Patients › Rehabilitation
Proksimal Humerus Fixation (ORIF)
Rehabilitation after locking-plate fixation of a proximal humerus fracture, gated on radiographic healing at review.
Ang protocol na ito ay sumasaklaw sa rehabilitasyon pagkatapos ng pagsusuri ng fracture ng proximal humerus (basag ng buto ng itaas na braso malapit sa balikat, na naayos gamit ang locking plate at mga turnilyo, open reduction at internal fixation, ORIF) kay Dr. Kieran Hirpara sa Mater Private Hospital Rockhampton. Dalhin ang pahinang ito o ang PDF nito sa iyong unang bisita sa physiotherapy upang manatiling koordinado ang iyong rehabilitasyon. Ang iyong rehabilitasyon ay ipinapasa-paso ng iyong physiotherapist sa mga yugto sa ibaba, depende sa kung paano gumagaling ang iyong fracture.
Kung mayroon kang anumang alalahanin tungkol sa iyong sugat pagkatapos ng operasyon, makipag-ugnayan sa mga kwarto. Madalas ay nakakatulong na kumuha ng litrato ng sugat at ipadala ito sa pamamagitan ng email para sa pagsusuri.
Ano ang inaasahan¶
Ang rehabilitasyon pagkatapos ng operasyon para sa pagtitiyak ng fracture ay nagkakaiba sa rehabilitasyon pagkatapos ng karamihan sa mga nakaplano na operasyon sa balikat. Ang plate at mga turnilyo ang nag-aayos ng basag na buto sa tamang posisyon, ngunit ang buto mismo ay kailangan pa ring gumaling, at ang bilis ng paggaling ay malaki ang pagkakaiba mula sa isang tao patungo sa isa. Dahil dito, ang talahanayan sa ibaba ay isang karaniwang gabay kaysa sa isang nakatakdang iskedyul: ang bawat hakbang sa iyong programa ay nakadepende sa bilang ng linggo mula sa operasyon at sa kung paano gumagaling ang fracture sa iyong mga X-ray, ayon sa kumpirmasyon sa iyong mga review kay Dr. Hirpara. Huwag kang gumalaw patungo sa susunod na yugto lamang base sa kalendaryo; hintayin ang iyong review.
May isa pang bagay na nagpapakita ng pagkakaiba ng operasyong ito. Ang mga butong protuberance sa itaas ng humerus (ang tuberosities) ang kung saan dumidikit ang mga tendon ng rotator cuff, at sa maraming fracture ng proximal humerus, ang mga fragment na ito ay bahagi ng basag at inayos pabalik gamit ang plate o mga tahi. Ang sobrang pagtrabaho ng mga kalamnan ng rotator cuff nang masyadong maaga ay maaaring humila sa mga fragment na ito bago pa sila gumaling. Sa isang modernong locking plate, ang pag-aayos ay matibay mula sa unang araw, kaya't pinapayagan ang maagang banayad na paggalaw: maaari kang gumalaw ng shoulder nang active-assisted at banayad na active sa loob ng limitasyon ng kaginhawaan mula sa maagang panahon, pagtaas ng braso sa isang range na walang sakit. Ang maingat na elemento ay ang pag-load ng rotator-cuff: kung ang mga fragment ng tuberosity ay hindi bahagi ng fracture, o ay solidong na-fix, maaaring bigyan ka ng surgeon ng pahintulot na magsimula nang mas maaga sa active rotation at trabaho ng cuff; kung ang mga tuberosities ay kasangkot at gumagaling, ang active na trabaho ng rotator-cuff at ang pinilit na outward rotation ay hahadlangan nang kaunti pang mas matagal. Ipapaliwanag ni Dr. Hirpara kung alin ang angkop sa iyo.
Ang iyong programang ehersisyo ay gumagamit ng tatlong uri ng paggalaw, at ang iyong team ang magtatakda kung alin ang angkop sa iyo:
- Active range of motion: pinapayagan ang paggalaw nang walang tulong o tulong.
- Active-assisted range of motion: gumagamit ng kabilang braso o bagay upang tumulong sa paggalaw ng braso.
- Passive range of motion: ganap na nakarelaks, gumagamit ng kabilang braso o puwersa upang gawin ang 100% ng trabaho.
Gising ka mula sa operasyon na may braso sa loob ng sling. Suotin ito nang buong-oras sa unang tatlong linggo o kaya, pagkatapos ay unti-unting bawasan ang paggamit nito sa mga sumusunod na linggo ayon sa kaginhawaan; ang mga publikadong protokol ay karaniwang tatlong linggo ng immobilisation, at ang ebidensya ay sumusuporta sa mas maagang paggalaw kaysa sa mas mahabang panahon sa sling. Hindi mo kailangang matulog na may suot na ito. Tangkilikin ito nang ilang beses sa isang araw para sa iyong mga ehersisyo at para sa paghuhugas at pagdadaan, at kapag nakaupo nang tahimik sa bahay, maaari mong pahinga ang braso labas ng sling. Huwag magmaneho habang suot mo ang sling.
Ang paglalakbay sa isang tingin:
- Yugto I — Proteksyon at maagang passive movement: linggo 0–6
- Yugto II — Pagbawi ng active movement: linggo 6–12
- Yugto III — Pagpapalakas: mga buwan 3 hanggang 4½
- Yugto IV — Pagbabalik sa buong aktibidad: mula sa mga 4½–6 buwan
Yugto I — Proteksyon at maagang pasibong paggalaw (Linggo 0–6)¶
Ang unang anim na linggo ay nakatuon sa pagprotekta sa nakafix na fracture habang pinipigilan ang pagiging matigas ng natitirang bahagi ng braso (at ng sariling shoulder joint). Dahil ang locking plate ay nag-iingat sa buto mula pa noong simula, ang banayad na maagang paggalaw ay inirerekomenda imbes na maghintay ng anim na linggo. Isang physiotherapist ang magpapatunog sa iyo ng mga banayad na ehersisyo bago ka lumabas sa ospital: pendulum exercises (pagpapahinga ng braso at banayad na pag-ikot sa pamamagitan ng pag-ikot ng katawan), at pagpapanatili ng paggalaw ng siko, pulso, at kamay labas ng sling nang ilang beses sa isang araw. Mula sa maagang yugto, at sa loob ng isang komportableng saklaw na walang sakit, maaari ka nang simulan ang paggalaw ng braso gamit ang tulong ng iyong ibang kamay (active-assisted) at banayad sa sarili nitong lakas (active), itaas ito sa harap ng iyong katawan ayon sa iyong kagustuhan. Ang bahaging kailangan ng pag-iingat ay ang pag-load ng rotator cuff: iwasan ang pilit na pag-ikot ng braso palabas (external rotation) at iwasan ang resisted rotator-cuff work hanggang sa gumaling ang iyong tuberosities, gaya ng kumpirma ni Dr. Hirpara. Gumamit ng yelo para sa pagpapagaan ng sakit, at kumain ng iyong painkillers bago ang iyong mga ehersisyo at appointment sa physiotherapy.
Para sa iyong physiotherapist:
Mga Layunin
- Protektahan ang fixation at i-optimize ang paggaling ng buto
- Ayusin ang sakit at pamamaga
- Itatag ang maagang active-assisted na naglalakbay patungo sa active elevation sa loob ng isang saklaw na walang sakit
- Panatilihin ang buong galaw ng leeg, siko, pulso, at kamay
Pamamahala
- Buong oras na suot ang sling ng ~3 linggo, pagkatapos ay unti-unting bawasan ayon sa kagustuhan (konbensyon sa literatura); alisin nang ilang beses sa isang araw para sa mga ehersisyo at hygiene; hindi kinakailangan habang nakahiga
- Pendulum / Codman exercises nang ilang beses sa isang araw
- Maagang active-assisted at banayad na active forward elevation sa loob ng isang komportableng saklaw na walang sakit mula sa simula para sa stable fixation; elevation na nagsisimula sa posisyong nakahiga na naglalakbay patungo sa nakatayo ayon sa kontrol; palawakin ang saklaw ayon sa kagustuhan
- Passive range of motion kung kinakailangan kung saan hindi pa natutol ang active: forward elevation sa scapular plane hanggang humigit-kumulang 90°, internal rotation sa tiyan (hindi sa likod ng likod)
- External rotation pinapanatili sa isang banayad na maagang default na humigit-kumulang 30–40° habang ang braso ay nasa gilid; ang surgeon ay maaaring palawakin ito kung ang tuberosities ay hindi involved o solid na fixed
- Aktibong range of motion ng cervical, siko, pulso, at kamay labas ng sling; ball squeezes para sa grip
- Scapular setting at trabaho sa scapular mobility (elevation, depression, retraction, protraction)
- Ang banayad na deltoid at periscapular isometrics ay maaaring ipakilala ayon sa kagustuhan
- Cryotherapy at analgesia bago ang mga session; scar mobilisation at desensitisation kapag ang sugat ay gumaling na
Mga Precautions
- Iwasan ang pilit o resisted external rotation at mabigat na rotator-cuff loading hanggang sa kumpirmahin ang paggaling ng tuberosity (nasa gabay ng surgeon); ang active elevation sa isang saklaw na walang sakit ay pinapayagan
- Walang internal rotation sa likod ng likod; iwasan ang abduction sa coronal plane
- Panatilihin ang maagang paggalaw na walang sakit: banayad at sa loob ng kagustuhan, hindi pilit
- Walang pag-angat na higit sa humigit-kumulang 0.5–1 kg gamit ang operated na braso
- Walang weight-bearing sa pamamagitan ng operated na braso (walang pagtutulak pataas mula sa upuan o kama)
- Walang pagmamaneho habang suot ang sling
- Walang pilit o masakit na paggalaw sa dulo ng saklaw
Mga Kriterya para mag-progress
- Radiographic na ebidensya ng paggaling na naglalakbay, gaya ng kumpirma sa review ni Dr. Hirpara sa humigit-kumulang 6 linggo
- Ang sakit ay maayos na kontrolado
- Buong galaw ng siko, pulso, at kamay ay panatilihin
- Komportableng active-assisted hanggang sa active elevation sa loob ng isang saklaw na walang sakit
Yugong II — Pagbawi ng aktibong galaw (Linggo 6–12)¶
Sa iyong pagsusuri sa humigit-kumulang anim na linggo, titingnan ni Dr Hirpara ang iyong mga X-ray. Kung ang paggaling ay gumagalaw ayon sa inaasahan, titigil ang anumang paggamit ng sling at magsisimula ka na gumalaw ng iyong braso nang sarili, unang may tulong (gamit ang kabilang braso, isang baston, o pulley), pagkatapos ay aktibo. Karaniwang pinakamabuti ang pagsisimula ng aktibong pagtaas ng braso habang nakahiga sa iyong likod, kung saan mas maliit ang epekto ng gravity, at unti-unting lumipat sa pag-upo at pagtayo habang umuunlad ang kontrol. Maaaring magsimula ang mga banayad na ehersisyo para sa pagtatakda ng kalamnan (isometric) para sa rotator cuff sa yugong ito pagkatapos kumpirmihin ni Dr Hirpara ang paggaling; ang mga ehersisyo laban sa resistensya ay darating nang higit pa. Maaari kang bumalik sa pagmamaneho kapag wala ka nang sa sling, may sapat kang galaw at kontrol ng braso upang mamaneho nang ligtas, at hindi ka na kumukuha ng malalakas na gamot sa sakit; kung may pag-aalinlangan, talakayin ito sa iyong pagsusuri.
Para sa iyong pisyoterapeuta:
Mga Layunin
- Ibalik ang buong passive na saklaw ng galaw
- Lumipat mula sa active-assisted papuntang active na saklaw ng galaw sa lahat ng mga plano
- Muling itatag ang normal na scapulohumeral na ritmo at bawasan ang mga compensatory na pattern
- Bumalik sa normal na magaan na mga araw-araw na gawain
Pamamahala
- Ang sling ay ganap na itinatapon sa pinakahuli sa 6-week na pagsusuri
- Active-assisted na saklaw ng galaw: lawn-chair progression, table / wall slides, pulleys, mga ehersisyo sa baston, na lumalampas sa mga limitasyon ng Yugong I ayon sa kaginhawaan
- Active na saklaw ng galaw mula sa humigit-kumulang 6–8 linggo: supine flexion na lumilipat papuntang upright elevation; side-lying external rotation at flexion; low rows / low punch
- Submaximal na rotator cuff at deltoid isometrics mula sa humigit-kumulang 6–8 linggo, kapag ang braso ay nasa gilid, pagkatapos kumpirmihin ang paggaling
- Magaan na elbow isotonics (biceps curls, triceps extensions) at scapular strengthening (retraction, prone rows)
- Glenohumeral at scapulothoracic mobilisation ayon sa kinakailangan, na may pag-progres ng mga grado ayon sa paggaling
- Pagwawasto ng postura; patuloy na init / yelo at analgesia sa paligid ng mga sesyon ayon sa kagustuhan
Mga Paalala
- Walang resisted (isotonic) na pagpapalakas ng rotator cuff hanggang sa kumpirmihin ang union, karaniwang hindi bago ang 8–12 linggo
- Walang pwersadong end-range overpressure o agresibong passive stretching
- Ang pagbuhat ay limitado sa humigit-kumulang 1–2 kg gamit ang operadong braso
- Mag-ingat at wawsitin ang shoulder hitching at trunk-lean compensation sa elevation
Mga Kriteryo para mag-progres
- Buong, o halos buong, passive na saklaw ng galaw
- Aktibong elevation na may magandang mekaniks, hindi bababa sa ilalim ng taas ng balikat
- Mabuting tinatanggap ang isometrics nang walang pagtaas ng sakit
- Ang union ay gumagalaw sa X-ray, ayon sa kumpirmasyon sa iyong pagsusuri kay Dr Hirpara
Yugong III — Pagpapalakas (mga Buwan 3 hanggang 4½)¶
Kapag ang fracture ay nag-ugnay na at bumabalik ang iyong aktibong paggalaw, ang pokus ay lumilipat sa pagpapatibay ng lakas. Ang mga ehersisyong may resistensya ay nagsisimula nang dahan-dahan (gamit ang mga elastic band at magagawang bigat para sa rotator cuff, deltoid, at mga kalamnan ng balikat) at unti-unting pinapalakas. Patuloy ang paghuhubog habang pinapalakas ang ganap na paggalaw sa lahat ng direksyon, kabilang ang pag-abot sa likod ng likod. Ang mga karaniwang gawain sa araw-araw ay dapat na halos bumalik na sa normal sa yugong ito, at mas magaan na mga gawaing pang-libangan ay karaniwang muling sisimulan, ayon sa gabay ng iyong pisyoterapeuta.
Para sa iyong pisyoterapeuta:
Mga Layunin
- Ganap na aktibong saklaw ng paggalaw sa lahat ng mga plano na may normal na mekanika
- Unti-unting pagpapanumbalik ng lakas at katatagan ng rotator cuff, deltoid, at scapular
Pamamahala
- Lumipat mula sa isometrics papunta sa paggamit ng elastic band at pagpapagaan ng free-weight strengthening (mga 0.5–2 kg) para sa cuff, deltoid, at mga scapular stabilisers: mababang load, mas mataas na paulit-ulit (halimbawa, 2–3 sets ng 8–12), mga sesyon ng resistensya tungkol sa 3 beses bawat linggo upang maiwasan ang sobrang pagpapabigat
- Pagpapalakas ng pag-ikot sa simula ay may braso sa gilid, sa ilalim ng taas ng balikat
- Bigyang-diin ang anterior deltoid at ang trapezius–serratus anterior force couple para sa matatag na base ng scapula
- Programa ng flexibility para sa terminal na saklaw sa lahat ng mga plano: posterior capsule (cross-body) stretch, pag-ikot sa loob sa likod ng likod, anterior chest wall / pectoralis minor stretches, doorway stretch
- Magsimula ng internal rotation sa likod ng likod at grade III–IV mobilisations ayon sa saklaw ng paggalaw
- Upper-body ergometer na may mababang resistensya; pangkalahatang kondisyon ng aerobic
Mga Paalala
- Ang pagpapalakas ay mananatili sa komportableng saklaw at hindi dapat magdulot ng sakit na tumatagal
- Walang pag-angat ng higit sa mga 4–5 kg gamit ang operated na braso sa yugong ito
- Iwasan ang sobrang pagpapabigat sa pamamagitan ng braso (mga push-up at katulad ay darating sa huli)
Mga Kriteryo para lumipat
- Ganap na aktibong saklaw ng paggalaw na walang mga estratehiyang pampalit
- Tinatanggap ng programa ng pagpapalakas nang walang pagtaas ng sakit o pagkawala ng saklaw
Yugong IV — Pagbabalik sa buong aktibidad (mula sa humigit-kumulang 4½–6 na buwan)¶
Ang huling yugong ay isang unti-unting pagbabalik sa mas mabigat na pagtaas ng karga, trabahong manual, mga gawain sa itaas ng ulo, at isports. Ang pagsasanay sa lakas ay umaabot sa mas mabigat na resistensya at mga compound na galaw, at, kung angkop sa iyong trabaho o isports, sa mas mabilis at mas dinamikong ehersisyo. Karamihan sa mga tao ay bumabalik sa kanilang karaniwang mga aktibidad sa humigit-kumulang anim na buwan, bagaman ang lakas at kumpiyansa ay karaniwang patuloy na umaunlad hanggang sa isang taon. Ang tamang finish line ay nakadepende sa kung ano ang kailangan gawin ng braso, kaya ang pagbabalik sa mabigat na trabahong manual o sa mga isports na may kontak at sa itaas ng ulo ay kinikilala ni Dr. Hirpara at ng iyong physiotherapist kaysa itakda lamang ng kalendaryo.
Para sa iyong physiotherapist:
Mga Layunin
- Pagbabalik sa buong trabaho, recreational, at sporting na aktibidad
- Lakas ng na-operahang braso na humahapit na sa lakas ng kabilang panig
Pamamahala
- Progressive na resistensya sa pamamagitan ng mga bands, free weights, at mga compound na galaw na batay sa gym
- Pag-unlad ng push-up (pader → bangko → tuhod → buo) at closed-chain stability work ayon sa kakayahang tanggapin
- Mula sa humigit-kumulang 4½ na buwan: eccentric loading, plyometrics (pagtrabaho gamit ang may bigat na bola), proprioceptive, at mga drill para sa rhythmic stabilization kung angkop
- Resisted rotation sa 90° ng elevation, at mga interval na espesipiko sa isports o sa propesyon kung angkop
Mga Paalala
- Ang pag-unlad ay nananatiling gabay ng sintomas: kung magbalik ang sakit o pagkawala ng range, bumagal at ibalik muna ang komportableng galaw
Mga Kriteryo para sa discharge
- Lakas ng na-operahang braso na hindi bababa sa humigit-kumulang 80% ng kabilang panig kung sinusukat
- Walang sakit kasabay ng progressive na pagpapalakas
- Nakakapag-isa sa isang maintenance home program
Pagkatapos ng iyong protokol¶
Ang mga yugto sa itaas ay naangkop mula sa mga publikadong protokol ng rehabilitasyon para sa pag-aayos ng fracture ng proximal humerus: Massachusetts General Brigham Sports Medicine, Twin Cities Orthopedics, ang UConn Musculoskeletal Institute, NYU Langone Orthopedic Center at South Bend Orthopaedics, kasama ang isang systematic review ng rehabilitasyon pagkatapos ng fracture ng proximal humerus. Mas malaki ang pagkakaiba ng mga publikadong protokol para sa operasyong ito kumpara sa karamihan ng mga operasyon sa balikat, dahil ang tamang bilis ay nakadepende sa kung paano naayos ang indibidwal na fracture at kung paano ito gumagaling; kaya ang iyong pag-unlad sa mga yugto ay pinamumunuan ni Dr Hirpara sa iyong mga review at ina-adjust ng iyong physiotherapist sa pagitan ng mga review na iyon. Ang pahinang ito ay kasabay ng pangkalahatang payo sa paggaling ng klinika; tingnan ang pagmamana ng post-operative na sakit at pag-aalaga sa sugat. Para sa operasyon mismo, tingnan ang pag-aayos ng proximal humerus.
Kung gusto mong basahin ang ebidensya sa likod ng protokol na ito (ang pananaliksik tungkol sa maagang kumpara sa pinagda-delay na paggalaw pagkatapos ng plate fixation, ang debate sa pagitan ng operasyon at sling, at ang mga komplikasyon na dinisenyo upang maiwasan ng staged progression), isang buong may sanggunian na buod ng ebidensya ay available bilang PDF kasama ang pahinang ito.
Evidence & references
Proximal Humerus Fracture Fixation (Locking-Plate ORIF) — Post-operative Rehabilitation: Evidence¶
Topic scope: Post-operative rehabilitation after open reduction and internal fixation (ORIF) of a proximal humerus fracture with a locking (angular-stable) plate and screws. This page covers the evidence behind the phased rehabilitation program — early protected/passive motion, deferred active and resisted motion, and graded strengthening — and the surgical-outcome facts that shape it. It does not cover the separate pathways of non-operative fracture management, intramedullary nailing, hemiarthroplasty or reverse total shoulder arthroplasty, although the operative-versus-non-operative debate is summarised because it frames who is offered this operation at all.
Defining principle of the rehab here (mobilise early, protect the tuberosities): A locking plate is an angular-stable construct — the screws lock into the plate, so the fixation holds even in osteoporotic bone without relying on bone-to-screw friction. Because that stability is present from day one, this protocol now permits early active (and active-assisted) shoulder elevation in a pain-free range for stable fixation, consistent with the early-active-motion RCT evidence (Loew 2025), rather than holding the shoulder passive-only for six weeks. The element still keyed to biological healing is rotation and rotator-cuff loading: where the tuberosity fragments to which the rotator cuff attaches are part of the fracture, active/resisted rotation and cuff work are held back until those fragments unite, whereas where the tuberosities are uninvolved or solidly fixed the surgeon may clear cuff loading sooner. The brake is therefore biological, not mechanical — the plate is strong immediately — and it is now selective (rotation/cuff), not a blanket movement ban. Progression of cuff loading remains governed by fracture stability and radiographic healing, not the calendar. This places the protocol close to the early-active-movement end of the spectrum while still being more tuberosity-aware than a pure debridement/decompression, and far less tuberosity-dependent than a fracture arthroplasty, where healing of the tuberosities to the prosthesis dictates a slower, stricter cuff-loading timetable.
The operation¶
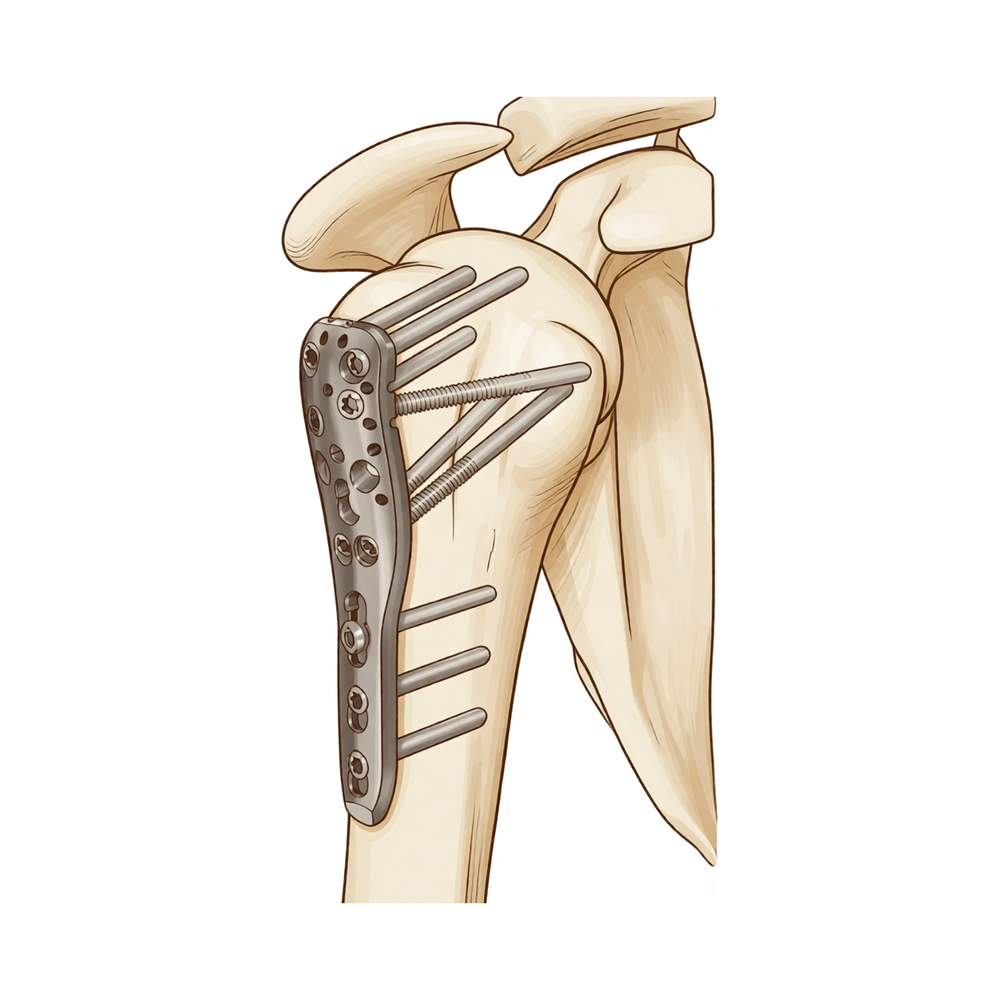
A proximal humerus fracture is a break of the upper end of the arm bone, near the shoulder. In ORIF the fragments are realigned (reduced) and held with a pre-contoured locking plate on the outer surface of the bone, fixed with multiple locking screws into the humeral head. Where the tuberosities (the bony knobs carrying the rotator-cuff attachments) are part of the fracture, they are reduced and secured to the plate, often reinforced with heavy sutures through the cuff. The plate provides immediate mechanical stability; the rehabilitation then protects the biological healing of the fracture and the tuberosity fragments.
Evidence by theme¶
1. Modern locking plates permit early active motion — supported by RCT evidence and adopted here for stable fixation¶
The historical "restrictive" protocol kept the arm immobilised with no active movement for ~6 weeks, with passive limits of flexion to ~90°, external rotation to ~20° and internal rotation to the belly. The rationale for early motion is to prevent the shoulder stiffening (adhesive capsulitis is a recognised complication of these fractures) while still protecting the bone. Because an angular-stable locking plate is mechanically strong from day one, early active elevation can be permitted for stable fixation; the element kept keyed to biological healing is rotation and rotator-cuff loading, because that is what pulls on the tuberosity fragments.
The more aggressive question — can patients move actively from the start? — has now been tested. A prospective randomised controlled trial (Loew et al., J Orthop, 2025) compared a conventional 4-week sling-immobilisation group against an early functional group with no movement or force restrictions after locking-plate ORIF (both groups avoided heavy lifting and impact for 3 months). At 24 months there was no significant difference in DASH or Constant score: Constant score averaged 81.3 (conventional) vs 78.4 (early functional), with relative Constant score 89.8% of the uninjured side in both groups — i.e. early active motion was non-inferior. Moderate (single RCT). This is consistent with the broader signal that early intensive mobilisation yields similar outcomes to conventional later mobilisation after operative treatment. In line with this evidence, Dr Hirpara's protocol now permits early active elevation in a pain-free range for stable fixation; the literature still has no consensus on the optimal regimen, so the one element kept deliberately cautious and keyed to radiographic healing is active/resisted rotation and rotator-cuff loading, because that is the movement that stresses the healing tuberosity fragments.
2. Post-operative protocols are highly heterogeneous, but converge on short immobilisation and early passive ROM¶
The best summary of practice is a systematic review of 45 cohorts (40 articles, 3,507 patients, 3,519 fractures) (Budharaju et al., Shoulder Elbow, 2024). Across studies:
- Sling immobilisation averaged 3.1 weeks (most commonly 3 weeks; range 0–6).
- Passive ROM began at ~0.9 weeks on average (most commonly at 2 days).
- Active ROM began at ~2.5 weeks on average (most commonly at 3 weeks).
- Strengthening began at ~5.5 weeks on average (most commonly at 6 weeks).
The authors emphasised substantial variability regardless of management, concluded that this heterogeneity limits cross-study comparison, and noted that early mobilisation may produce superior function — supporting consideration of shorter immobilisation. The synthesis page's "~3 weeks in the sling, then wean" reflects this averaged convention, not a trial-proven optimum. Moderate for the descriptive pattern; weak/consensus for any specific timetable.
3. Progression is governed by fracture stability and healing, not the calendar — because of the tuberosities and biological complications¶
The locking plate is strong immediately; what limits the rehab is the bone. Two facts anchor the "wait-for-healing" rule:
- Tuberosity / cuff loading. When the tuberosities are part of the fracture, loading the rotator cuff (forced/resisted external rotation and resisted cuff work) too early risks displacing fragments before they unite. This is the explicit reason the early phases keep rotation cautious and defer cuff loading until healing, even though early active elevation in a pain-free range is permitted; where the tuberosities are uninvolved or solidly fixed, the surgeon may clear cuff loading sooner.
- The major complications of locking-plate ORIF are largely biological and mechanical, and several are loading- and reduction-sensitive. A systematic review (Thanasas / Brorson-class series) reports the commonest complications as intra-articular screw perforation (~9–12%), varus collapse (~6.8%), loss of reduction, avascular necrosis of the humeral head (~4.6%, reported range 0–15%), subacromial impingement (~5%), adhesive capsulitis (~4%), nonunion (~1.5%) and deep infection (~1.4%). Screw perforation and avascular necrosis frequently coincide, because a head that collapses or undergoes AVN lets fixed-length locked screws migrate into the joint. Moderate (pooled observational series).
This complication profile is why progression waits on radiographs: premature loading risks tipping a borderline reduction into varus collapse or screw cut-out. Some surgeons even advocate early planned plate removal to avoid secondary screw penetration once the head shows AVN/collapse (Dimitriou et al., J Orthop, 2019) — a salvage strategy, not part of routine rehab, but it illustrates how mechanical and biological failure interact.
4. Who is offered ORIF at all — the operative-versus-non-operative debate (PROFHER and after)¶
The single most influential trial is PROFHER (Rangan et al., JAMA, 2015; 250 patients, 32 UK centres, displaced fractures involving the surgical neck): surgery showed no important difference in Oxford Shoulder Score versus sling-based non-operative care over 2 years, and was more expensive. The 5-year follow-up (Handoll/Keding et al., Bone Joint J, 2017) confirmed no significant difference in shoulder function or quality of life persisting to 5 years. A smaller RCT in displaced 3-part fractures in the elderly (Fjalestad et al., J Shoulder Elbow Surg, 2012) similarly found no functional advantage to internal fixation over non-operative care in that group, and a systematic review and meta-analysis (Beks et al., J Shoulder Elbow Surg, 2018) found no clear superiority of operative treatment across observational and randomised data combined. Strong (multiple RCTs + SR-MA).
The clinical upshot — and the reason this matters to a rehab page — is that ORIF is selectively indicated, typically in younger patients, in fractures where reduction and stable fixation are achievable and worthwhile, and where the alternative (non-operative care or arthroplasty) is judged less favourable. The decision is individualised; "difficulty in decision-making" for displaced fractures is itself documented as affecting outcomes (Okike et al., J Shoulder Elbow Surg, 2018). Patients should understand that being offered ORIF is a considered judgement, not an automatic consequence of the fracture.
5. Adjacent rehabilitation evidence (non-operative immobilisation duration)¶
Although it concerns non-operatively treated fractures, a relevant randomised controlled trial (Tanji et al., J Bone Joint Surg Am, 2021) compared 1 versus 3 weeks of immobilisation and supports the broad theme that earlier movement is at least as good as longer immobilisation for many proximal humerus fractures. It does not directly govern the post-ORIF protocol but reinforces the same direction-of-travel away from prolonged slings. Moderate (RCT, non-operative population).
Phased post-operative timeline (consistent with the synthesis page)¶
| Phase | Window | Sling | Shoulder motion | Strengthening | Governing rule |
|---|---|---|---|---|---|
| I — Protection & early passive motion | Weeks 0–6 | Full-time ~3 weeks, then weaned; off for exercises/hygiene; not in bed | Early active-assisted/active elevation permitted in a pain-free range from the outset (supine-start → upright); passive as needed; pendulums; elbow/wrist/hand active. ER kept to a gentle ~30–40° default; rotation cautious — defer active/resisted cuff work until tuberosities heal (surgeon-guided) | None at the shoulder (deltoid/periscapular isometrics as comfort allows) | Protect fixation + tuberosities; settle pain/swelling |
| II — Regaining active movement | Weeks 6–12 | Discarded by the 6-week review at the latest | Active-assisted → active in all planes (supine-start elevation); submaximal cuff/deltoid isometrics once healing confirmed | Light elbow/scapular work; no resisted cuff work until union (typically not before 8–12 weeks) | Radiographic healing at the ~6-week review gates active motion |
| III — Strengthening | ~Months 3–4½ | Off | Full active ROM in all planes, including behind-the-back | Graded bands → light free weights (~0.5–2 kg) for cuff, deltoid, scapula | Union confirmed; symptom-guided load progression |
| IV — Return to full activity | ~4½–6 months | Off | Full, with dynamic/overhead drills as relevant | Heavier resistance, compound + sport/work-specific | Return-to-task agreed with surgeon/physio, not the calendar |
The phase boundaries are individualised at Dr Hirpara's reviews on the basis of X-ray healing — this is the operative consequence of the "stability- and healing-governed, not calendar-governed" principle.
Key controversies / evidence quality¶
-
Early active versus delayed (protected) mobilisation after ORIF. A single RCT (Loew 2025) found unrestricted early active motion non-inferior to 4-week immobilisation at 24 months, and the broader literature leans toward shorter immobilisation. The protocol here aligns with that early-active-motion evidence: early active and active-assisted elevation in a pain-free range is permitted for stable fixation, rather than holding the shoulder passive-only for six weeks. Because there is still no consensus and no large confirmatory trial (protocols remain heterogeneous — Budharaju 2024), the protocol keeps one deliberate, evidence-aware caution: active/resisted rotation and cuff loading is keyed to radiographic tuberosity healing rather than released wholesale on day one. Moderate evidence, unsettled.
-
Operative versus non-operative treatment of displaced fractures. PROFHER (2015) and its 5-year follow-up (2017), plus an elderly-3-part RCT (Fjalestad 2012) and a meta-analysis (Beks 2018), found no clear functional benefit of surgery on average — which is why ORIF is selectively, not routinely, offered. The trials enrolled broad/older populations; the subgroup most likely to benefit from fixation (younger patients, good bone, reconstructable head-preserving fractures) is exactly where this operation is concentrated. Strong evidence overall; subgroup benefit remains debated.
-
The post-operative rehab protocol itself is consensus/expert. No high-level RCT defines the optimal phase structure, ROM limits or strengthening onset after ORIF. The timings here are drawn from published surgeon protocols and the systematic-review averages, individualised at review. Weak/consensus.
Evidence-strength flags (summary)¶
- STRONG (RCT / SR-MA): operative versus non-operative equivalence on average for displaced fractures (PROFHER 2-yr JAMA 2015 + 5-yr Bone Joint J 2017; Fjalestad 2012 RCT; Beks 2018 SR-MA).
- MODERATE (single RCT / pooled series): early active motion non-inferior to immobilisation after ORIF at 24 months (Loew 2025 RCT); 1-vs-3-week immobilisation non-operatively (Tanji 2021 RCT); locking-plate complication profile — screw perforation, varus collapse, AVN, etc. (pooled observational series); descriptive practice pattern of short sling + early passive ROM (Budharaju 2024 SR of 45 cohorts).
- WEAK / CONSENSUS: the specific phased rehabilitation timetable after ORIF (no defining rehab RCT; published surgeon protocols + systematic-review averages; progression individualised by radiographic healing).
Citations¶
RAG corpus (180,000+ Orthopaedic articles) — real DOIs¶
- Five-year follow-up results of the PROFHER trial comparing operative and non-operative treatment of adults with a displaced fracture of the proximal humerus. Bone Joint J. 2017. DOI: 10.1302/0301-620x.99b3.bjj-2016-1028
- Operative versus nonoperative treatment of proximal humeral fractures: a systematic review, meta-analysis, and comparison of observational studies and randomized controlled trials. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2018.03.009
- Internal fixation versus nonoperative treatment of displaced 3-part proximal humeral fractures in elderly patients: a randomized controlled trial. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2010.12.018
- One Versus 3-Week Immobilization Period for Nonoperatively Treated Proximal Humeral Fractures: a randomized controlled trial. J Bone Joint Surg Am. 2021. DOI: 10.2106/jbjs.20.02137
- Contemporary Management of Proximal Humeral Fractures. J Am Acad Orthop Surg. 2024. DOI: 10.5435/jaaos-d-24-01073
- The Use of Precontoured Humeral Locking Plates in the Management of Displaced Proximal Humerus Fracture. J Am Acad Orthop Surg. 2009. DOI: 10.5435/00124635-200909000-00005
- Use of locking plates in the treatment of proximal humerus fractures. J Shoulder Elbow Surg. 2010. DOI: 10.1016/j.jse.2010.01.001
- Functional results and unfavorable events after treatment of proximal humerus fractures using a new locking plate system. BMC Musculoskelet Disord. 2023. DOI: 10.1186/s12891-023-06176-5
- Fracture site augmentation with calcium phosphate cement reduces screw penetration after open reduction–internal fixation of proximal humeral fractures. J Shoulder Elbow Surg. 2012. DOI: 10.1016/j.jse.2011.09.017
- Difficulty in decision making in the treatment of displaced proximal humerus fractures: the effect of uncertainty on surgical outcomes. J Shoulder Elbow Surg. 2018. DOI: 10.1016/j.jse.2017.09.033
Literature (URLs)¶
- Loew M, et al. Postoperative treatment of proximal humerus fractures with an early active motion protocol: a prospective randomized controlled trial. J Orthop. 2025. https://www.sciencedirect.com/science/article/pii/S1058274625001867 (Constant 81.3 conventional vs 78.4 early-functional at 24 months; early active motion non-inferior)
- Budharaju A, Hones KM, Hao KA, et al. Rehabilitation protocols in proximal humerus fracture management: a systematic review. Shoulder Elbow. 2024;16(4):449–458. https://pmc.ncbi.nlm.nih.gov/articles/PMC11437559/ (45 cohorts; sling 3.1 wk, passive 0.9 wk, active 2.5 wk, strengthening 5.5 wk; early mobilisation may improve function)
- Rangan A, et al. (PROFHER). Surgical vs nonsurgical treatment of adults with displaced fractures of the proximal humerus: the PROFHER randomized clinical trial. JAMA. 2015;313(10):1037–1047. https://pubmed.ncbi.nlm.nih.gov/25756440/ (250 patients; no important difference in Oxford Shoulder Score at 2 years)
- Complications associated with locking plate of proximal humerus fractures (systematic review of complication rates). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC5858203/ (screw perforation ~9–12%, varus collapse ~6.8%, AVN ~4.6%)
- Avascular necrosis and posttraumatic arthritis after proximal humerus fracture internal fixation: evaluation and management. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9889581/ (AVN reported range 0–15%)
- Late screw-related complications in locking plating of proximal humerus fractures: a systematic review. Injury. https://www.sciencedirect.com/science/article/abs/pii/S0020138319306989
- Dimitriou D, et al. Early locking plate removal following ORIF of proximal humeral fractures could prevent secondary implant-related complications. J Orthop. 2019;17:106–109. https://pmc.ncbi.nlm.nih.gov/articles/PMC6919395/
Published rehabilitation protocols (patient-guidance — basis for the phase structure)¶
- Massachusetts General Brigham Sports Medicine. Rehabilitation Protocol for Proximal Humeral Fracture Open Reduction Internal Fixation (ORIF). https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-proximal-humeral-fracture-with-ORIF.pdf
- LaPrade CM. Post-Surgical Physical Therapy Protocol: Proximal Humerus Fracture ORIF. Twin Cities Orthopedics. https://tcomn.com/wp-content/uploads/2024/08/CML_Proximal-Humerus-ORIF-PT_10-2024.pdf
- Coyner KJ. ORIF Proximal Humerus Fractures Protocol. UConn Musculoskeletal Institute. https://www.drcoyner.com/pdf/orif-proximal-humerus-fractures-protocol.pdf
- Jazrawi LM. Rehabilitation Protocol: Proximal Humerus Open Reduction & Internal Fixation (ORIF). NYU Langone Orthopedic Center. https://www.newyorkortho.com/pdf/proximal-humerus-fracture-orif-post-op-instructions-and-rehab.pdf
- South Bend Orthopaedics. ORIF Proximal Humerus Fracture Rehab Protocol. https://www.sbortho.com/wp-content/uploads/2023/09/br-pt-fracture-orif-proximal-humerus.pdf