Patients › Rehabilitation
Pagkakaisa ng Pulso
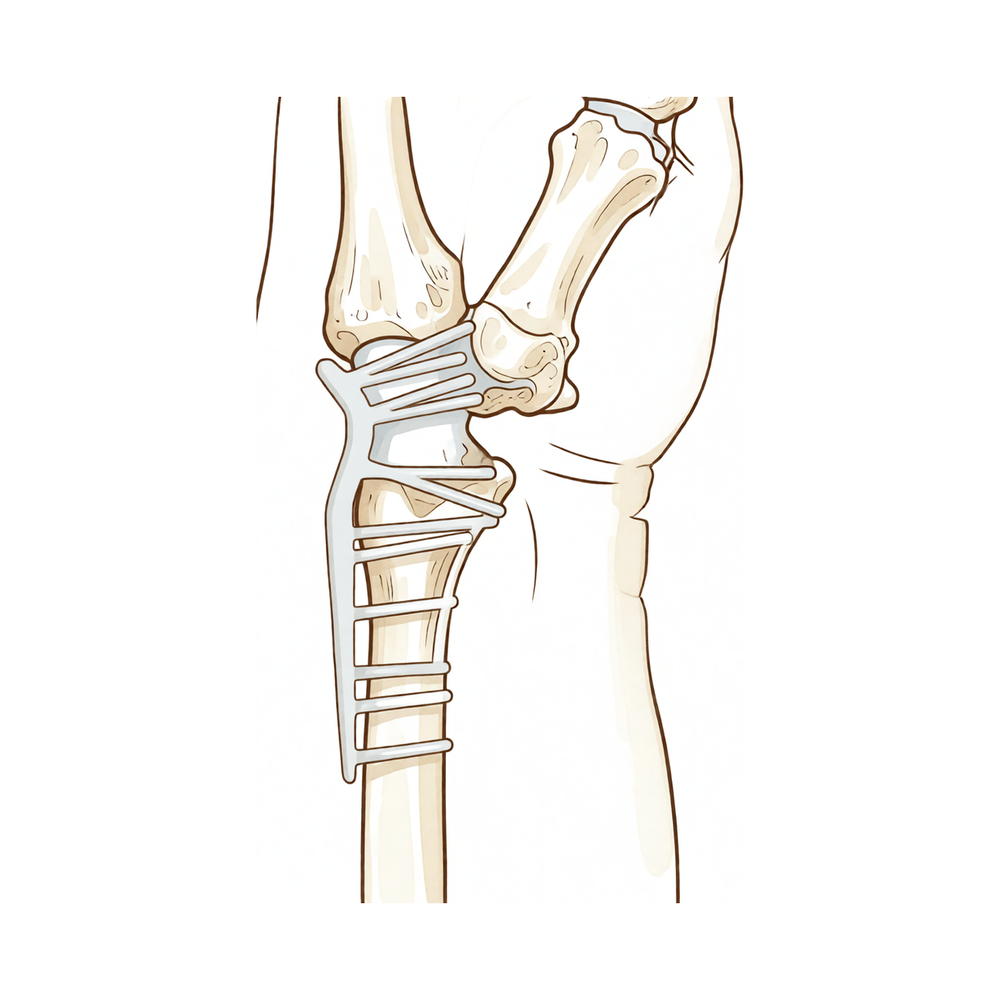
Isang plano ng paggaling pagkatapos ng kabuuang pagsasama ng pulso (arthrodesis), kung saan ang sira-sirang pulso ay pinagsama nang matibay gamit ang dorsal plate upang hindi na ito gumalaw ayon sa disenyo, habang ang mga daliri, hinlalaki, at pag-ikot ng forearms ay pinapanatiling gumagalaw mula sa simula, at ang hawak ay binubuo nang dahan-dahan pagkatapos magsama ang buto.
Ang protokol na ito ay gabay sa iyong paggaling pagkatapos ng total wrist fusion (tinatawag ding wrist arthrodesis, isang operasyon na nagpapatibay nang permanente sa sukat na pulso upang hindi na ito gumalaw) kay Dr Kieran Hirpara sa Mater Private Hospital Rockhampton. Nagsisimula ito sa iyong home exercise program, sinundan ng istrukturadong klinikal na protokol na isinulat para sa iyong hand therapist: dalhin ang pahinang ito o ang PDF nito sa iyong unang bisita sa terapiya upang manatiling koordinado ang iyong rehabilitasyon. Maaaring baguhin ng iyong therapist ang plano depende sa pag-unlad ng iyong paggaling.
Kung mayroon kang anumang alalahanin tungkol sa iyong sugat pagkatapos ng operasyon, makipag-ugnayan sa mga kwarto. Karaniwang makakatulong na kumuha ng litrato ng sugat at ipadala ito sa pamamagitan ng email para sa pagsusuri.
Ano ang inaasahan¶
Ang total wrist fusion (pagsasama ng buong pulso) ay ginagawa para sa pulso na nasira na sa lahat ng kanyang mga kasukasuan (end-stage o "pancarpal" arthritis) at masakit kapag gumagalaw. Sa halip na subukang panatilihin ang paggalaw ng nasirang kasukasuan, ang operasyon ay kunsintido nitong tinatanggal ang paggalaw: ang buto ng braso (radius) ay isinasama sa mga buto ng kamay (metacarpals) gamit ang dorsal plate na nakapaloob sa likod ng pulso, na nagtatakda ng pulso sa isang matigas na posisyon na bahagyang nakatutukoy pabalik (bahagyang extension) na pinakamainam para sa pagkapit. Sa mga sumunod na linggo, ang mga buto ay nagkakaisa (unite) upang maging isang matigas na bloke.
Ang pangunahing ideya ng paggaling na ito ay kabaligtaran ng karamihan sa mga operasyon: ang pulso ay dapat huminto sa paggalaw: iyon ang gamot, hindi komplikasyon. Kaya walang layunin na muling makuha ang paggalaw ng pulso, at walang mga ehersisyo upong yumuko o tuwidin ang pulso. Sa halip, ang buong rehabilitasyon ay nagpoprotekta sa dalawang bagay na hindi kinakaharap ng fusion at napakahalaga para sa pagganap ng kamay:
- Dapat manatiling ganap na mobile ang iyong mga daliri at hinlalaki. Ang mga matigas na daliri ang pangunahing dahilan kung bakit nababigo ang wrist fusion, kaya ang paggalaw ng mga daliri at hinlalaki ay nagsisimula mula sa unang araw.
- Ang pag-ikot ng braso (pag-ikot ng palad pataas at pababa) ay nananatili. Ang fusion ay hindi kasama ang paggalaw na ito, at kinukuha nito ang marami sa ginagawa noong panahon ng pulso (pag-ikot ng mga susi, gripo ng tubig, at hawakan ng pinto) kaya ito ay pinapanatiling malambot mula sa simula.
Dahil ang dorsal plate ay humahawak nang mahigpit sa mga buto (stable fixation), kailangan lamang ng magaan na splint o panluto para sa kaginhawaan, at ang maagang paggalaw ng mga daliri at braso ay hinahikayat imbes na pigilan. Kapag nagkaisa na ang buto (karaniwan sa loob ng anim hanggang walong linggo), nagsisimula ang pagpapalakas ng pagkapit. Maraming tao ang gumagana nang maayos pagkatapos ng wrist fusion, at dahil hindi na masakit ang pagkapit, ang lakas ng pagkapit ay madalas na umuunlad kumpara sa masakit na pulso bago ang operasyon.
Mga Paalala at Limitasyon¶
- Huwag subukang galawin ang sariling pulso: ito ay naka-fuse nang matigas ayon sa disenyo. Walang mga ehersisyo sa pagbaluktot ng pulso, ngayon man o sa hinaharap.
- Panatilihin ang paggalaw ng iyong mga daliri, hinlalaki, at pag-ikot ng forearms nang buo mula sa unang araw: ito ang pinakamahalagang bagay na maaari mong gawin para sa iyong kamay.
- Suotin ang iyong splint o panapos ayon sa utos para sa kaginhawaan at proteksyon hanggang sa magsama ang buto; panatilihin itong malinis at tuyo.
- Huwag mag-load o humawak nang mahigpit, at iwasan ang pag-angat ng higit pa sa isang magaan na tasa, hanggang sa magsama ang fusion at ikaw ay magkaroon ng pahintulot (karaniwan ay nasa anim hanggang walong linggo): ang mabigat na pag-load bago ang pagkakasama ay nagdudulot ng panganib na mabigo ang plate o ang fusion.
- Huwag magmaneho habang nasa splint ka o hindi ka makakontrol ng sasakyan nang ligtas; magpapatuloy ang pagmamaneho kapag wala ka nang sa splint at kayang-kaya mong hawakan ang manibela, ayon sa kumpirmasyon sa iyong review.
Para sa pangangalaga sa sugat, pamamahala ng pamamaga, at pag-aayos ng peklat, tingnan ang gabay ng klinika tungkol sa pangangalaga sa sugat.
Mga ehersisyo ninyo¶
Ito ang mga ehersisyo mula sa inyong handout. Simulan lamang ito ayon sa gabay ni Dr. Hirpara at ng inyong hand therapist. Ang mga unang ehersisyo ay nagpoprotekta sa mga natitirang galaw na pinapayagan ng fusion (paggalaw ng daliri at hinlalaki, pag-ikot ng forearms, at kontrol sa pamamaga) at walang isa sa mga ito ang kumakailangan ng galaw sa pulso, na nananatiling matibay. Ang pagpapalakas ng hawak ay nasa mas huling yugto at hindi dapat simulan hangga’t hindi pa nagkakaisa ang fusion at hindi pa kayo espesipikong pinapayagan. Itigil ang anumang nagdudulot ng matulis na sakit sa likod ng pulso.
Ang iyong klinikal na protokol¶
Ang natitirang bahagi ng pahinang ito ay ang yugto-yugto na klinikal na protokol para sa rehabilitasyon pagkatapos ng total wrist arthrodesis. Ang seksyong ito ay dapat ibigay sa iyong hand therapist, at bawat yugto ay nagsisimula sa isang paliwanag sa simpleng wikang Ingles kung ano ang nangyayari. Walang layunin sa wrist-ROM: ang radiocarpal (at karaniwang third carpometacarpal) joints ay pinagsama o fused gamit ang dorsal plate. Ang protokol ay umiiral upang mapanatili ang digital range, forearm rotation, at kontrol sa oedema habang nag-uunite ang fusion, pagkatapos ay magtayo ng grip sa stable na construct.
Bago ang paggamot, suriin ang operation report at past medical history ng pasyente, at makipag-ugnayan sa treating surgeon tungkol sa construct (dorsal arthrodesis plate; kung ang third CMC joint ay kasama o hindi), ang posisyon ng fused wrist, anumang bone graft na ginamit, at ang union status. Pinagsasama ni Dr. Hirpara ang wrist sa bahagyang extension gamit ang dorsal plate; ang fixation ay stable, kaya ang isang magaan na splint/dressing para sa kumportableng paggamit ay ginagamit imbes na matagal na rigid casting, at ang maagang digital at forearm motion ang pinagpupriorityhan.
Yugto I — protektahan ang konstruksyon, i-mobilisa ang mga malayang kasukasuan (linggo 0 hanggang 6)¶
Ang unang anim na linggo ay nagpoprotekta sa paggaling ng pagsasama habang pinapanatili ang ganap na paggalaw sa lahat ng mga bahaging hindi nasama. Isang magaan na splint o panapos ay isinusuot para sa kaginhawaan. Walang galaw ng pulso (ang konstruksyon ay rigid ay disenyo) at ang pokus ay ganap na nakatuon sa mga daliri, hinlalaki, forearms, at pamamaga.
Para sa iyong hand therapist:
Edukasyon at mga paalala - Splint/panapos para sa kaginhawaan at proteksyon hanggang sa klinikal at radiograpikong union; walang rigid at matagalang pag-cast na kinakailangan dahil sa stable na plate fixation - Walang mobilisasyon ng pulso: ang radiocarpal/CMC construct ay fused; walang target na ROM - Walang loaded grip o pag-angat na higit pa sa isang magaan na tasa hanggang sa kumpirmahin ang union - Mag-ingat sa digital stiffness: ang pangunahing banta sa resulta pagkatapos ng wrist fusion
Pamamahala - Sugat: mga surgical dressing ayon sa utos; tanggalin ang sutures at mag-review ng splint/X-ray sa humigit-kumulang 10–14 araw; monitor para sa impeksyon - Oedema: itaas ang kamay sa antas ng puso, mabagal na digital pumping, ice kung kinakailangan - Mga ehersisyo: buong aktibong AROM ng mga daliri at hinlalaki (composite fist → full extension, thumb opposition) mula sa unang araw; aktibong pronation/supination ng forearm; aktibong shoulder at elbow ROM; walang galaw ng pulso, walang resisted grip
Mga pamantayan para sa pag-progres - Nagsugpo ang sugat; pinapanatili ang buong o halos buong digital ROM; maagang radiograpikong mga senyales ng union sa humigit-kumulang anim na linggo
Yugto II — kumpirmahin ang pagkakaisa, simulan ang pag-load ng hawakan (linggo 6 hanggang 12)¶
Mula mga anim hanggang walong linggo, karaniwang nagkakaisa na ang pagsasanib sa X-ray, at kapag kumpirmado ito ng doktor, itatapon ang splint at sisimulan ang pagpapalakas ng hawakan. Patuloy ang trabaho sa forearms at mga daliri; ang pulso ay mananatiling fused at walang load hanggang sa kumpirmahin ang pagkakaisa.
Para sa iyong hand therapist:
Pagsusuri - Kumpirmahin ang estado ng pagkakaisa kasama ang treating surgeon bago mag-load; digital ROM; arc ng pag-ikot ng forearm; baseline ng hawakan; pagsusuri sa sugat/peklat
Edukasyon at mga paalala - Simulan ang hawakan at magaan na pag-load lamang pagkatapos kumpirmahin ng doktor ang pagkakaisa (karaniwang anim hanggang walong linggo) - Ang hardware sa dorsal wrist ay subcutaneous; bantayan ang paglabas/irritation at iulat ito - Patuloy na bigyang-priyoridad ang buong digital ROM sa buong yugto
Pamamahala - Mga ehersisyo: progressive pagpapalakas ng hawakan (malambot na bola → putty → graded grippers) kapag kumpirmado ang pagkakaisa; simulan ang pamamahala sa peklat kapag gumaling na ang sugat; patuloy na pag-ikot ng forearm at buong digital ROM; ipakilala ang magaan na functional na paggamit ng kamay - Ipaalam na ang pag-ikot ng forearm ngayon ang pumapalit sa nawalang galaw ng pulso sa mga pang-araw-araw na gawain (susi, tap, pag-ikot)
Mga pamantayan para mag-progres - Kumpirmadong pagkakaisa; walang sakit na magaan na hawakan; buong digital ROM; mobile na peklat
Yugto III — pagpapalakas at pagbabalik sa pagdadala ng bigat (linggo 12 pataas)¶
Kapag solid na ang pagkakaisa (fusion), walang mga limitasyon sa galaw na kailangang protektahan; ang kamay ay maaaring bigatan ayon sa kakayahin at unti-unting palakasin. Ang lakas ng hawak at kabuuang lakas ng kamay ay patuloy na umaayos sa loob ng ilang buwan, madalas na mas magaling pa kaysa bago ang operasyon dahil ngayon ay walang sakit sa paghawak.
Para sa iyong hand therapist:
Pagsusuri - Lakas ng hawak kumpara sa kabilang panig; pagsusuri sa functional at partikular sa trabaho/gawain; toleransya sa hardware
Edukasyon at mga paalala - Walang limitasyon sa galaw kapag nagkakaisa na; unti-unting dagdagan ang bigat ayon sa kakayahin - Mabigat/manual na pagdadala ng bigat ay unti-unting palakasin; ang buong pagtaas ng lakas ay patuloy hanggang sa humigit-kumulang labindalawang buwan
Pamamahala - Mga ehersisyo: progressive na resisted na grip at pagpapalakas ng forearms; unti-unting pagbabalik sa functional at trabaho; patuloy ang anumang natitirang trabaho sa mobility ng mga daliri - Isalang-alang ang discharge kapag functional at umaayos ang grip at pamamahalaan na ang mga pang-araw-araw na gawain; i-refer pabalik sa treating doctor kung lumitaw ang digital stiffness, persistent na irritation ng hardware, o masamang resulta
Mga pamantayan para sa pagbabalik sa pagdadala ng bigat - Solid na pagkakaisa; functional at umaayos na grip; walang sakit sa pagdadala ng bigat na partikular sa gawain
Pagbabalik sa trabaho at gawain¶
Ang magaan na paggamit ng kamay sa pang-araw-araw (pagkain, pagsulat, magaan na pag-aalaga sa sarili) ay inirerekomenda mula sa simula, hangga't komportable at hindi kumukubli nang mahigpit o nagtatayo ng higit pa sa isang magaan na tasa bago magsama ang pagsasama. Dahil hindi dapat magmaneho habang nasa splint o hindi kayang kontrolin ang sasakyan nang ligtas, magplano ng tulong sa transportasyon sa mga unang linggo; muling magmamaneho kapag wala na ang splint at kayang hawakan ang manibela, na kumpirmado sa iyong follow-up.
Ang pagkukubli na may bigat, pagtatayo, at paghila ay hintayin hanggang sa magsama ang pagsasama (karaniwang nasa anim hanggang walong linggo) at ikaw ay pinapayagan, at dahan-dahang pagpapalakas. Karamihan ay bumabalik sa opisina o magaan na trabaho sa loob ng tatlong buwan, habang ang mas mabigat o manual na trabaho ay mas maaga, batay sa mga pamantayan na tinataya ni Dr. Hirpara at ng iyong hand therapist kaysa sa kalendaryo lamang. Patuloy na pagpapalakas ng lakas hanggang isang taon, at dahil hindi na masakit ang sira na pulso, marami ang mas mahigpit na kumukubli at mas malaya na gumagamit ng kamay kaysa bago ang operasyon.
Pagkatapos ng iyong protocol¶
Ang protocol na ito ay kasabay ng pangkalahatang payo para sa paggaling ng klinika: tingnan ang pamamahala ng post-operative na sakit, pag-aalaga sa sugat, at pamamahala ng peklat. Ang naka-ayos na plano sa itaas ay sumasalamin sa mga publikadong resulta at gabay sa rehabilitasyon pagkatapos ng total wrist arthrodesis, at ang iyong patuloy na paggaling ay indibidwal na pinamumunuan ni Dr. Hirpara at ng iyong hand therapist ayon sa pag-unlad ng iyong fusion at kamay.
Evidence & references
Total Wrist Arthrodesis — Procedure Outcomes & Post-operative Rehabilitation (Radiocarpal Fusion, Dorsal Plate)¶
Topic scope: post-operative rehabilitation after total wrist arthrodesis — permanent surgical fusion of the radiocarpal (and usually the third carpometacarpal) joints with a dorsal arthrodesis plate, for end-stage pancarpal (panarticular) arthritis of the wrist. This is a salvage reconstruction that deliberately abolishes wrist motion, not a motion-preserving operation, so the rehabilitation has no wrist-ROM goal. It is built around preserving the joints the fusion leaves free — the fingers, thumb and forearm rotation — and controlling oedema while the fusion unites, then progressive grip loading once united.
Defining principle of the rehab here: total wrist fusion trades motion for a stable, pain-free wrist. The whole wrist is set solid (radius → metacarpals) in slight extension; loss of wrist movement is the intended endpoint, not a deficit to be rehabilitated. Modern dorsal locking-plate fixation is rigid enough that prolonged casting is unnecessary — so the deliberate priorities are early digital and forearm-rotation motion (digital stiffness is the principal threat to a good result) and swelling control, with grip strengthening deferred until radiographic union (typically 6–8 weeks). The single branch point is union status: loading is gated on the surgeon confirming the fusion has consolidated, after which there are no motion restrictions to protect.
A. PROCEDURE OUTCOMES (total wrist arthrodesis, dorsal plate)¶
Total wrist arthrodesis is a reliable, durable salvage for the painful, arthritic wrist that has failed non-operative care: the great majority of patients obtain lasting pain relief and a stable hand, accepting the loss of wrist motion in exchange.
- High union rates and durable pain relief. Plate arthrodesis is a well-established, reproducible operation; published series and the JAAOS review of indications and outcomes report reliable fusion, good pain relief and high patient satisfaction, with most patients willing to undergo it again [Wei & Feldon, JAAOS 2017; Shah et al., J Hand Surg Am 2022 — technique/modifications]. Moderate–strong (review + technique series).
- Grip strength is preserved or improves. Because gripping is no longer painful and the wrist is a stable platform, grip strength after fusion is typically equal to or better than the painful pre-operative wrist. A 2026 systematic review and meta-analysis of long-term grip strength after total wrist fusion (comparing inclusion vs sparing of the third CMC joint) confirms maintained long-term grip with comparable complication profiles between the two constructs [Lawson-Smith et al., J Hand Surg Glob Online 2026]. Moderate (SR/meta-analysis).
- Function is good for daily tasks; forearm rotation compensates for lost wrist motion. Patients adapt well because forearm pronation/supination (unaffected by the fusion) substitutes for much of the lost wrist arc in activities such as turning keys, taps and handles. Carpometacarpal-joint– sparing plate designs aim to retain a small amount of motion and reduce distal hardware issues [Briotti et al., HAND 2022 — Medartis CMC-sparing plate]. Moderate (cohort).
- Complications are defined and manageable. Principal complications are nonunion, hardware prominence/irritation requiring plate removal (the dorsal plate is subcutaneous), wound issues, and adjacent-segment problems (distal radioulnar joint / digital stiffness). These are recognised, generally treatable, and informed-consent staples rather than common catastrophes [Wei & Feldon, JAAOS 2017; Kalb & Prommersberger, Oper Orthop Traumatol 2009 — AO plate technique]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE¶
The rehab questions after total wrist fusion are different from a motion-preserving operation: there is no wrist arc to recover. The evidence and consensus instead converge on early mobilisation of the unfused joints, oedema control, and union-gated grip loading, exploiting the stability of modern plate fixation.
- Stable plate fixation permits early digital and forearm motion. Rigid dorsal locking-plate constructs are robust enough that prolonged rigid immobilisation is unnecessary; a light splint or dressing for comfort, with immediate finger, thumb and forearm-rotation motion, is the intended default [Shah et al., J Hand Surg Am 2022; Kalb & Prommersberger, Oper Orthop Traumatol 2009]. Moderate (technique consensus).
- Preserving digital range is the priority — stiffness is the main avoidable failure. Because the hand's function after fusion depends entirely on the joints left mobile, full active finger and thumb range from day one, plus preserved forearm rotation, is the core therapeutic aim. This is a mechanistic/consensus position rather than one from comparative rehab trials. Weak–moderate (mechanism strong, dedicated rehab RCTs absent).
- Grip strengthening is deferred to union, then progressed freely. Loaded grip is withheld until the surgeon confirms radiographic union (commonly 6–8 weeks), after which there are no motion restrictions and strengthening is progressed as tolerated; grip continues to improve for several months. Consensus / protocol-based.
- Hand therapy targets the free joints, not the wrist. Published patient-guidance protocols and surgical references describe early referral to a hand therapist for finger and forearm mobility and later putty-based grip strengthening — there is no wrist-ROM component by design [AAOS OrthoInfo — Wrist Fusion; institutional post-op protocols]. Consensus (patient-guidance).
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect construct, mobilise free joints | Week 0–6 | Light splint/dressing for comfort; no wrist motion (fused) | Elevate; immediate full finger + thumb AROM; forearm pronation/supination; elbow/shoulder ROM; oedema control | Light functional use only; no loaded grip / lifting > a light cup | Sutures + splint/X-ray review ~10–14 days. Digital stiffness is the chief threat |
| II — Confirm union, begin grip loading | Week 6–12 | Loading gated on surgeon-confirmed union (≈6–8 wk) | Splint discarded at union; progressive grip (ball → putty → grippers); scar massage once healed; continue forearm + digital ROM | Grip introduced light → graded after union | Forearm rotation substitutes for lost wrist motion. Watch dorsal hardware prominence |
| III — Strengthening & return to load | Week 12 → 12 months | None once united | Progressive resisted grip/forearm strengthening; work-/task-specific loading | Full load as tolerated; heavy/manual built up gradually | Office/light work ~3 months; strength improves up to ~12 months, often exceeding pre-op (pain-free grip) |
(Phase windows mirror the precautions and recovery structure in the patient protocol; they are typical guides anchored to union, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Fusion vs total wrist arthroplasty. The central modern controversy. Systematic review of total wrist arthroplasty versus arthrodesis (originally in rheumatoid disease) found insufficient evidence to declare either superior, with arthroplasty preserving some motion at the cost of higher revision/implant-related complications, and fusion offering durability at the cost of motion [Cavaliere & Chung, Plast Reconstr Surg 2008]. A cost-utility analysis found arthrodesis and arthroplasty both reasonable, with trade-offs in motion, complications and cost [Cavaliere & Chung, J Hand Surg Am 2010]. The "where are we now" synthesis frames the choice as patient-specific (demand, bilateral disease, expectations) rather than a settled winner [Jump, Trail & Talwalkar, J Hand Surg Eur 2025]. Moderate; genuine equipoise.
- Arthrodesis as salvage for failed arthroplasty. Total wrist fusion reliably salvages a failed total wrist arthroplasty, though such salvage fusions behave somewhat differently (bone loss, grafting) from primary arthrodesis [Zijlker et al., J Hand Surg Eur 2021]. Moderate.
- Include or spare the third CMC joint. Constructs differ in whether the plate crosses the third carpometacarpal joint. Long-term grip and complication outcomes are broadly comparable between inclusion and sparing, with CMC-sparing designs aiming to reduce distal hardware issues and retain a trace of motion [Lawson-Smith et al., J Hand Surg Glob Online 2026; Briotti et al., HAND 2022]. Moderate.
- Hardware prominence and removal. The subcutaneous dorsal plate is a recognised source of irritation and a common reason for elective hardware removal once the fusion is solid — expected, not a failure of the operation [Wei & Feldon, JAAOS 2017]. Moderate.
- Special populations. In spastic/neurological wrists (e.g. cerebral palsy), fusion changes hand function in nuanced ways — improving positioning but with task-specific trade-offs — underlining that the goal is a useful stable position, not motion [Hargreaves, Warwick & Tonkin, J Hand Surg Br 2000]. Moderate (specialised cohort).
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (SR / meta-analysis): preserved-to-improved long-term grip strength after total wrist fusion; comparable outcomes between CMC-inclusion and CMC-sparing constructs [Lawson-Smith et al. 2026].
- MODERATE: reliable union, durable pain relief and high satisfaction with plate arthrodesis [Wei & Feldon 2017; Shah et al. 2022]; genuine equipoise between fusion and arthroplasty with motion-vs-durability/complication trade-offs [Cavaliere & Chung 2008, 2010; Jump et al. 2025]; fusion as salvage for failed arthroplasty [Zijlker et al. 2021]; defined complication set (nonunion, hardware removal, DRUJ/digital adjacent issues).
- WEAK / CONSENSUS: the specific early digital/forearm-motion, union-gated grip rehabilitation programme (mechanistically rationalised — stiffness avoidance — with no dedicated rehab RCTs); exact phase timings (typical, anchored to union rather than trial-derived); stable-fixation early-motion default from technique consensus [Shah et al. 2022; Kalb & Prommersberger 2009].
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Total Wrist Arthrodesis: Indications and Clinical Outcomes. J Am Acad Orthop Surg. 2017. DOI: 10.5435/jaaos-d-15-00424
- Radiocarpal Fusion: Indications, Technique, and Modifications. J Hand Surg Am. 2022. DOI: 10.1016/j.jhsa.2022.04.002
- Long-term Grip Strength and Complications After Total Wrist Fusion With and Without Inclusion of the Third Carpometacarpal Joint: A Systematic Review and Meta-analysis. J Hand Surg Glob Online. 2026. DOI: 10.1016/j.jhsg.2026.101022
- Wrist Arthrodesis Using the Medartis Carpometacarpal Joint Sparing Plate. HAND. 2022. DOI: 10.1177/15589447221141474
- A Systematic Review of Total Wrist Arthroplasty Compared with Total Wrist Arthrodesis for Rheumatoid Arthritis. Plast Reconstr Surg. 2008. DOI: 10.1097/prs.0b013e318180ece3
- A Cost-Utility Analysis of Nonsurgical Management, Total Wrist Arthroplasty, and Total Wrist Arthrodesis in Rheumatoid Arthritis. J Hand Surg Am. 2010. DOI: 10.1016/j.jhsa.2009.12.013
- Arthrodesis or arthroplasty, complete or partial: where are we at in the 21st century? J Hand Surg Eur Vol. 2025. DOI: 10.1177/17531934241296758
- Comparative outcomes of total wrist arthrodesis for salvage of failed total wrist arthroplasty and primary wrist arthrodesis. J Hand Surg Eur Vol. 2021. DOI: 10.1177/17531934211057389
- Die vollständige Versteifung des Handgelenks mit der AO-Handgelenk-Arthrodesenplatte (Complete wrist arthrodesis with the AO wrist arthrodesis plate). Oper Orthop Traumatol. 2009. DOI: 10.1007/s00064-009-1905-2
- Changes in Hand Function Following Wrist Arthrodesis in Cerebral Palsy. J Hand Surg Br. 2000. DOI: 10.1054/jhsb.2000.0366
Wrist-fusion rehabilitation / patient-guidance literature (URLs)¶
- American Academy of Orthopaedic Surgeons — Wrist Fusion (Wrist Arthrodesis), OrthoInfo (recovery timeline; fusion heals ~8–12 weeks; the fused wrist no longer moves; therapy for joints not fused). https://orthoinfo.aaos.org/en/treatment/wrist-fusion-wrist-arthrodesis/
- Wrist Arthrodesis Technique — postoperative care and approach considerations. Medscape eMedicine. https://emedicine.medscape.com/article/1241236-technique
- Total Wrist Arthrodesis (Wrist Fusion) — procedure and rehabilitation overview. Resurgens Orthopaedics. https://www.resurgens.com/hand-wrist/procedures/wrist-fusion-total-wrist-arthrodesis
- Full Wrist Fusion — Post-Operative Rehabilitation Protocol (institutional hand-therapy protocol; early digital/forearm motion, union-gated grip strengthening). Alaska Orthopedic. https://www.akortho.com/wp-content/uploads/Full-Wrist-Fusion.pdf