Patients › Rehabilitation
Pagpapalit ng PIP Joint
Isang protektadong plano ng paggaling pagkatapos ng pagpapalit ng silicone sa nasirang gitnang kasukasuan ng daliri (PIP joint), kung saan ang bilis ng pagsisimula ng paggalaw ay nakadepende sa kung ang doktor ay pumasok mula sa harap (palma) o likod ng daliri.
Ang protokol na ito ay gabay sa iyong paggaling pagkatapos ng pagpapalit sa nasirang gitnang kasukasuan ng daliri (ang proximal interphalangeal (PIP) joint, ang gitnang knuckle) gamit ang flexible silicone spacer, na isinagawa ni Dr Kieran Hirpara sa Mater Private Hospital Rockhampton. Nagsisimula ito sa iyong home exercise program, sinundan ng istrukturadong klinikal na protokol na isinulat para sa iyong hand therapist. Dalhin ang pahinang ito o ang PDF nito sa iyong unang bisita sa therapy upang manatiling koordinado ang iyong rehabilitasyon. Maaaring baguhin ng iyong therapist ang plano depende sa kung paano ang pag-unlad ng iyong paggaling.
Kung mayroon kang anumang alalahanin tungkol sa iyong sugat pagkatapos ng operasyon, makipag-ugnayan sa mga kwarto. Karaniwang makakatulong kukuha ng litrato ng sugat at ipadala ito sa pamamagitan ng email para sa pagsusuri.
Ano ang inaasahan¶
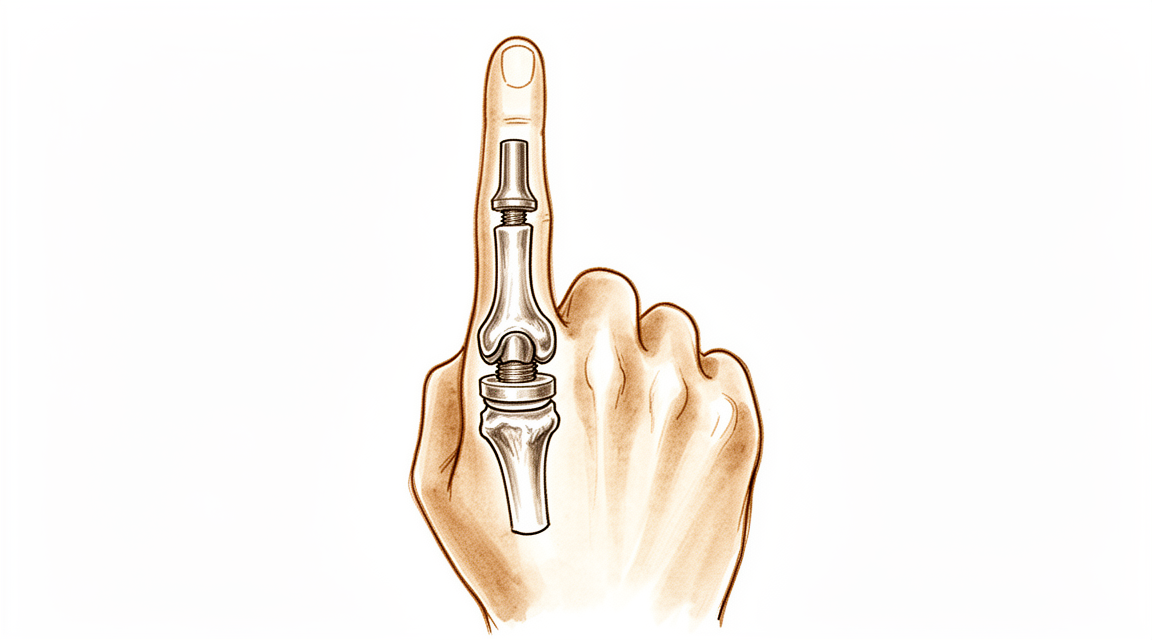
Ang gitnang kasukasuan ng iyong daliri ay nagsuot na dahil sa arthritis, na nakakaaliw at nakakapagod. Sa operasyong ito, tinatanggal ang mga nasirang ibabaw ng kasukasuan at isang flexible silicone spacer (isang implantong uri ng Swanson) ang ilalagay sa pagitan ng dalawang buto. Ang spacer ay hindi isang rigid mechanical hinge; ito ay isang bendy spacer na nagpapanatili ng distansya sa pagitan ng mga buto, pinapayagan ang pagliko ng daliri, at pinapayagan ang iyong sariling scar tissue na bumuo ng bagong supportive sleeve sa paligid nito. Ang pangunahing at pinakamalapit na benepisyo ay pain relief. Inaasahan mo rin ang isang makabuluhang, modest na arc ng pagliko (karaniwang nasa 40 hanggang 60 degrees) imbes na isang buo at normal na range. Karamihan sa mga tao ay napakasaya dahil nawala ang sakit at komportable ang paggamit ng daliri.
Ang pinakamahalagang bagay sa iyong paggaling ay kung saan pumasok ang surgeon, dahil iyon ang nagdidikta kung kailan ka makakapag-move:
- Mula sa harap (ang palm side, isang volar approach): ang straightening tendon sa likod ng daliri ay naiiwan na buo. Dahil walang kailangang mag-heal sa likod, karaniwang maaari kang magsimulang gumalaw ng daliri sa loob ng ilang araw.
- Mula sa likod (isang dorsal approach): ang straightening tendon (ang central slip) ay kailangang hiwain o itaas upang maabot ang kasukasuan, pagkatapos ay ayusin. Ang repair na ito ay kailangang protektahan muna, kaya ang daliri ay isplinted na tuwid sa maagang yugto at ang pagliko ay ipinakilala nang mas dahan-dahan, sa ilalim ng gabay ng iyong hand therapist.
Ang iyong hand therapist ang sumusunod sa plano para sa iyong surgical approach. Ipapaliwanag ni Dr. Hirpara sa kanila kung anong approach ang ginamit, at ang mga timing sa ibaba ay tailored dito. Anuman ang approach na ginawa mo, ang bagong kasukasuan ay isang hinge: gusto nito ang pagliko at pagtuwid sa isang tuwid na linya, ngunit hindi nito gusto ang pagtulak o pag-ikot sa gilid. Ang pagprotekta nito mula sa side-to-side stress ang nagpapanatili ng kanyang katatagan para sa pangmatagalan.
Mga Paalala at Limitasyon¶
- Galawin ang daliri lamang sa tuwid na linya (pagtukol at pagwawasto) at iwasan ang anumang pwersa sa gilid o pag-ikot sa operadong daliri. Ang bagong kasukasuan ay isang bisagra, at ang stress sa gilid ay maaaring paluwagin o deforme ito.
- Suotin ang iyong splint ayon sa utos, at gumamit ng buddy strapping habang nag-e-ehersisyo upang manatiling tuwid ang paggalaw ng daliri.
- Kung ang iyong operasyon ay mula sa likod ng daliri, huwag IPUKO ang iyong sariling pagwawasto laban sa limitasyong ibinigay sa simula: ang tendon ng pagwawasto ay nagpapagaling.
- HUWAG gumawa ng matibay na pagkapit, mahigpit na pagpipit, o mabibigat o nakakaiting gawain hanggang sa ma-clear ka ng iyong hand therapist para sa pagpapalakas (karaniwan mula sa anim na linggo).
- Panatilihin ang paggalaw ng ibang kasukasuan ng daliri, ng iyong pulso, at ng iyong balikat mula sa simula, at gamitin ang kamay para sa magaan na pang-araw-araw na gawain hangga't komportable.
Para sa pag-aalaga sa sugat, pamamahala ng pamamaga, at peklat, tingnan ang gabay ng klinika tungkol sa pag-aalaga sa sugat.
Mga ehersisyo ninyo¶
Ito ang mga ehersisyo mula sa inyong handout. Simulan lamang ito ayon sa gabay ni Dr. Hirpara at ng inyong hand therapist, at manatili sa loob ng anumang saklaw at limitasyon na ibinigay sa inyo. Ang maagang gawain ay pinapanatiling gumagalaw ang daliri sa tuwid na linya nang walang stress sa gilid: protektadong pagbaluktot, banayad na pagwawasto, buddy strapping, at tendon glides. Kung ang inyong operasyon ay mula sa likod ng daliri, ang ehersisyong aktibong pagwawasto ang dapat protektahan sa maagang yugto at dahan-dahang palakihin. Ang pagpapalakas ng hawak (grip strengthening) ay kabilang sa mas huling yugto at hindi dapat simulan hangga’t hindi pa ito espesipikong pinapayagan. Itigil ang anumang nagdudulot ng matulis na sakit o nagpaparamdam ng kawalan ng katatagan sa daliri.
Ang iyong klinikal na protokol¶
Ang natitirang bahagi ng pahinang ito ay ang yugto-yugto na klinikal na protokol para sa rehabilitasyon pagkatapos ng arthroplasty ng PIP joint na may silicone. Ang seksyong ito ay dapat ibigay sa iyong hand therapist, at ang bawat yugto ay nagsisimula sa isang paliwanag sa simpleng wikang Ingles tungkol sa nangyayari. Ang protokol ay nakadepende sa approach, at ito ang pangunahing central branch point: ang volar (palmar) approach ay nag-iwan ng extensor mechanism na intact at nagpapahintulot sa maagang aktibong galaw sa loob ng ilang araw; ang dorsal approach ay naghihiwalay o naghihati sa central slip, kaya ang paggaling ng extensor ay dapat protektahan muna gamit ang extension orthotics at graded flexion. Sa buong proseso, ang silicone implant ay isang flexible spacer na ang long-term stability ay nakadepende sa peri-implant capsule, kaya iwasan ang coronal (lateral) stress at panatilihin ang galaw sa isang purong sagittal arc.
Bago ang paggamot, kumpirmahin sa treating surgeon ang surgical approach (volar vs dorsal), ang integridad/repair ng central slip at collateral ligaments, at anumang intra-operative arc. Itatakda ni Dr Hirpara ang approach; piliin ang volar (early-active-motion) o dorsal (extension-protected) pathway ayon sa kinakailangan. Ang inaasahang functional target ay isang pain-free arc na humigit-kumulang 40–60°, hindi buong range.
Yugto I — protektahan at simulan ang galaw (linggo 0 hanggang 3)¶
Ang unang mga linggo ay nagpoprotekta sa malambot na tisyu habang pinipigilan ang pagkakasikip, na may bilis na itinakda nang buo ng paraan ng operasyon. Matatag ang implant sa flexion–extension ngunit vulnerable sa side load, kaya ang lahat ng galaw ay pinapanatili sa isang malinis na sagittal plane at sinusuportahan ang daliri gamit ang buddy strapping at splint.
Para sa iyong hand therapist:
Edukasyon at mga paalala - Tukuyin ang surgical approach at sundin ang katumbas na landas: - Volar approach: intact ang extensor mechanism → simulan ang active PIP/DIP motion sa 3–5 araw. Mag-fit ng volar extension-block / template splint na nagpapahintulot sa isang maikling flexion arc (karaniwang ~30° sa simula), na dahan-dahang pinapalawak. - Dorsal approach (central slip split/repaired): protektahan ang extension. PIP splinted malapit sa full extension buong oras; ipakilala ang active flexion sa isang limitadong maikling arc sa ilalim ng supervisyon, na pinapahalagahan ang repair ng central-slip. (Maaaring gamitin ang relative-motion / dynamic-extension scheme ayon sa kagustuhan ng surgeon.) - Mahigpit na pag-iwas sa coronal (lateral/radial–ulnar) stress sa operated joint: buddy strap sa katabing digit upang gabayan ang purong sagittal tracking. - Walang paghawak, pagpipit o resisted/loaded na paggamit.
Pamamahala - Sugat: surgical dressings ayon sa utos; monitor para sa impeksyon - Oedema: elevation, banayad na retrograde massage, magaan na compressive wrap - Mga ehersisyo: protektadong active PIP/DIP flexion–extension sa loob ng itinakdang arc; tendon glides; active motion ng hindi apektadong joints (DIP, MCP, wrist, thumb); simulan ang buddy strapping para sa aktibidad - Splint na suot buong oras sa pagitan ng mga session ng ehersisyo
Mga pamantayan para mag-progress - Maayos ang paggaling ng sugat; walang extensor lag na umuusbong (dorsal pathway); komportable, kontroladong galaw sa loob ng kasalukuyang arc
Yugto II — pagpapahusay ng galaw (linggo 3 hanggang 6)¶
Buksan ang arc ng flexion, at para sa mga daliri na may dorsal na daan, unti-unting bawasan ang proteksyon sa extension habang nagkukonsolida ang central slip. Layunin ng panahong ito na makabuo ng kapaki-pakinabang na arc (≈40–60°) bago mahigpit na itakda ng pagtanda ng sikat ang saklaw ng galaw.
Para sa iyong hand therapist:
Mga Pagsusuri - Aktibo at pasibong arc ng PIP; extensor lag (dorsal na daan); koronal na katatagan; sakit at edema; pagsusuri sa sugat/sikat
Edukasyon at mga paalala - Unti-unting palakasin ang pinapayalang arc ng flexion patungo sa functional na target (≈40–60°) - Volar: ituloy ang pag-unlad ng aktibong flexion ayon sa kakayahang tanggapin; magdagdag ng banayad na pasibong flexion kung buo at matatag ang extension - Dorsal: bawasan ang splinting ng extension ayon sa paggaling ng central-slip (karaniwang binabawasan ang suporta sa araw sa mga linggo 4–6); mag-ingat laban sa extensor lag: huwag hanapin ang flexion sa presyo ng aktibong extension - Patuloy na mahigpit na iwasan ang lateral/torsional na load; walang resisted strengthening pa
Pamamahala - Mga ehersisyo: grasyadong aktibo at aktibo-assisted na PIP flexion–extension; blocking exercises upang pokusin ang galaw ng PIP; patuloy na tendon glides at buddy strapping; simulan ang scar massage kapag gumaling na ang sugat - Panatilihin ang buong galaw ng mga katabing joints
Mga pamantayan para magpatuloy - Gumaling na sugat; matatag na joint sa koronal na plano; itinatag na functional na pain-free arc; minimal na extensor lag (dorsal)
Yugto III — palakasin at ibalik (linggo 6 hanggang 12 at higit pa)¶
Kapag nakapagkaroon na ng galaw at malusog na ang mga malambot na tisyu (humigit-kumulang anim na linggo), magsisimula ang magaan na pagpapalakas at unti-unting dadagdagan. Panatilihin ang axial na pagpapalakas (hila at tuwid na pagkarga) habang patuloy na pinapansin ang lateral/torsional na stress sa implant sa pangmatagalan.
Para sa iyong hand therapist:
Pagsusuri - Hila at pinch kumpara sa kabilang panig; huling arc ng PIP; koronal na katatagan; functional at task-specific na pagsubok
Edukasyon at mga paalala - Magsimula ng magaan na pagpapalakas ng hila mula sa humigit-kumulang anim na linggo, unti-unting pagdagdagan - Ipakilala ang pinch loading nang maingat at patuloy na iwasan ang makapangyarihang lateral/pag-ikot na pagkarga sa operated na kasukasuan sa walang katapusan (tagal-buhay ng implant) - Magtakda ng realistikal na inaasahan: ang matibay na pagpapagaan ng sakit ang pangunahing benepisyo; ang huling arc ay katamtaman (≈40–60°) at karamihan ay nakatakda na sa ~3 buwan
Pamamahala - Mga ehersisyo: progressive na hila/gamit ang putty; graded na functional at work-specific na pagkarga; patuloy na anumang natitirang mobility at trabaho sa peklat - Isalang-alang ang discharge kapag nakamit na ang matatag, komportableng, functional na daliri na may kapaki-pakinabang na pain-free na arc - Mag-refer pabalik sa naggamot na doktor kung huminto ang paggaling, maging unstable/nagde-deviate ang kasukasuan, o magkaroon ng pagdududa sa failure ng implant
Mga pamantayan para sa discharge / pagbabalik - Komportableng, walang sakit, koronal na matatag na kasukasuan na may functional na arc; sapat na hila; kayang tugunan ang mga pang-araw-araw at trabaho na pangangailangan
Pagbabalik sa trabaho at gawain¶
Ang magaan na paggamit ng kamay sa pang-araw-araw (pagkain, pagsulat, magaan na pag-aalaga sa sarili) ay inirerekomenda mula sa simula, hangga't komportable ito, at habang ito ay nasa tuwid na linya at iwasan ang puwersa mula sa gilid patungo sa gilid o pag-ikot sa operadong daliri. Karaniwang maaaring magmaneho kapag kumportable ka na hawakan ang manibela at kontrolado ang sasakyan nang ligtas, wala ka na sa anumang mahigpit na splint, at hindi ka na kumukuha ng malakas na gamot sa sakit, na karaniwang ilang linggo, at kumpirmado sa iyong pagsusuri.
Ang mas matibay na pagkupot at mga gawain na may kargahan ay inaasahan hanggang sa humigit-kumulang anim na linggo, at dahan-dahang binubuo. Ang mas mabigat na manual o pag-ikot na trabaho ang huli na babalik, at batay sa pagbawi ng komportableng, matatag na daliri na may sapat na pagkupot, pinahahalagahan ni Dr. Hirpara at ng iyong hand therapist, hindi lamang base sa kalendaryo. Tandaan ang pangmatagalang kasunduan sa operasyong ito: maaasahan ang pagpapagaan ng sakit at isang kapaki-pakinabang na arkong humigit-kumulang 40 hanggang 60 degrees, na may pag-iwas sa puwersa mula sa gilid patungo sa gilid sa kasukasuan sa pangmatagalan upang protektahan ang implant.
Pagkatapos ng iyong protocol¶
Ang protocol na ito ay kasabay ng pangkalahatang payo para sa paggaling ng klinika; tingnan ang pamamahala ng post-operative na sakit, pag-aalaga sa sugat, at pamamahala ng peklat. Ang nakalarawang phased na plano ay sumasalamin sa publikadong gabay sa rehabilitasyon pagkatapos ng silicone PIP joint arthroplasty, at ang iyong patuloy na paggaling ay indibidwal na pinamumunuan ni Dr. Hirpara at ng iyong hand therapist ayon sa ginamit na surgical approach at kung paano ang pag-unlad ng iyong daliri.
Evidence & references
Silicone PIP Joint Replacement — Procedure Outcomes & Post-operative Rehabilitation (Swanson-type Arthroplasty for PIP Osteoarthritis)¶
Topic scope: post-operative rehabilitation after silicone (Swanson-type) proximal interphalangeal (PIP) joint arthroplasty for primary osteoarthritis. The worn joint surfaces are excised and a flexible silicone spacer is implanted; this is an interposition / encapsulation arthroplasty, not a rigidly-fixed mechanical hinge. The implant works as a flexible spacer around which a peri-implant fibrous capsule forms to provide stability. The dominant, reliable benefit is pain relief; the functional gain is a modest active arc (~40–60°), not restoration of normal range.
Defining principle of the rehab here: the rehabilitation pathway is dictated by the surgical approach, because the rate-limiting tissue is the extensor mechanism, not the implant. A volar (palmar) approach leaves the central slip and extensor mechanism intact → it permits immediate / early active motion (within 3–5 days). A dorsal approach must split or reflect the central slip to reach the joint → the extensor repair must be protected first with extension orthotics and a graded, short-arc flexion programme. Across both pathways the silicone spacer is stable in the sagittal (flexion–extension) plane but vulnerable in the coronal plane, so the programme deliberately avoids lateral / torsional load and tracks the joint in a pure sagittal arc (buddy strapping). Therapy aims to bank the useful arc before scar maturation fixes it while protecting extension and the implant — it is not an immobilise-to-heal construct in the volar case.
A. PROCEDURE OUTCOMES (silicone PIP arthroplasty for osteoarthritis)¶
Silicone PIP arthroplasty is a reliable pain-relieving operation with predictable but modest motion; the principal debates are over surgical approach and implant choice (silicone vs surface-replacement/pyrocarbon), not whether arthroplasty relieves pain.
- Pain relief is high and durable; motion gains are modest. A long-term series of Swanson silicone PIP arthroplasty for osteoarthritis (mean ~10-year follow-up) reported excellent pain relief (mean VAS ~0.4) with essentially unchanged arc (≈55° pre-op → ≈50° post-op) and high patient satisfaction — patients would have the surgery again despite limited motion gain [Bales, Wall & Stern, J Hand Surg Am 2014]. Moderate (level-IV long-term cohort).
- The volar approach can improve the active arc. A volar-approach silicone PIP series reported the active arc improving from ~33° to ~72°, with good function and satisfaction, by preserving the extensor mechanism and enabling early motion [Proubasta et al., J Hand Surg Am 2014]. Moderate–weak (level-IV).
- Radiographic implant deformation/fracture is common but poorly correlated with symptoms. In the long-term Swanson series most implants deformed and many fractured radiographically, yet clinical revision was uncommon (survivorship ~90% at ~10 years) and there was no correlation between radiographs and satisfaction [Bales, Wall & Stern 2014]. Strong natural-history signal within a cohort.
- Silicone vs surface-replacement and pyrocarbon implants give broadly comparable clinical results; no implant is clearly superior. Systematic review across implants/approaches found comparable outcomes with implant-/approach-specific complication profiles [Yamamoto et al., Plast Reconstr Surg 2017; Carlson Strother, Moran & Rizzo, JAAOS 2023]. Moderate (SR + narrative review).
- Pyrocarbon and resurfacing implants carry their own failure modes (subsidence, squeaking, intra-operative periprosthetic fracture, instability), informing implant choice rather than rehab [Watts et al., J Hand Surg Am 2012; Wagner et al. medium-term 2018 & intra-op fractures 2015; Branam et al. resurfacing-vs-silicone 2007]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE¶
The central rehab questions are (1) how soon to move and (2) how to splint, and the answer to both is set by the surgical approach and the extensor mechanism. The evidence base is low-level (expert consensus / single-cohort therapy series) — there are no RCTs comparing PIP arthroplasty rehab pathways.
- Approach dictates the timeline (the core principle). Surgical reviews establish that a volar approach preserves the central slip and permits immediate active and passive motion, while a dorsal approach requires post-operative protection of the split/repaired central slip before flexion is advanced [Renfree, Bone Joint J 2022 (surgical approaches); Herren, Hand Clin 2017; Yamamoto et al. 2017]. Moderate (surgical evidence) — strong mechanistic basis.
- A structured 12-week, splint-based therapy programme is the consensus framework (dorsal pathway). Feldscher's hand-therapy protocol for PIP (pyrocarbon, central-slip-splitting dorsal approach) uses a volar static finger orthosis allowing a limited short-arc PIP/DIP active arc that is increased over the rehab course, with a hand-based resting splint (MCP flexed, PIP/DIP near 0°) for full-time use except during template-splint exercise [Feldscher, J Hand Ther 2010]. Weak (expert-consensus protocol).
- A defined controlled-motion program exists and reports good arcs. A controlled-motion rehabilitation program for PIP arthroplasty reported favourable range-of-motion outcomes, supporting graded controlled motion over rigid immobilisation [Ramanathan, Koludrovich & Evans, J Hand Ther 2021]. Weak (cohort / programme description).
- Static and dynamic extension splinting give similar results. A comparison of static vs dynamic splinting after PIP pyrocarbon arthroplasty found comparable outcomes, favouring static splinting for simplicity and patient convenience [Jennings & Livingstone / static-vs-dynamic cohort, J Hand Ther 2011]. Weak–moderate (comparative cohort).
- Coronal-plane protection is the durable, lifelong caveat. Collateral integrity and avoidance of lateral stress underpin long-term implant stability; collateral compromise drives instability/deviation [Carlo et al., collateral reconstruction, J Hand Surg Am 2016; Carlson Strother et al. 2023]. Consensus / mechanistic.
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint (by approach) | Hand-therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect & initiate motion | Week 0–3 | Volar: active motion at 3–5 days, short flexion arc (~30°) in template/extension-block splint. Dorsal: PIP splinted near extension full-time; supervised short-arc flexion only | Protected sagittal PIP/DIP motion; tendon glides; buddy strapping; uninvolved-joint motion; no lateral/torsional load | None (no grip/pinch) | Implant stable in flexion–extension, vulnerable coronally |
| II — Advance motion | Week 3–6 | Progressively increase flexion arc toward ~40–60°. Dorsal: wean extension splint as central slip consolidates (≈wk 4–6); guard against extensor lag | Graded active/AAROM flexion–extension; blocking; scar massage once healed; continue buddy strapping | Still no resisted strengthening | Bank the useful arc before scar maturation fixes it |
| III — Strengthen & return | Week 6–12+ | Lifting/grip restrictions progressively lifted; lateral/twisting load avoided indefinitely | Light grip → cautious pinch; functional & work-specific loading | Grip from ~6 wk, graded | Pain relief is the durable gain; final arc (~40–60°) largely set by ~3 months |
(Phase windows mirror the precautions in the patient protocol; they are typical guides — not trial-derived deadlines — and the volar vs dorsal split is the dominant variable.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Volar vs dorsal approach (the rehab-defining question). The volar approach spares the extensor mechanism and permits early active motion (and a better reported arc), at the cost of being more technically demanding; the dorsal approach is more familiar but mandates extensor protection and a slower, splint-led flexion programme. Choice is surgeon-dependent and drives the entire rehab pathway. Moderate surgical evidence; no head-to-head rehab RCT.
- Implant choice (silicone vs surface-replacement vs pyrocarbon). No implant is clearly superior on clinical outcomes; silicone is durable for pain relief with high radiographic deformation/fracture that poorly predicts symptoms, while pyrocarbon/resurfacing trade different complication profiles (subsidence, instability, intra-operative fracture). Moderate (SR + cohorts).
- Static vs dynamic splinting (dorsal pathway). Comparable outcomes; static splinting is favoured for simplicity and convenience. Weak–moderate.
- Motion gain is modest and that is expected, not failure. Patients reliably lose pain but gain little arc (especially via dorsal/silicone); mislabelling the modest arc as a poor result misframes a successful pain-relieving operation. Counsel the ~40–60° expectation up front. Strong natural-history signal.
- Lifelong coronal-stress avoidance. Long-term stability depends on the peri-implant capsule and collaterals; forceful lateral/twisting load risks deviation, instability and implant failure. Consensus.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (mechanistic / natural-history): the surgical-approach principle (volar preserves extensor mechanism → early motion; dorsal splits central slip → protect extension first); the modest-arc / reliable-pain-relief outcome pattern; radiographic implant deformation poorly predicting symptoms.
- MODERATE: procedure outcomes are level-IV case series (long-term Swanson silicone series; volar approach series); implant-comparison systematic review/narrative review; surgical-approach reviews.
- WEAK / EXPERT CONSENSUS: the specific rehabilitation regimen — short-arc controlled motion, 12-week splint-based programme, static-vs-dynamic splinting equivalence, exact phase timings. These are low-level, expert-consensus / single-cohort therapy descriptions, not trial-derived; individualise to the operative approach and tissue quality.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2013.11.008
- Proubasta IR, Lamas CG, Natera L, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014;39(6). DOI: 10.1016/j.jhsa.2014.03.033
- Weistra K, Kan HJ, van Alebeek VAHJ, et al. Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex in 72 cases. HAND. 2022. DOI: 10.1177/15589447221122829
- Branam BR, Tuttle HG, Stern PJ, et al. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007. DOI: 10.1016/j.jhsa.2007.04.006
- Yamamoto M, Malay S, Fujihara Y, et al. A systematic review of different implants and approaches for proximal interphalangeal joint arthroplasty. Plast Reconstr Surg. 2017. DOI: 10.1097/prs.0000000000003260
- Renfree KJ. Surgical approaches for proximal interphalangeal joint arthroplasty. Bone Joint J. 2022;104-B(12). DOI: 10.1302/0301-620x.104b12.bjj-2022-0946
- Herren DB. Current European practice in the treatment of proximal interphalangeal joint arthritis. Hand Clin. 2017. DOI: 10.1016/j.hcl.2017.04.002
- Carlson Strother CR, Moran SL, Rizzo M. Small joint arthroplasty of the hand: an update on indications, outcomes, and complications. J Am Acad Orthop Surg. 2023;31(15). DOI: 10.5435/jaaos-d-23-00034
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. DOI: 10.1016/j.jht.2009.10.011
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. DOI: 10.1016/j.jht.2019.04.003
- Watts AC, Hearnden AJ, Trail IA, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: minimum two-year follow-up. J Hand Surg Am. 2012. DOI: 10.1016/j.jhsa.2012.02.012
- Wagner ER, Weston JT, Houdek MT, et al. Medium-term outcomes with pyrocarbon proximal interphalangeal arthroplasty: a study of 170 consecutive arthroplasties. J Hand Surg Am. 2018. DOI: 10.1016/j.jhsa.2018.06.020
- Wagner ER, Van Demark R, Kor DJ, et al. Intraoperative periprosthetic fractures in proximal interphalangeal joint arthroplasty. J Hand Surg Am. 2015. DOI: 10.1016/j.jhsa.2015.06.101
- McGuire DT, White CD, Carter SL, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: outcomes of a cohort study. J Hand Surg Eur Vol. 2011;37(6). DOI: 10.1177/1753193411434053
- Carlo J, Dell PC, Matthias R, et al. Collateral ligament reconstruction of the proximal interphalangeal joint. J Hand Surg Am. 2016;41(1). DOI: 10.1016/j.jhsa.2015.10.007
- Aversano FJ, Calfee RP. Salvaging a failed proximal interphalangeal joint implant. Hand Clin. 2018. DOI: 10.1016/j.hcl.2017.12.011
PIP arthroplasty rehabilitation literature (URLs)¶
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. https://pubmed.ncbi.nlm.nih.gov/20036511/
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/31481342/
- Static versus dynamic splinting for proximal interphalangeal joint pyrocarbon implant arthroplasty: a comparison of current and historical cohorts. J Hand Ther. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143198/
- Proubasta IR, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24799141/
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for PIP joint osteoarthritis. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24559624/
- The dorsal approach to silicone implant arthroplasty of the proximal interphalangeal joint. J Hand Surg Am. 2007. https://www.sciencedirect.com/science/article/abs/pii/S0363502307004662
- Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex. HAND. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC10953532/