Patients › Shoulder
Osteoarthritis ng AC Joint
AC joint osteoarthritis causes localized shoulder pain with cross-body movements; treatment ranges from activity modification to surgery.
Ano ang nararamdaman mo¶
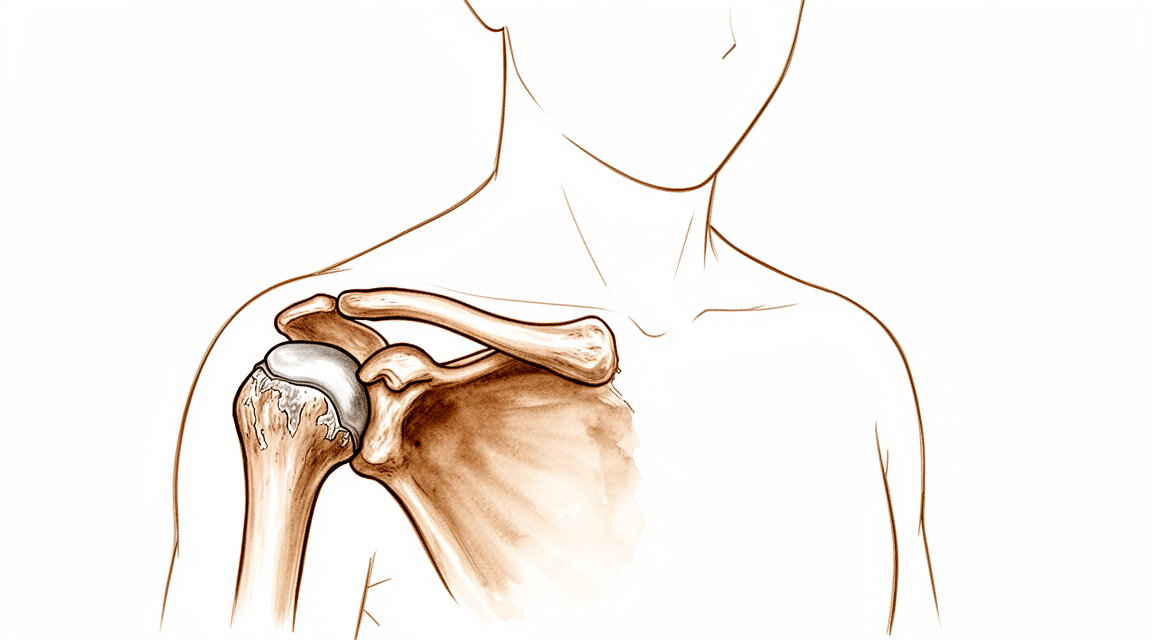
Maaaring mararamdaman mo ang sakit sa pinakatuktok ng iyong balikat, kung saan nagtatagpo ang iyong collarbone at shoulder blade. Ito ang iyong acromioclavicular joint. Maaaring manatiling mahina ang sakit sa loob ng mga taon. Sa katunayan, 90% ng mga tao na may maagang palatandaan sa X-ray ay walang nararamdamang sakit sa loob ng 7 na taon. Gayunpaman, kung magsisimula ang mga sintomas, madalas itong sumusunod sa isang maikling pattern.
Karaniwang lumalala ang sakit kapag gumagalaw ka ng iyong braso patungo sa katawan. Maaari mong maranasan ito kapag umaabot ka sa mataas na shelf o sa likod ng iyong likod upang i-fasten ang bra. Ang pagtutukoy ng isang damit ay maaari ring mag-trigger ng matulis na pinching. Ang pag-angat ng mga bagay, lalo na sa itaas, ay naglalagay ng direktang presyon sa joint na ito. Maraming pasyente ang nakakakita na ang pagpahinga ng braso sa kanilang gilid ay nagdadala ng ginhawa. Ang banayad na galaw ay madalas na mas maganda kaysa sa pagkakatayo nang buong katahimikan.
Ang sakit sa gabi ay isang karaniwang reklamo. Maaari kang magising kung ikaw ay mag-rol sa iyong apektadong balikat. Ang bigat ng iyong katawan ay pumipindot sa inflamed na joint, na nagiging sanhi ng hirap na makahanap ng komportableng posisyon. May ilang tao ang nakakakita na ang sakit ay mas malala kapag sila ay unang gumising sa umaga. Maaaring magkaroon ng stiffness hangga't hindi pa nila galawin ang kanilang katawan sa loob ng ilang oras.
Mahalagang malaman na ang mga findings ng imaging ay hindi laging tumutugma sa iyong mga sintomas. Ang pagkakaiba-iba sa pagitan ng symptomatic at asymptomatic radiographic AC osteoarthritis ay hindi kinakailangan. Lahat ng mga pasyente ay pantay-pantay na nasisiyahan sa resulta ng preoperative acromioclavicular injection, anuman ang ipinakita ng X-ray. Ibig sabihin, ang antas ng iyong discomfort ang tunay na gabay para sa paggamot, hindi lamang ang anyo ng joint sa isang scan.
Kung ikaw ay may nakaraang shoulder surgery, tulad ng rotator cuff repair, ang hindi naaayos na arthritis sa joint na ito ay nauugnay sa mababang percentage ng failure. Ito ay bihira na magdulot ng malalaking problema sa sarili nito. Gayunpaman, kung ikaw ay mayroong persistent na sakit na nakakaapekto sa mga araw-araw na gawain tulad ng pagdadaos o pagtulog, ang iyong surgeon ay maaaring pag-usapan ang mga opsyon tulad ng injection o maliit na surgery upang alisin ang worn na bone ends. Ang mga prosedurong ito ay nagbibigay ng predictable na pain relief para sa symptomatic cases.
Ano ang nangyayari talaga¶
Ang iyong acromioclavicular (AC) joint ay matatagpuan sa pinakatuktok ng iyong balikat, kung saan nagtatagpo ang iyong collarbone at shoulder blade. Isipin ang joint na ito bilang isang maliit na bisagra na nagbibigay-daan sa malinis na paggalaw ng iyong braso pataas. Sa loob nito, ang makinis na cartilage ay gumagana bilang shock absorber, na nagbibigay ng cushion sa mga buto upang hindi sila magkagrasa sa isa’t isa.
Sa AC osteoarthritis, unti-unti nang nasusira ang protektibong cartilage na ito sa paglipas ng panahon. Ito ay sa katunayan ay wear-and-tear arthritis. Habang pinapapalabo ang cushion, mas direktang nagkakaharap at nagkagrasa ang mga buto. Ang friction na ito ay nagdudulot ng pamamaga at sakit, lalo na kapag umabot ka sa ibang gilid ng katawan o itinaas ang iyong braso pataas. Maaari ring maging matigas o mapang-irita ang joint capsule, na ang mangangahulugan ay ang sleeve na nakapalibot sa joint, na nagdaragdag sa hindi komportableng pakiramdam.
Minsan, ang mga ligament na nagtutulak sa collarbone ay napapahaba o naputol. Maaari nitong sanayin ang pagtaas ng collarbone sa higit pa sa normal na posisyon, na lumilikha ng kitang-kita na bulto. Kapag nangyari ito, nagbabago ang normal na paggalaw ng iyong shoulder blade. Ang mga pagbabagong kinematic na ito ay maaaring maging pinagmumulan ng sakit at disfunkshon sa balikat. Kahit mukhang maayos ang joint sa X-ray, maaari pa ring magdulot ng mga sintomas ang altered movement.
Mahalagang malaman na hindi lahat ng pagbabago sa X-ray ay nangangahulugan na magkakaroon ka ng sakit. Ang asymptomatic AC osteoarthritis ay nanatiling asymptomatic sa 90% ng mga pasyente sa loob ng 7 taon. Ibig sabihin, maraming tao ang may kitang-kita na pagkasira sa mga scan ngunit walang nararamdamang sakit sa lahat. Ang hindi naaangkop na osteoarthritis ng AC joint, anuman ang symptomatic o hindi, na nakaharap sa arthroscopic rotator cuff repair ay may kaugnayan sa mababang percentage ng pagkabigo.
Gayunpaman, kung maging severe ang arthritis, maaari itong magdulot ng ibang mga isyu. Ang severe acromioclavicular joint osteoarthritis ay may kaugnayan sa acromial stress fractures pagkatapos ng reverse shoulder arthroplasty. Titingnan ng iyong surgeon ang iyong mga sintomas at imaging upang desisyunin kung ang joint ang tunay na pinagmumulan ng iyong sakit.
Ang layunin ng paggamot ay bawasan ang friction na ito at ibalik ang malinis na paggalaw. Parehong ang open at arthroscopic resection arthroplasty techniques ay nagbibigay ng predictable na pagpapagaan ng sakit para sa symptomatic AC osteoarthritis. Ang mga prosedurong ito ay kasama ang pag-alis ng isang maliit na bahagi ng collarbone upang lumikha ng mas maraming espasyo, na nagpapahintulot sa mga buto na mag-slide nang hindi nagkagrasa. Ang simpleng pagbabagong ito ay maaaring makabuluhang mapabuti ang iyong function ng balikat at bawasan ang sakit.
Mga maitutulong namin dito¶
Maaari kang magsimula sa sariling pamamahala at pisyikal na terapiya. Ang konservatibong pamamaraan na ito ay isang wastong paunang paggamot para sa maraming sugat sa balikat at kondisyon ng kasukasuan. Maaaring imungkahi ng iyong doktor ang pagbabago ng mga gawin kung mayroon kang osteolysis, na ang pagkasira ng buto. Layunin ng pisyikal na terapiya na palakasin ang mga kalamnan sa paligid ng iyong balikat upang suportahan ang kasukasuan. Parehong epektibo ang mga konservatibong at operatibong paggamot para sa pamamahala ng osteoarthritis ng acromioclavicular na kasukasuan. Bigyan ng patas na pagkakataon ang non-operatibong paggamot na ito, dahil nakakatulong ito sa karamihan ng mga pasyente na may masakit na kondisyon sa lugar na ito.
Kung patuloy ang sakit, maaaring talakayin ng iyong doktor ang medikal na pamamahala. Kasama nito kadalasan ang mga gamot pang-alis ng sakit at anti-inflammatory na gamot upang bawasan ang pamamaga at hindi pagkacomportable. Maaari mo ring isaalang-alang ang mga injeksyon sa acromioclavicular na kasukasuan. Nag-aalok ang mga injeksyong ito ng 47% na tagumpay sa loob ng isang taon sa mga pasyente na may osteoarthritis ng acromioclavicular na kasukasuan. Tinitiyak ng injeksyon ang pagbaba ng pamamaga at sakit direkta sa lugar ng kasukasuan. Patuloy na pinaghahambing ng mga pananaliksik ang iba't ibang uri ng injeksyon ng steroid upang malaman kung alin ang pinakamainam para sa isolated na sakit ng kasukasuan. Habang ang ilang pasyente ay nakakahanap ng pangmatagalang ginhawa, ang iba ay maaaring kailangang mag-explora ng ibang mga opsyon kung ang epekto ng injeksyon ay mawawala.
Ang operasyon ay itinuturing kapag naabot na ng konservatibong alaga ang hangganan nito at patuloy na nakakaapekto ang sakit sa iyong pang-araw-araw na buhay. Parehong ang open at arthroscopic resection arthroplasty techniques ay nagbibigay ng predictible na pag-alis ng sakit para sa symptomatic na osteoarthritis ng acromioclavicular na kasukasuan. Ang prosedurang ito ay kinabibilangan ng pagtatanggal ng maliit na bahagi ng collarbone upang lumikha ng mas maraming espasyo at bawasan ang friction. Ang limitadong distal clavicle excision ay nagbabawas ng sakit at nagpapabuti ng function ng balikat sa midterm na follow-up sa mga pasyente na resistant sa konservatibong paggamot. Itatatakda ng iyong doktor kung ikaw ay isang magandang kandidato batay sa iyong partikular na mga sintomas at resulta ng imaging. Para sa ilang tao, sapat na ang simpleng pagtatanggal ng tisyu ng buto na ito upang ibalik ang kumportableng pakiramdam at galaw nang hindi nangangailangan ng mas komplikadong rekonstruksyon.
Ano ang inaasahan¶
Kung ikaw ay may diagnosis na wear-and-tear arthritis sa acromioclavicular (AC) joint ngunit walang sakit, malamang na mananatili itong ganito. Sa 90% ng mga pasyente, ang asymptomatic AC osteoarthritis ay nanatiling asymptomatic sa loob ng 7-taong panahon. Hindi mo kailangang mag-alala tungkol sa natuklasan na ito kung hindi ito nakakaabala sa iyo. Karaniwan ang pagkakakita ng mga senyales ng arthritis sa mga scan kahit walang mga sintomas.
Kung mayroon kang sakit, ang prognosis ay nakadepende sa kung paano mo ito pamamahalaan. Ang mga injection sa loob ng joint ay nag-aalok ng 1-taong rate ng tagumpay na 47%. Ibig sabihin, halos kalahati ng mga pasyente ay nakakakuha ng pangmatagalang ginhawa mula sa tratamientong ito. Kung hindi tumutulong ang mga injection, maaaring irekomenda ng iyong surgeon ang isang prosedura upang alisin ang isang maliit na bahagi ng collarbone. Ang limitadong distal clavicle excision ay nagbabawas ng sakit at nagpapabuti ng function ng balikat sa midterm follow-up para sa mga pasyente na hindi sumasagot sa conservative treatment.
Maaari kang maghanda ng predictable na ginhawa sa sakit kung pipiliin mo ang surgery. Parehong ang open at arthroscopic resection techniques ay nagbibigay ng ganitong ginhawa. Gayunpaman, mayroong natatanging hanay ng mga posibleng komplikasyon sa bawat approach. Tatalakayin ng iyong surgeon kung aling paraan ang pinakamainam para sa iyong partikular na anatomy at istilo ng buhay.
Kung iiwan mo ang symptomatic arthritis na walang tratamiento, maaari itong manatili. May ilang mga pasyente na nakakaranas ng patuloy na discomfort na nagbabawal sa mga araw-araw na gawain. Kung gagawa ka ng ibang surgeries sa balikat, tulad ng rotator cuff repair, ang hindi tratadong AC joint osteoarthritis ay nauugnay sa mababang percentage ng failure. Gayunpaman, ang osteoarthritis ay karaniwang nauugnay sa mas masamang final na clinical outcomes pagkatapos ng rotator cuff repair. Ang hindi gumagaling o muling napunit na rotator cuff ay nagpapataas din ng risk ng pag-unlad ng arthritis na ito.
Para sa mga severe na kaso, lalo na kung ikaw ay may reverse shoulder replacement, ang severe AC joint osteoarthritis ay nauugnay sa acromial stress fractures. Ang radiographic AC joint osteoarthritis ay karaniwan sa mga pasyente na dumaraan sa ganitong uri ng surgery. Babantayan ng iyong surgeon ang mga risk na ito nang mahigpit.
Sa kabuuan, iba-iba ang daloy ng AC joint arthritis. Maaari itong matigil sa pamamagitan ng conservative care, manatili kahit may tratamiento, o dahan-dahang umunlad. Karamihan sa mga pasyente ay nakakakita na ang mga targeted na treatments ay nagbibigay ng malaking pagpapabuti sa function at kaginhawaan.
Kailan pumunta sa doktor¶
Pumunta sa iyong GP kung mayroon kang patuloy na sakit na hindi gumagaling kahit magpahinga. Humingi ng pagsusuri ng espesyalista kung napapansin mo ang kahinaan o kawalan ng katatagan sa balikat. Humingi ng pag-aalaga kung ang kasukasuan ay nakakabit o biglang bumabagsak. Kontakin ang iyong surgeon kung ang mga sintomas ay nakakaapekto sa iyong pagtulog o trabaho. Biglaang paglala ng sakit ay dahilan din upang humingi ng tulong. Tandaan na ang asymptomatic wear-and-tear arthritis ay madalas na walang sakit sa loob ng pitong taon. Gayunpaman, ang hindi naaayos na mga isyu ay minsan ay nakakaapekto sa ibang pagkukumpuni ng balikat. Susuriin ng iyong doktor ang pagkapagod at talakayin kung makakatulong ang injeksyon. Ang maagang pagsusuri ay tinitiyak na makakakuha ka ng tamang pag-aalaga bago lumala ang kondisyon.
Evidence & references
Overview¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis [8].
- Open and arthroscopic resection arthroplasty techniques have unique sets of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique [8].
- Limited distal clavicle excision reduced pain and improved shoulder function at midterm follow-up in patients with AC joint osteoarthritis resistant to conservative treatment [9].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair [3].
- Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results [5].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete AC dislocations [21].
Anatomy & Pathophysiology¶
- Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation [10].
- None of the reconstruction strategies completely restored the shoulder girdle to its preinjured state [26].
- Kinematic changes resulting from AC joint dislocation could be a potential source of pain and dysfunction in the shoulder [27].
- Scapular and clavicular kinematics were affected in AC separation models [28].
- The position of the hook portion of a clavicle hook plate can predispose anatomic structures to post-operative complications of subacromial impingement and bony erosion [29].
- Future research should focus on addressing horizontal and rotational instability to restore native physiological and biomechanical properties of the AC joint [35].
- Coracoclavicular reconstruction with augmentation of the acromioclavicular joint provides improved horizontal stability compared to isolated coracoclavicular reconstruction [41].
- Adding a fixation of the AC joint minimizes lateral tilting of the scapula and maintains a more anatomic reposition result over time [45].
Classification¶
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Mild arthroscopic findings of acromioclavicular joint osteoarthritis may be clinically significant and warrant resection, but further characterization of such patients is needed [1].
- Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic acromioclavicular joint osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity of the joint but did not correlate with clinical results [11].
- The acromial center line to dorsal clavicle radiographic measurement and the use of the Alexander view provide a more realistic appreciation of true acromioclavicular joint displacement, especially in defining watershed cases (Rockwood types IIIA, IIB, and IV) [12].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the acromioclavicular joint is reproducible and provides additional information on the severity of the injury [24].
- Injuries to the sternoclavicular joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae [16].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
Clinical Presentation¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterisation of patients in whom mild arthroscopic findings of OA of the AC joint are clinically significant and warrant resection is needed [1].
- A distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Osteolytic changes seemed to be associated with incongruity of the AC joint, but did not correlate with clinical results [11].
- Additional research is needed to determine the main cause of pain in isolated acromioclavicular osteoarthritis and to compare clinical outcomes of intra-articular versus extra-articular injections [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness to palpation, female sex, dominant side surgery) [18].
- Recurrence of the initial dislocation after arthroscopically assisted reduction appears to be related to the onset of degenerative ACJ arthropathy [14].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder [4].
Investigations¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Preventive arthroscopic distal clavicle resection (DCR) is not recommended in patients with radiological but asymptomatic ACJ arthritis [19].
- Further characterization is needed to determine which patients with mild arthroscopic findings of AC joint OA are clinically significant and warrant resection [1].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty (RSA) [7].
- Severe ACJ osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Osteolytic changes in the AC joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Patients with edema on MRI were more likely to present with pain than patients without edema [43].
- Subchondral bone edema on histologic examination was more frequent in patients with pain [43].
- The outcomes of a preoperative AC injection suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome [6].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated AC osteoarthritis [13].
- Risk factors for subsequent distal clavicle excision after rotator cuff repair include tenderness to palpation at the AC joint, female sex, and surgery on the dominant side [18].
- Subsequent distal clavicle excision was performed in 40% of cases with a combination of the three identified risk factors (tenderness, female sex, dominant side) [18].
- The arthroscopic approach offers an advantage in diagnosing and treating occult intra-articular pathology during distal clavicle excision [20].
- Some persistent pain and osteoarthritis progression remain concerns in the revision of failed open anterior stabilization of the shoulder using arthroscopy [4].
- Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and provides additional information on injury severity, which may influence treatment decisions [24].
- The AC-DC measurement and use of the Alexander view provide a more realistic appreciation of true AC joint displacement, particularly in defining watershed cases (IIIA/IIB/IV) [12].
- Radiological failures were observed in 41% of cases in a prospective multicenter study of arthroscopic acute AC dislocation fixation [50].
Treatment¶
Non-Operative Management¶
- Conservative therapy is a valid initial treatment option for Rockwood Type V acromioclavicular dislocations [15].
- Non-operative reduction and stabilization is a valuable treatment option for acute high-grade acromioclavicular joint separations [33].
- Nonoperative treatment is helpful for most patients with painful conditions of the acromioclavicular joint, although those with osteolysis may need to modify their activities [44].
- Conservative and surgical treatments are both effective in the management of acromioclavicular joint osteoarthritis [17].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- Additional research is needed to determine the main cause of pain and to compare clinical outcomes of intra-articular versus extra-articular steroid injections for isolated acromioclavicular osteoarthritis [13].
Operative Management¶
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic acromioclavicular osteoarthritis [8].
- Limited distal clavicle excision reduces pain and improves shoulder function at midterm follow-up in patients with acromioclavicular joint osteoarthritis resistant to conservative treatment [9].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Further characterization is needed to identify patients in whom mild arthroscopic findings of acromioclavicular joint osteoarthritis are clinically significant and warrant resection [1].
- Conversion to anatomic coracoclavicular ligament reconstruction shows similar clinical outcomes compared to successful non-operative treatment in chronic primary type III to V acromioclavicular joint injuries at a minimum 5-year follow-up [49].
- The authors recommend anatomic reconstruction procedures for the treatment of chronic complete acromioclavicular dislocations [21].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair, and an unhealed or re-torn cuff increases the risk of osteoarthritis [23].
Diagnostic Considerations¶
- A distinction between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis appears unnecessary, as all patients were equally satisfied with the outcome of preoperative acromioclavicular injection [6].
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year course [2].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in the revision of failed open anterior stabilization of the shoulder [4].
Complications¶
- Asymptomatic AC-OA remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated ACJ osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Osteoarthritis is associated with poorer final clinical outcomes after rotator cuff repair [23].
- An unhealed or re-torn rotator cuff increases the risk of developing osteoarthritis [23].
- Severe AC joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty [7].
- Radiographic ACJ osteoarthritis is common in patients undergoing reverse shoulder arthroplasty [7].
- Some persistent pain and osteoarthritis progression remain concerns following arthroscopy in revision of failed open anterior stabilization of the shoulder [4].
- Recurrence of the initial dislocation after arthroscopically assisted reduction of acute AC joint dislocation appears to be related to the onset of degenerative ACJ arthropathy [14].
- Treatment of acute grade III and IV AC dislocations by synthetic ligament reconstruction carries a risk of significant early osteolysis [25].
- Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, complication rate, or revision rate [38].
- Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis but each has a unique set of potential complications [8].
Recovery¶
- Asymptomatic acromioclavicular osteoarthritis diagnosed by MRI remained asymptomatic in 90% of patients over a 7-year period [2].
- Untreated acromioclavicular joint osteoarthritis, whether symptomatic or not, encountered during arthroscopic rotator cuff repair is associated with a low percentage of failure [3].
- Limited distal clavicle excision for acromioclavicular joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up [9].
- Acromioclavicular injections offer a 1-year success rate of 47% in patients with acromioclavicular osteoarthritis [22].
- A preoperative acromioclavicular injection study suggested that distinguishing between symptomatic and asymptomatic radiographic acromioclavicular osteoarthritis is unnecessary, as all patients were equally satisfied with the outcome [6].
- Osteolytic changes in the acromioclavicular joint seemed to be associated with incongruity but did not correlate with clinical results [11].
- Recurrence of initial acromioclavicular joint dislocation appears to be related to the onset of degenerative acromioclavicular joint arthropathy [14].
- Treatment of acute grade III and IV acromioclavicular dislocations using synthetic ligament reconstruction gave satisfactory results in terms of recovery of strength, but evolution is not risk-free due to the onset of significant early osteolysis [25].
- Arthroscopic coracoclavicular ligament reconstruction with double-bundle soft tissue allograft for chronic type V acromioclavicular dislocations showed sustained and statistically significant improvements in functional outcomes, high rates of return to sport, and maintenance of active-duty military status at minimum 10-year follow-up [39].
- Minimally invasive coracoclavicular ligament augmentation with a flip button/polydioxanone repair for total acromioclavicular joint dislocation revealed excellent radiologic and clinical results with no subluxations or dislocations noted in short-term follow-up [48].
- Some persistent pain and osteoarthritis progression remain concerns in the arthroscopic revision of failed open anterior stabilization of the shoulder [4].
- Type V acromioclavicular dislocations may be given a trial of conservative therapy [15].
Key Evidence¶
- [L2] Further characterisation of patients in whom mild arthroscopic findings of OA of AC joint are clinically significant and warrant resection is needed. [1] (10.1007/s00167-014-3114-2)
- [L2] Asymptomatic AC-OA remained asymptomatic in 90% over 7 years. [2] (10.1016/j.jse.2019.04.004)
- [L2] Untreated ACJ osteoarthritis, symptomatic or not, encountered during arthroscopic RCR is associated with a low percentage of failure. [3] (10.1007/s00167-020-06098-y)
- [L4] Some persistent pain and osteoarthritis progression remain concerns. [4] (10.1016/j.arthro.2009.04.073)
- [L3] Clinicians should consider overreduction of the AC joint because it may lead to favorable radiological results. [5] (10.1177/0363546519862850)
- [L4] The outcomes of this study seem to suggest that a distinction between symptomatic and asymptomatic radiographic AC OA is unnecessary, as all patients were equally satisfied with the outcome. [6] (10.5397/cise.2023.00073)
- [L3] Radiographic ACJ osteoarthritis is common in patients undergoing RSA. [7] (10.1016/j.jseint.2021.11.008)
- [L5] Both open and arthroscopic resection arthroplasty techniques provide predictable pain relief for symptomatic AC osteoarthritis, though each has a unique set of potential complications that may be minimized with improved understanding of anatomy, biomechanics, and meticulous surgical technique. [8] (10.1177/0363546513485359)
- [L4] Limited distal clavicle excision of patients with AC joint osteoarthritis resistant to conservative treatment reduced pain and improved shoulder function at midterm follow-up. [9] (10.1016/j.otsr.2016.01.008)
- [L5] Anatomic techniques that address both coracoclavicular ligaments and the AC capsule are recommended to restore horizontal and vertical stability while allowing physiological rotation. [10] (10.1016/j.arthro.2019.01.038)
- [L4] The AC-DC measurement and use of the Alexander view provides the clinician with a more realistic appreciation of true AC joint displacement, especially in defining watershed cases (ie, IIIA/IIB/IV) and may better inform the decision-making process regarding management options and recommendations. [12] (10.1016/j.jse.2019.12.014)
- [L4] Additional research is needed to determine the main cause of pain and compare clinical outcomes of intra-articular versus extra-articular injections. [13] (10.5397/cise.2023.00311)
- [L4] Recurrence of the initial dislocation appears to be related to onset of degenerative ACJ arthropathy. [14] (10.1016/j.otsr.2017.11.001)
- [L4] This suggests that Type V AC dislocations may be given a trial of conservative therapy. [15] (10.1177/2325967115s00017)
- [L1] Injuries to the SC joint are uncommon, and recognition and classification are critical to proper management to minimize long-term sequelae. [16] (10.1177/0363546513498990)
- [L4] Conservative and surgical treatments are both effective in acromioclavicular joint osteoarthritis management. [17] (10.1007/s00167-020-06377-8)
- [L3] Risk factors for subsequent DCE included tenderness to palpation at the AC joint, female sex, and surgery on the dominant side, with subsequent DCE performed in 40% of cases with a combination of these 3 factors. [18] (10.1177/2325967119844295)
- [L1] Preventive arthroscopic DCR is not recommended in patients with radiological but asymptomatic ACJ arthritis. [19] (10.1177/0363546514547254)
- [L1] The arthroscopic approach offers a unique advantage in diagnosing and treating occult intra-articular pathology. [20] (10.1016/j.jse.2006.10.006)
- [L4] The authors recommend this procedure for the treatment of chronic complete AC dislocations. [21] (10.1016/j.injury.2010.09.023)
- [L4] AC injections offer a 1-year success rate of 47%. [22] (10.5397/cise.2023.00031)
- [L4] Osteoarthritis is associated with poorer final clinical outcomes, and an unhealed or re-torn cuff increases the risk of osteoarthritis. [23] (10.1016/j.otsr.2017.03.007)
- [L1] Evaluating the integrity of the capsuloligamentous structures stabilizing the AC joint is reproducible and gives additional information on the severity of the injury, which might also influence the treatment decision. [24] (10.1016/j.jse.2020.10.026)
- [L4] Treatment of ACD by synthetic ligament reconstruction gave satisfactory results, notably in terms of recovery of strength, but evolution is not risk-free with onset of significant early osteolysis. [25] (10.1016/j.otsr.2010.06.004)
- [L5] Although each technique was able to restore different elements of the joint kinematics, none of the strategies completely restored the shoulder girdle to its preinjured state. [26] (10.1177/03635465221095231)
- [L5] The kinematic changes could be a potential source of pain and dysfunction in the shoulder with AC joint dislocation. [27] (10.1177/0363546512458571)
- [L5] Scapular and clavicular kinematics were affected in AC separation models. [28] (10.1016/j.jse.2013.01.004)
- [L5] The observed frequency of hook contact with surrounding subacromial structures in a static shoulder confirms that the position of the hook portion of the implant can predispose anatomic structures to the post-operative complications of subacromial impingement and bony erosion. [29] (10.1016/j.injury.2009.12.012)
- [L4] Non-operative reduction and stabilization of high-grade AC joint separations seems to be a valuable treatment option. [33] (10.1007/s00402-020-03630-0)
- [L5] Future research should focus on addressing horizontal and rotational instability, to restore native physiological and biomechanical properties of the AC joint. [35] (10.1186/s12891-022-05935-0)
- [L1] Open and arthroscopic AC joint reconstruction techniques have no differences in loss of reduction, the complication rate, and the revision rate based on the available literature. [38] (10.1177/0363546518795147)
- [L4] Outcomes after arthroscopic CC reconstruction for chronic, type V AC dislocations in an active-duty military patient population show sustained and statistically significant improvements in functional outcomes as well as high rates of return to sport and maintenance of active-duty military status at long-term follow-up. [39] (10.1016/j.arthro.2025.05.008)
- [L1] Coracoclavicular reconstruction with augmentation of the acromioclavicular joint has been shown to provide improved horizontal stability in both biomechanical and clinical studies compared to isolated coracoclavicular reconstruction. [41] (10.1007/s00167-018-5152-7)
- [L4] Patients with edema on MRI were more likely to present pain than patients without edema, and subchondral bone edema on histologic examination was more frequent in patients with pain. [43] (10.1016/j.jseint.2020.03.007)
- [L5] Nonoperative treatment is helpful for most patients, although those with osteolysis may have to modify their activities. [44] (10.5435/00124635-199905000-00004)
- [L3] The presented data suggest adding a fixation of the AC joint to minimize lateral tilting of the scapula and maintain a more anatomic reposition result over time. [45] (10.1007/s00402-021-03761-y)
- [L4] The short-term follow-up of 15 recently operated patients reveals excellent radiologic and clinical results, with no subluxations or dislocations of the acromioclavicular joint noted. [48] (10.1016/j.arthro.2006.12.015)
- [L4] At a minimum 5-year follow-up, patients with successful non-operative treatment for type III-V ACJ injuries achieved similar clinical outcomes compared to those who were converted to ACCR. [49] (10.1007/s00167-020-06159-2)
- [L4] Surgery for AC dislocations is difficult with radiological results that must still be improved, as radiological failures were observed in 41% of cases. [50] (10.1016/j.otsr.2015.09.012)
References¶
[1] Outcome of distal clavicle resection in patients with acromioclavicular joint osteoarthritis and full‐thickness rotator cuff tear. Knee Surgery, Sports Traumatology, Arthroscopy. 2014. DOI: 10.1007/s00167-014-3114-2 [2] Seven-year course of asymptomatic acromioclavicular osteoarthritis diagnosed by MRI. Journal of Shoulder and Elbow Surgery. 2019. DOI: 10.1016/j.jse.2019.04.004 [3] Acromioclavicular joint arthritis is not an indication for routine distal clavicle excision in arthroscopic rotator cuff repair. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06098-y [4] The Role of Arthroscopy in Revision of Failed Open Anterior Stabilization of the Shoulder. Arthroscopy. 2009. DOI: 10.1016/j.arthro.2009.04.073 [5] Factors Predicting the Outcome After Arthroscopically Assisted Stabilization of Acute High-Grade Acromioclavicular Joint Dislocations. The American Journal of Sports Medicine. 2019. DOI: 10.1177/0363546519862850 [6] Diagnostic value of a preoperative acromioclavicular injection for symptomatic acromioclavicular osteoarthritis: a retrospective study of cross-sectional midterm outcomes. Clinics in Shoulder and Elbow. 2024. DOI: 10.5397/cise.2023.00073 [7] Severe acromioclavicular joint osteoarthritis is associated with acromial stress fractures after reverse shoulder arthroplasty. JSES International. 2022. DOI: 10.1016/j.jseint.2021.11.008 [8] Degenerative Joint Disease of the Acromioclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513485359 [9] Limited distal clavicle excision of acromioclavicular joint osteoarthritis. Orthopaedics & Traumatology: Surgery & Research. 2016. DOI: 10.1016/j.otsr.2016.01.008 [10] Editorial Commentary: Why We Have To Respect The Anatomy In Acromioclavicular Joint Surgery And Why Clinical Shoulder Scores Might Not Give Us The Information We Need!. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2019.01.038 [11] 10.1016-0020-1383-83-90092-x. n.d.. [12] Improved identification of unstable acromioclavicular joint injuries in a clinical population using the acromial center line to dorsal clavicle radiographic measurement. Journal of Shoulder and Elbow Surgery. 2020. DOI: 10.1016/j.jse.2019.12.014 [13] Isolated acromioclavicular osteoarthritis and steroid injection. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00311 [14] Arthroscopically assisted reduction of acute acromioclavicular joint dislocation using a single double-button device: Medium-term clinical and radiological outcomes. Orthopaedics & Traumatology: Surgery & Research. 2018. DOI: 10.1016/j.otsr.2017.11.001 [15] Successful Conservative Therapy in Rockwood Type V Acromioclavicular Dislocations. Orthopaedic Journal of Sports Medicine. 2015. DOI: 10.1177/2325967115s00017 [16] Instability and Degenerative Arthritis of the Sternoclavicular Joint. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513498990 [17] No differences between conservative and surgical management of acromioclavicular joint osteoarthritis: a scoping review. Knee Surgery, Sports Traumatology, Arthroscopy. 2021. DOI: 10.1007/s00167-020-06377-8 [18] Preoperative Factors Associated With Subsequent Distal Clavicle Resection After Rotator Cuff Repair. Orthopaedic Journal of Sports Medicine. 2019. DOI: 10.1177/2325967119844295 [19] Is Arthroscopic Distal Clavicle Resection Necessary for Patients With Radiological Acromioclavicular Joint Arthritis and Rotator Cuff Tears?. The American Journal of Sports Medicine. 2014. DOI: 10.1177/0363546514547254 [20] Arthroscopic versus open distal clavicle excision: Comparative results at six months and one year from a randomized, prospective clinical trial. Journal of Shoulder and Elbow Surgery. 2007. DOI: 10.1016/j.jse.2006.10.006 [21] Surgical treatment of chronic acromioclavicular dislocation: Comparison between two surgical procedures for anatomic reconstruction. Injury. 2010. DOI: 10.1016/j.injury.2010.09.023 [22] Mid- to long-term success rate and functional outcomes of acromioclavicular injections in patients with acromioclavicular osteoarthritis. Clinics in Shoulder and Elbow. 2023. DOI: 10.5397/cise.2023.00031 [23] Osteoarthritis after rotator cuff repair: A 10-year follow-up study. Orthopaedics & Traumatology: Surgery & Research. 2017. DOI: 10.1016/j.otsr.2017.03.007 [24] The ligamentous injury pattern in acute acromioclavicular dislocations and its impact on clinical and radiographic parameters. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2020.10.026 [25] Acute grade III and IV acromioclavicular dislocations: Outcomes and pitfalls of reconstruction procedures using a synthetic ligament. Orthopaedics & Traumatology: Surgery & Research. 2010. DOI: 10.1016/j.otsr.2010.06.004 [26] Differences between Coracoclavicular, Acromioclavicular, or Combined Reconstruction Techniques on the Kinematics of the Shoulder Girdle. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465221095231 [27] The Function of the Acromioclavicular and Coracoclavicular Ligaments in Shoulder Motion. The American Journal of Sports Medicine. 2012. DOI: 10.1177/0363546512458571 [28] Acromioclavicular joint ligamentous system contributing to clavicular strut function: a cadaveric study. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2013.01.004 [29] Subacromial morphometric assessment of the clavicle hook plate. Injury. 2010. DOI: 10.1016/j.injury.2009.12.012 [33] Can an acute high-grade acromioclavicular joint separation be reduced and stabilized without surgery? A surgeon’s experience. Archives of Orthopaedic and Trauma Surgery. 2020. DOI: 10.1007/s00402-020-03630-0 [35] Current concepts in acromioclavicular joint (AC) instability – a proposed treatment algorithm for acute and chronic AC-joint surgery. BMC Musculoskeletal Disorders. 2022. DOI: 10.1186/s12891-022-05935-0 [38] Current Concepts in the Operative Management of Acromioclavicular Dislocations: A Systematic Review and Meta-analysis of Operative Techniques. The American Journal of Sports Medicine. 2018. DOI: 10.1177/0363546518795147 [39] Arthroscopic Coracoclavicular Ligament Reconstruction With Double‐Bundle Soft Tissue Allograft for Chronic Type V Acromioclavicular Dislocations Shows Excellent Patient Outcomes and Return to Duty and Sport at Minimum 10‐Year Follow‐Up. Arthroscopy. 2025. DOI: 10.1016/j.arthro.2025.05.008 [41] Acromioclavicular joint augmentation at the time of coracoclavicular ligament reconstruction fails to improve functional outcomes despite significantly improved horizontal stability. Knee Surgery, Sports Traumatology, Arthroscopy. 2018. DOI: 10.1007/s00167-018-5152-7 [43] Histologic and magnetic resonance image evaluation in acromioclavicular joint osteoarthritis. JSES International. 2020. DOI: 10.1016/j.jseint.2020.03.007 [44] Painful Conditions of the Acromioclavicular Joint. Journal of the American Academy of Orthopaedic Surgeons. 1999. DOI: 10.5435/00124635-199905000-00004 [45] Additional acromioclavicular cerclage limits lateral tilt of the scapula in patients with arthroscopically assisted coracoclavicular ligament reconstruction. Archives of Orthopaedic and Trauma Surgery. 2021. DOI: 10.1007/s00402-021-03761-y [48] Minimally Invasive Coracoclavicular Ligament Augmentation With a Flip Button/Polydioxanone Repair for Treatment of Total Acromioclavicular Joint Dislocation. Arthroscopy. 2007. DOI: 10.1016/j.arthro.2006.12.015 [49] Conversion to anatomic coracoclavicular ligament reconstruction (ACCR) shows similar clinical outcomes compared to successful non‐operative treatment in chronic primary type III to V acromioclavicular joint injuries. Knee Surgery, Sports Traumatology, Arthroscopy. 2020. DOI: 10.1007/s00167-020-06159-2 [50] Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation. Prospective multicenter study of 116 cases. Orthopaedics & Traumatology: Surgery & Research. 2015. DOI: 10.1016/j.otsr.2015.09.012