patients with total and reverse shoulder arthroplasty during rehabilitation exercises with different loads. Clinical Biomechanics. 2012. DOI: 10.1016/j.clinbiomech.2012.04.009 [35] Scaption kinematics of reverse shoulder arthroplasty do not change after the sixth postoperative month. Clinical Biomechanics. 2018. DOI: 10.1016/j.clinbiomech.2018.07.005 [36] A 3-Dimensional Classification for Degenerative Glenohumeral Arthritis Based on Humeroscapular Alignment. Orthopaedic Journal of Sports Medicine. 2022. DOI: 10.1177/23259671221110512 [37] Elliptical and spherical heads show similar obligate glenohumeral translation during axial rotation in total shoulder arthroplasty. BMC Musculoskeletal Disorders. 2023. DOI: 10.1186/s12891-023-06273-5 [38] Precision of novel radiological methods in relation to resurfacing humeral head implants: assessment by radiostereometric analysis, DXA, and geometrical analysis. Archives of Orthopaedic and Trauma Surgery. 2012. DOI: 10.1007/s00402-012-1580-x [40] Determination of predisposing scapular anatomy with a statistical shape model—Part II: shoulder osteoarthritis. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2021.01.018 [41] How do deltoid muscle moment arms change after reverse total shoulder arthroplasty?. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2015.09.015 [42] The effect of humeral version on teres minor muscle moment arm, length, and impingement in reverse shoulder arthroplasty during activities of daily living. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2014.08.019 [43] CORR Insights®: Reverse Total Shoulder Arthroplasty Alters Humerothoracic, Scapulothoracic, and Glenohumeral Motion During Weighted Scaption. Clinical Orthopaedics & Related Research. 2022. DOI: 10.1097/corr.0000000000002383 [44] The effects of prosthetic humeral head shape on glenohumeral joint kinematics: a comparison of non-spherical and spherical prosthetic heads to the native humeral head. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.002 [45] Current concepts in the surgical management of primary glenohumeral arthritis with a biconcave glenoid. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.06.017 [47] Involvement of the scapulothoracic articulation after well-functioning reverse total shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2025. DOI: 10.1016/j.jse.2024.12.018 [48] Quantification of B2 glenoid morphology in total shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2015.01.007 [50] Augmented Glenoid Component for Bone Deficiency in Shoulder Arthroplasty. Clinical Orthopaedics & Related Research. 2008. DOI: 10.1007/s11999-007-0104-4 [51] Relationship Between Deltoid and Rotator Cuff Muscles During Dynamic Shoulder Abduction: A Biomechanical Study of Rotator Cuff Tear Progression. The American Journal of Sports Medicine. 2018. DOI: 10.1177/0363546518768276 [52] Rotator cuff contact pressures at the tendon-implant interface after anatomic total shoulder arthroplasty using a metal-backed glenoid component. Journal of Shoulder and Elbow Surgery. 2018. DOI: 10.1016/j.jse.2018.04.017 [53] Which Components of the Simple Shoulder Test Show Improvement After Scapulothoracic Fusion for Recalcitrant Scapular Winging? Clinical Results at a Minimum of 5 Years of Follow-up. Clinical Orthopaedics & Related Research. 2023. DOI: 10.1097/corr.0000000000002673 [54] One and two-year clinical outcomes for a polyethylene glenoid with a fluted peg: one thousand two hundred seventy individual patients from eleven centers. International Orthopaedics. 2018. DOI: 10.1007/s00264-018-4213-3 [55] High and low performers in internal rotation after reverse total shoulder arthroplasty: a biplane fluoroscopic study. Journal of Shoulder and Elbow Surgery. 2023. DOI: 10.1016/j.jse.2022.10.009 [56] Glenosphere design affects range of movement and risk of friction-type scapular impingement in reverse shoulder arthroplasty. The Bone & Joint Journal. 2018. DOI: 10.1302/0301-620x.100b9.bjj-2018-0264.r1 [57] Magnetic resonance scanning vs axillary radiography in the assessment of glenoid version for osteoarthritis. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2012.10.036 [58] A comparison of normal and osteoarthritic humeral head size and morphology. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2015.08.047 [60] The return of subscapularis strength after shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2014.06.042 [63] Critical shoulder angle is an effective radiographic parameter that is associated with rotator cuff tears and osteoarthritis: a systematic review. Journal of ISAKOS. 2019. DOI: 10.1136/jisakos-2018-000255 [64] A three-dimensional comparative study on the scapulohumeral relationship in normal and osteoarthritic shoulders. Journal of Shoulder and Elbow Surgery. 2016. DOI: 10.1016/j.jse.2016.02.035 [65] Economic Decision Model Suggests Total Shoulder Arthroplasty is Superior to Hemiarthroplasty in Young Patients with End-stage Shoulder Arthritis. Clinical Orthopaedics & Related Research. 2016. DOI: 10.1007/s11999-016-4991-0 [67] A quantitative method for determining medial migration of the humeral head after shoulder arthroplasty: preliminary results in assessing glenoid wear at a minimum of two years after hemiarthroplasty with concentric glenoid reaming. Journal of Shoulder and Elbow Surgery. 2011. DOI: 10.1016/j.jse.2010.03.010 [68] Total shoulder arthroplasty with minimum 5-year follow-up: does the presence of subchondral cysts in the glenoid increase risk of failure?. Journal of Shoulder and Elbow Surgery. 2018. DOI: 10.1016/j.jse.2017.10.035 [69] Biconcave glenoids show 3 differently oriented posterior erosion patterns. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2021.04.028 [70] Long-term outcomes of humeral head replacement for the treatment of osteoarthritis; a report of 44 arthroplasties with minimum 10-year follow-up. Journal of Shoulder and Elbow Surgery. 2018. DOI: 10.1016/j.jse.2017.10.017