Patients › Rehabilitation
Fraktura ng Distal Radius (ORIF)
Staged rehabilitation after plate fixation of a distal radius fracture, from the first days to return to full activity.
Ang protokol na ito ay gabay sa iyong paggaling pagkatapos ng operasyong pagpapatibay (surgical fixation) ng frakturang distal radius (pulso) (open reduction and internal fixation, ORIF) kay Dr. Kieran Hirpara sa Mater Private Hospital Rockhampton. Nagsisimula ito sa iyong home exercise program, kasunod ang estrukturadong klinikal na protokol na isinulat para sa iyong physiotherapist o hand therapist: dalhin ang pahinang ito o ang PDF nito sa iyong unang bisita sa terapiya upang manatiling koordinado ang iyong rehabilitasyon. Maaaring baguhin ng iyong therapist ang plano depende sa pag-unlad ng iyong paggaling.
Kung mayroon kang anumang alalahanin tungkol sa iyong sugat pagkatapos ng operasyon, makipag-ugnayan sa mga kwarto. Karaniwang makakatulong na kumuha ng litrato ng sugat at ipadala ito sa pamamagitan ng email para sa pagsusuri.
Maaaring inaasahan¶
Para sa pangangalaga sa sugat, pamamagasan, at peklat, tingnan ang gabay ng klinika tungkol sa pangangalaga sa sugat.
Pagkatapos ng iyong operasyon, maaari kang irefer sa isang hand therapist para sa paggawa ng thermoplastic splint. Sa sitwasyong ito, ang splint ay suot pansamantala para sa kumportableng suporta at proteksyon, at kailangan pa ring tanggalin ang splint para sa iyong home exercise program. Kung irefer ka para sa splint, makakatanggap ka ng karagdagang impormasyon tungkol sa paggamit at pangangalaga nito.
Ang mga ehersisyo sa ibaba ay mahalaga para mabawi ang range of motion ng iyong mga daliri, pulso, at forearms. Ang init at yelo ay magagandang modalities na madalas ginagamit para mabawi ang galaw, muling mabawi ang function, at mapabuti ang kumportableng pakiramdam. Kapag ang sugat ay gumaling na, maaari kang maglagay ng init bago ang mga ehersisyo; ang ice pack ay maaaring gamitin pagkatapos upang pigilan o bawasan ang pamamaga.
Ang pamamahala sa peklat (lalo na ang masahe) ay napakahalaga pagkatapos ng distal radius surgery, upang ang mga tendon na dumadaan sa ilalim ng incision ay manatiling malaya ang paggalaw at hindi mahigpit (adherent) sa gumagaling na peklat.
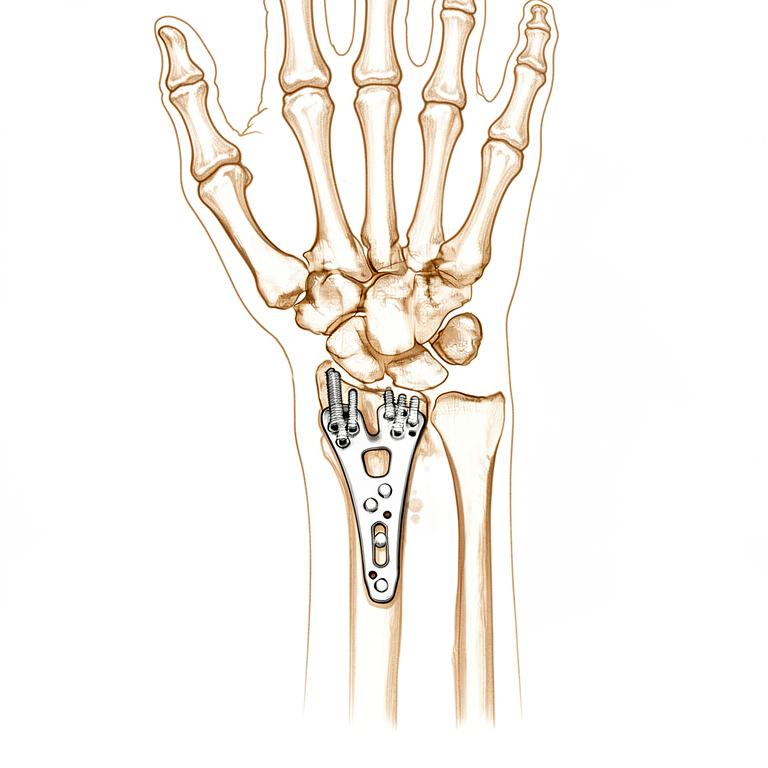
Ang volar locking plate ay dinisenyo upang hawakan ang fracture nang sapat na matibay upang magsimula ang paggalaw nang maaga, at ang protocol na ito ay nakabatay doon. Ang pananaliksik na nagkukumpara ng maagang paggalaw ng pulso sa ilang linggo ng immobilisation pagkatapos ng volar plate fixation ay nagpapakita na ang pag-simula ng paggalaw nang maaga ay maaaring mapabuti ang short-term na paggalaw, grip, at kumportableng pakiramdam nang hindi kinompromiso ang posisyon ng fracture [1][2]. Sa parehong oras, ang mga trial na nagkukumpara ng pag-simula ng paggalaw ng pulso sa humigit-kumulang dalawang linggo sa pag-simula ng paggalaw sa humigit-kumulang anim na linggo ay nagpakita na pareho ang dalawang grupo sa loob ng tatlo hanggang anim na buwan [3], kaya kahit mayroong maagang benepisyo, walang kailangang magmadali, at ang steady na progresyon na inilalarawan sa ibaba ay mahigpit na sinusuportahan. Ang paggaling ng buto ay sumusunod sa sarili nitong timeline anuman ang pakiramdam ng pulso, kaya ang mga huling precautions (walang weight-bearing, mabigat na pagbuhat, o contact sport hanggang 12 linggo pagkatapos ng fracture) ay pinapanatili kahit na ang paggalaw ay kumportable na.
Mga Paalala at Limitasyon¶
Ang magaan na gamit ng iyong kamay sa pang-araw-araw na gawain tulad ng pag-aalaga sa sarili, pagkain, paghuhubad, pagsusulat, at pag-type ay inirerekomenda.
Mahalagang iwasan ang pag-angat, paghawak, pagdadala ng bigat, at pagtama ng impact hanggang 8 linggo pagkatapos ng iyong operasyon. Ang banayad na pagpapalakas ay dahan-dahang ipinakilala mula sa ika-4 na linggo, nagsisimula sa magaan na ehersisyo ng mga daliri at isometric na ehersisyo ng pulso, at dahan-dahang pinapalakas nang maingat upang hindi masira ang maagang proteksyong ito.
Ito ang mga ehersisyo mula sa iyong handout, para sa pagbawi ng galaw ng iyong mga daliri, pulso, at forearms. Kung mayroon kang splint, alisin ito bago magsimula ng iyong mga ehersisyo. Simulan ang mga ito ayon sa gabay ni Dr. Hirpara at ng iyong therapist.
Mga ehersisyo mo¶
Ang iyong klinikal na protokol¶
Ang natitirang bahagi ng pahinang ito ay ang pinapabilis na klinikal na protokol para sa fracture ng distal radius na ginagamutan ng open reduction at internal fixation gamit ang volar plate. Ang seksyong ito ay dapat ibigay sa iyong physiotherapist o hand therapist, at ang bawat yugto sa ibaba ay nagsisimula sa isang simpleng paliwanag sa wikang Ingles tungkol sa nangyayari.
Araw 1–4 pagkatapos ng iyong operasyon¶
Sa unang ilang araw, ang pokus ay sa pagprotekta sa fixation, pagpapababa ng pamamaga, at pagpapanatili ng galaw ng iyong mga daliri, pulso, forearms, siko, at balikat. Mananatiling naka-putol ang iyong surgical bandage hanggang araw 3, kung kailan ito babawasan at ang sugat ay muling dadalhin. Panatilihing itaas ang kamay kapag nagpapahinga, gamitin ito para sa magaan na pang-araw-araw na gawain (sa ilalim ng 1–2 kg) sa loob ng komportableng limitasyon, at iwasan ang pagdudulot ng bigat sa pamamagitan ng braso, mahigpit na pagkapit, o pag-angat. Karaniwang hindi kailangan ang splint, ngunit maaari itong ayusin kung babalik ka sa trabaho o mas masakit ang pulso.
Para sa iyong physiotherapist:
Bago ang paggamot, suriin ang x-ray, operation report, at nakaraang medikal na kasaysayan (PMHx) ng pasyente, at makipag-ugnayan sa treating surgeon tungkol sa katatagan ng fixation ng fracture at ang inaasahang prognosis.
Edukasyon at mga paalala
- Iwasan ang pagdudulot ng bigat sa pamamagitan ng braso, mahigpit na pagkapit, o pag-angat
- Hikayatin ang paggamit ng apektadong kamay para sa magaan (mas mababa sa 1–2 kg) na mga gawain sa pang-araw-araw na buhay (ADL) sa loob ng limitasyon ng sakit at normal na mga pattern ng galaw
Pamamahala
- Splint: walang kinakailangan, ngunit maaaring gamitin kung babalik ang pasyente sa trabaho o sa pagkakaroon ng tumaas na sakit; isaalang-alang ang thermoplastic splint o off-the-shelf support
- Sugat: ang surgical dressings/bandage ay dapat iwan na buo hanggang araw 3; bawasan ang bandage at muling dalhin ang sugat mula araw 3 pagkatapos ng operasyon; edukasyon tungkol sa pamamahala ng sugat
- Oedema: magbigay ng edukasyon tungkol sa elevation; magbigay ng compression therapy at retrograde massage kung kinakailangan
- Mga ehersisyo: magbigay ng active six pack exercises upang mapanatili ang range of motion (ROM) ng mga daliri; magbigay ng active wrist, forearm, at finger range of motion exercises; hikayatin ang regular na active elbow at shoulder ROM
Linggo 2–4 pagkatapos ng operasyon¶
Matatanggal ang mga sutura sa araw 10–14, at sisimulan ang masahe ng peklat kapag sapat na ang paggaling ng sugat. Patuloy ang programa ng ehersisyo (titigil ang mga ehersisyong "six pack" kapag nabawi ng mga daliri ang buong galaw) at sisimulan ang banayad na pagpapalakas ng pulso sa pamamagitan ng aktibasyon ng kalamnan (isometric). Sa yugtong ito, dapat gumalaw ang pulso lamang sa sariling lakas ng kalamnan: walang sinuman, kasama na ikaw, ang dapat itulak o i-stretch nang passive, dahil patuloy pa ring nag-uunite ang fracture. Patuloy na iwasan ang pagdadala ng bigat, mahigpit na paghawak, at pag-angat; ang mga magaan na pang-araw-araw na gawain na may bigat na hindi lampas 1–2 kg ay inirerekomenda. Hindi dapat magmaneho habang naka-splint ang pulso; maaari nang magmaneho kapag lumabas na sa splint, ayon sa kumpirmasyon sa iyong follow-up.
Para sa iyong pisyoterapeuta:
Pagsusuri
- Mga self-reported na pagsusuri: Patient-Rated Wrist Evaluation (PRWE), Disabilities of the Arm, Shoulder and Hand (DASH)
- Sukat ng circumferential na edema
- Visual analogue pain scale (VAS) o numerical rating scale
- Sukat ng active range of motion (AROM) gamit ang goniometry: kamay, pulso
- Subjektibong pagsusuri, kabilang ang pagsunod ng pasyente sa programa, functional na paggamit ng kamay sa mga gawain sa ADL, at mga problema/alalahanin
Edukasyon at mga paalala
- Iwasan ang pagdadala ng bigat sa pamamagitan ng braso, mahigpit na paghawak, o pag-angat
- Walang passive na galaw ng pulso
- Hikayatin ang paggamit ng apektadong kamay para sa mga magaan (hindi lampas 1–2 kg) na gawain sa ADL sa loob ng hangganan ng sakit at normal na mga pattern ng galaw
- Walang pagmaneho habang naka-splint; maaari nang magmaneho kapag lumabas na sa splint, kumpirmado sa follow-up
Pamamahala
- Sugat/peklat: pagtatanggal ng sutura sa araw 10–14; simulan ang pamamahala ng peklat kung angkop, depende sa progreso ng paggaling
- Edema: isaalang-alang ang paggamit ng compression bandaging, retrograde na masahe, manual na mobilisasyon ng edema (MEM), contrast bathing, at/o elevasyon kung kinakailangan
- Mga ehersisyo: tigilin ang mga aktibong ehersisyong "six pack" kapag nakamit na ang buong range ng daliri; isaalang-alang ang mga passive na ehersisyo ng daliri at hinlalaki, kabilang ang place/hold, kung hindi pa buo ang active ROM sa kamay; patuloyin ang mga aktibong ehersisyo ng ROM ng pulso; hikayatin ang regular na aktibong elbow at shoulder ROM; simulan ang isometric na pagpapalakas ng pulso
Paglutas ng problema
- Monitor para sa mga senyales ng impeksyon sa sugat, pagbabago ng sensasyon sa kamay, o maagang mga senyales ng complex regional pain syndrome (CRPS)
- Tukuyin ang mga aberrant na pattern ng galaw at干预 kung kinakailangan
Linggo 4–6 pagkatapos ng operasyon¶
Ang pagpapalakas ay nagsisimula nang dahan-dahan sa yugtong ito: mababang resistensya sa pagpapalakas ng mga daliri mula linggo 4, habang patuloy ang isometric na trabaho sa pulso at unti-unting ina-upgrade. Kung sapat ang iyong x-ray at matatag ang fixation, maaaring magsimula ang mahinhing passive na pag-stretch ng pulso (kung saan ang pulso ay ginagalaw gamit ang tulong ng iyong ibang kamay o ng iyong therapist) sa 4–6 linggo. Ang pagpapanumbalik ng galaw ay nananatiling may mas mataas na prioridad kaysa sa pagpapalakas. Patuloy na iwasan ang pagbibigat sa pamamagitan ng braso at ang mabibigat na pag-angat, habang patuloy na ginagamit ang kamay para sa magaan na mga pang-araw-araw na gawain.
Para sa iyong physiotherapist:
Pagsusuri
- Sukat ng circumferential na edema
- Visual analogue pain scale o numerical rating scale
- Sukat ng AROM goniometry at kalidad ng mga pattern ng galaw
- Subjektibong pagsusuri, kasama ang pagsunod ng pasyente sa regimen, functional na paggamit ng kamay sa mga gawain sa ADL, at mga problema/alalahanin
- Lakas ng hawak gamit ang dynamometer (3 bawat limb)
Edukasyon at mga paalala
- Iwasan ang pagbibigat sa pamamagitan ng braso, o ang mabibigat na pag-angat
- Hikayatin ang paggamit ng apektadong kamay para sa magaan (mas mababa sa 1–2 kg) na mga gawain sa ADL sa loob ng hangganan ng sakit at normal na mga pattern ng galaw
Pamamahala
- Bakod: patuloy na pamamahala ng bakod ayon sa kinakailangan
- Edema: patuloy na compression therapy, retrograde na masahe, MEM at elevation ayon sa kinakailangan; itigil ang contrast bathing
- Mga ehersisyo: patuloy na passive na mga ehersisyo sa daliri at hinlalaki kung hindi pa buo ang ROM; patuloy na active na mga ehersisyo sa ROM ng pulso; simulan ang mga ehersisyo sa pagpapalakas ng daliri laban sa mababang resistensya sa 4 linggo; simulan ang mahinhing passive na mga ehersisyo sa pulso sa 4–6 linggo kung matatag ang ORIF at sapat ang x-ray; hikayatin ang regular na active na elbow at shoulder ROM; patuloy/upgrade ang isometric na mga ehersisyo sa pagpapalakas ng pulso
Paglutas ng problema
- Suriin para sa mga senyales ng CRPS at sakit sa balikat
- Isaalang-alang ang dami ng mga ehersisyo sa home programme at bigyang-priyoridad ang ROM kaysa sa lakas
- Kung ang ROM ng pulso ay malaki ang limitasyon, isaalang-alang ang pagsisimula ng mahinhing passive range of motion (PROM) na mga ehersisyo sa pulso sa loob ng 4/10 VAS, sa pag-apruba ng surgeon
Linggo 6–8 pagkatapos ng operasyon¶
Ang yugto na ito ay nagsisimula ng unti-unting pagbabalik sa buong aktibidad sa loob ng susunod na 3 linggo. Ang pagsasanay sa pagpapalakas ng pulso ay tataas hanggang sa magaan na timbang (0.5–1.0 kg) o mababang resistensyang theraband, at ang resistensya para sa pagsasanay sa pagpapalakas ng daliri ay tataas. May dalawang mahigpit na limitasyon na nananatili: walang pagdudulot ng bigat, mabibigat na pag-angat o sports na may kontak hanggang 12 linggo pagkatapos ng fracture. Ang iyong terapepista ay mag-aalis sa iyo kapag ikaw ay may buong galaw at angkop na pagbabalik ng function.
Para sa iyong physiotherapist:
Pagsusuri
- Sukatin ang circumferential na edema kung kinakailangan
- Visual analogue pain scale o numerical rating scale
- Sukatin ang AROM goniometry
- Lakas ng hawak
- Pagsusuri ng pakiramdam
Edukasyon at mga paalala
- Unti-unting pagbabalik sa buong aktibidad sa loob ng susunod na 3 linggo
- Iwasan ang pagdudulot ng bigat, mabibigat na pag-angat at sports na may kontak hanggang 12 linggo pagkatapos ng fracture
Pamamahala
- Bakawan: patuloy na pamamahala ng bakawan kung kinakailangan
- Edema: patuloy na pamamahala ng edema kung kinakailangan
- Mga ehersisyo: patuloy na passive na ehersisyo sa daliri at hinlalaki kung hindi pa buong ROM; patuloy na active at passive na ehersisyo sa ROM ng pulso kung kinakailangan; dagdagan ang resistensya sa mga ehersisyo sa pagpapalakas ng daliri; magsimula ng mga ehersisyo sa pagpapalakas ng pulso gamit ang 0.5–1.0 kg na timbang o mababang resistensyang theraband; i-upgrade ang mga timbang at resistensyang ginagamit sa programa sa pagpapalakas ng pulso ayon sa kakayahan
Paglutas ng problema
- Isaalang-alang/magsimula ng night serial progressive splinting, boxing glove o dynamic splinting kung mabagal ang pag-unlad ng ROM
- Subaybayan ang anumang senyales ng kawalan ng katatagan ng pulso at gamutin nang angkop
- Isaalang-alang ang pag-alis kapag buong ROM at angkop na pagbabalik ng function
- Isaalang-alang ang pagpapa-refer sa treating doctor kung ang kondisyon ay huminto at/or may mababang resulta
Ang protocol na ito ay isinulat kasama si Sarah Farrell, BOccThy AHT, at si Kristy Gerlach, BOccThy AHT.
Pagkatapos ng iyong protocol¶
Ang protocol na ito ay nagtatrabaho kasama ng pangkalahatang payo para sa paggaling ng klinika; tingnan ang pamamahala ng post-operative na sakit, pag-aalaga sa sugat at mga batayan ng hand therapy. Para sa operasyon mismo at sa pinsala na pinapagaling nito, tingnan ang distal radius fixation (ORIF) at distal radius fracture. Ang phased na plano sa itaas ay naaayon sa publikadong ebidensya tungkol sa rehabilitasyon pagkatapos ng volar locking plate fixation, at ang iyong patuloy na paggaling ay indibidwal na pinamumunuan ng iyong physiotherapist o hand therapist ayon sa kung paano ang pag-unlad ng iyong pulso.
Mga Sanggunian¶
[1] Quadlbauer S, Pezzei C, Jurkowitsch J, et al. Ang agad na paggalaw ng mga fracture ng distal radius na na-stabilize gamit ang volar locking plate ay nagdudulot ng mas magandang maikling panahong resulta kaysa sa limang linggong immobilization: isang prospective randomized trial. Arch Orthop Trauma Surg. 2022;142(5):1–11. https://pubmed.ncbi.nlm.nih.gov/34852677/ [2] Gutiérrez-Espinoza H, Araya-Quintanilla F, Olguín-Huerta C, et al. Epektibidad ng maagang kumpara sa huling paggalaw sa mga pasyente na may fracture ng distal radius na na-trate gamit ang volar locking plate: isang systematic review at meta-analysis. Hand Surg Rehabil. 2020;39(4):261–271. https://www.sciencedirect.com/science/article/abs/pii/S2468122920302231 [3] Lozano-Calderón SA, Souer S, Mudgal C, Jupiter JB, Ring D. Pag-galaw ng pulso pagkatapos ng volar plate fixation ng mga fracture ng distal bahagi ng radius. J Bone Joint Surg Am. 2008;90(6):1297–1304. https://pubmed.ncbi.nlm.nih.gov/18519324/ [4] Miller LK, Jerosch-Herold C, Shepstone L. Epektibidad ng mga teknik sa pamamahala ng edema para sa subacute hand edema: isang systematic review. J Hand Ther. 2017;30(4):432–446. https://pubmed.ncbi.nlm.nih.gov/28807598/
Evidence & references
Distal Radius Fracture (ORIF) — Post-operative Rehabilitation Evidence Brief¶
Topic scope: post-operative rehabilitation after open reduction and internal fixation (ORIF) of a distal radius fracture with a volar locking plate. This brief backs an early-motion-but-protected hand/wrist pathway delivered with hand therapy, where wrist motion begins early while bone-dependent loading (weight-bearing, heavy lifting, contact sport) is deferred until ~12 weeks. It does not cover the indications for surgery vs casting, nor fragment-specific/dorsal/bridge-plate constructs (which carry their own loading rules).
Defining principle of the rehab here: a volar locking plate is a fixed-angle construct stable enough to permit immediate wrist motion — the screws lock to the plate and hold the articular reduction independent of the cast. So (unlike a cast-treated fracture, and unlike a tendon or ligament repair) the wrist does not need weeks of immobilisation to protect the reduction: the rehab is an early-movement pathway — finger/forearm/wrist active motion and oedema control from day one, splint for comfort only, isometric then progressive strengthening from ~weeks 4–6. The one timeline that is not negotiable is bone healing: union takes ~6–12 weeks regardless of how the wrist feels, which is why weight-bearing, heavy lifting and impact are held to 12 weeks even once motion is comfortable.
A. PROCEDURE & CONSTRUCT — what the rehab is protecting¶
Volar locking plate fixation is the dominant operative construct for displaced distal radius fractures and is the reference standard against which other techniques are compared. Key surgical-outcome facts that shape the rehab:
- Volar locking plates restore and hold articular reduction reliably, and across randomised comparisons give equivalent or better functional outcomes than non-operative care and competing fixation methods (dorsal plating, intramedullary nailing, fragment-specific), with most differences favouring early function rather than final endpoint [JAAOS controversies review 2014; Hand Clinics plate-fixation review 2021; IM-nail-vs-volar-plate RCTs].
- The fixed-angle construct is the rationale for early motion. Because the locking screws hold the subchondral fragments rigidly, the plate — not a cast — maintains the reduction, so wrist motion can start before union without displacing the fracture [Hand Clinics 2021; accelerated-rehab RCT, JBJS 2014].
- In older patients the operative-vs-conservative outcome gap is small. A 3-year RCT in patients >70 found volar plating and non-operative care converged on similar patient-reported function — context that keeps post-operative rehab pragmatic and patient-centred rather than aggressive [BMC Musculoskelet Disord 2022; Hand Clinics geriatric review 2021].
- Recovery is gradual. Range, grip and patient-reported scores improve steadily over the first 3–6 months; the construct permits early motion but does not accelerate the biology of healing or the return of grip strength.
B. REHABILITATION / HAND-THERAPY EVIDENCE¶
The central rehab questions for this construct are (1) when to start wrist motion, (2) how much supervised therapy is needed, and (3) what the strengthening timeline should be. The evidence is clear on the first, nuanced on the second, and consensus-driven on the third.
- Early motion is safe and gives a short-term advantage. Multiple RCTs and a systematic review show that starting wrist motion early after volar plating improves short-term ROM, grip and comfort without compromising the radiographic reduction [accelerated-rehab RCT, JBJS 2014; early-vs-late motion RCT, HAND 2018; Hand Therapy systematic review 2020]. This is the direct warrant for the day-1 finger/forearm/wrist program in this protocol.
- "Early" need not mean "immediate," and the advantage washes out by 3–6 months. The landmark trial comparing wrist mobilisation at ~2 weeks vs ~6 weeks found the two groups equivalent by 3–6 months [Lozano-Calderón / JBJS 2008]. So there is a genuine early benefit but no penalty for a measured, comfort-led progression — which is exactly why this protocol can be unhurried.
- Routine supervised physiotherapy adds little over a coached home program for most patients. Systematic reviews and RCTs repeatedly find that a structured home exercise program preceded by instruction/coaching performs as well as formal supervised therapy for uncomplicated cases, and that prescribed exercise programs add limited benefit over advice for impairment/activity outcomes [HEP-vs-supervised SR, J Hand Ther 2014; J Physiother SR 2017; Hand Clinics "is therapy needed?" 2021; Arch Orthop Trauma Surg 2020]. This supports a home-program-first model with hand-therapy review, escalating supervision for stiffness, oedema or slow progress — the structure of this protocol.
- Oedema control and scar/tendon-glide management are standard therapy elements. Elevation, retrograde massage, manual oedema mobilisation and (early) compression are the evidence-informed oedema toolkit [edema-management SR, J Hand Ther 2017]; scar massage to keep the flexor tendons gliding under the volar incision is consensus hand-therapy practice rather than RCT-derived.
Phased post-op timeline (volar locking plate, early-motion pathway)¶
Phases match this topic's synthesis.md. Timings are post-operative weeks; the 12-week
loading limit is referenced to the fracture (injury) date.
| Phase | Window | Splint | Motion / use | Strengthening | Notes |
|---|---|---|---|---|---|
| I — Protect & move | Days 1–4 | Comfort only, not routine | Active finger (six-pack), wrist, forearm, elbow & shoulder ROM from day 1; light ADL < 1–2 kg within pain limits | — | Surgical bandage to day 3, then redress. Oedema control + elevation. No weight-bearing, gripping or lifting |
| II — Active range & oedema | Week 2–4 | Comfort/work only (no driving while splinted) | Continue active wrist ROM (no passive yet); six-pack stops once fingers full | Isometric wrist activation begins | Sutures out day 10–14; start scar massage once healed. Watch for CRPS. PRWE/DASH baseline |
| III — Passive range & light load | Week 4–6 | Off | Add gentle passive wrist stretches at 4–6 wk if x-ray satisfactory & fixation stable | Finger strengthening (low resistance) from wk 4; upgrade isometrics | Movement still prioritised over strength |
| IV — Graded strengthening & return | Week 6–8 | Off | Restore/maintain full active & passive ROM | Wrist strengthening with 0.5–1.0 kg / light theraband, progress as tolerated | Graded return over ~3 wk. No weight-bearing, heavy lifting or contact sport until 12 weeks post-fracture. Discharge on full ROM + functional return |
The phase structure mirrors published surgeon/hand-therapy ORIF protocols (early ROM → scar + oedema → passive range + light resistance → progressive strengthening, with heavy load/sport held to ~12–16 weeks) [Physiopedia Colles' ORIF protocol; institutional ORIF rehab guidelines].
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- How early to mobilise. Early motion (immediate–2 wk) gives a real short-term ROM/grip/comfort advantage that equalises by 3–6 months vs starting at ~6 weeks. The evidence therefore supports early motion but does not mandate aggression — a measured progression is fully defensible. Moderate–strong (multiple RCTs + SR).
- Supervised therapy vs coached home program. For uncomplicated fractures the best available evidence finds no consistent benefit of routine formal physiotherapy over a well-instructed home program; supervision is best targeted to stiffness, oedema, CRPS risk or slow progress. Moderate (SRs/RCTs), but heterogeneous.
- Strengthening and return-to-load timing. The week-by-week strengthening ramp and the 12-week loading hold are construct- and biology-based consensus, drawn from surgeon/hand- therapy protocols rather than a strengthening-timing RCT. Weak/consensus.
- Whether the wrist needs any immobilisation at all. Some trials report that omitting post-op immobilisation does not worsen outcomes after volar plating, supporting the "splint for comfort only" stance here. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG / MODERATE–STRONG (RCT / SR): early wrist motion after volar plating is safe and improves short-term ROM/grip/comfort without loss of reduction (accelerated-rehab RCT JBJS 2014; early-vs-late RCT HAND 2018; Hand Therapy SR 2020); ~2-wk vs ~6-wk mobilisation equivalent by 3–6 months (Lozano-Calderón JBJS 2008).
- MODERATE: volar locking plate is a reliable fixed-angle construct with equivalent/favourable outcomes vs alternatives (JAAOS 2014; Hand Clinics 2021); operative-vs-conservative outcomes converge in the elderly (BMC 2022); coached home program ≈ supervised therapy for uncomplicated cases (J Hand Ther 2014; J Physiother 2017; Hand Clinics 2021); evidence-based oedema management (J Hand Ther 2017).
- WEAK / CONSENSUS: the detailed strengthening ramp and 12-week loading limit (surgeon & hand-therapy protocols; biology- and construct-based, not trial-derived); scar/tendon-glide massage practice.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Accelerated rehabilitation compared with a standard protocol after distal radial fractures treated with volar open reduction and internal fixation. J Bone Joint Surg Am. 2014. DOI: 10.2106/jbjs.m.00860
- Wrist mobilization following volar plate fixation of fractures of the distal part of the radius. J Bone Joint Surg Am. 2008. DOI: 10.2106/jbjs.g.01368
- Early versus late motion following volar plating of distal radius fractures. HAND. 2018. DOI: 10.1177/1558944718787880
- A systematic review of how daily activities and exercises are recommended following volar plating of distal radius fractures and the efficacy and safety of early versus late mobilisation. Hand Therapy. 2020. DOI: 10.1177/1758998320967032
- AAOS/ASSH Clinical Practice Guideline Summary: Management of Distal Radius Fractures. J Am Acad Orthop Surg. 2022. DOI: 10.5435/jaaos-d-21-00719
- Controversies in the management of distal radius fractures. J Am Acad Orthop Surg. 2014. DOI: 10.5435/jaaos-22-09-566
- Plate fixation of distal radius fractures. Hand Clinics. 2021. DOI: 10.1016/j.hcl.2021.02.008
- Non-operative treatment or volar locking plate fixation for dorsally displaced distal radius fractures in patients over 70 years — a three-year follow-up of a randomized controlled trial. BMC Musculoskelet Disord. 2022. DOI: 10.1186/s12891-022-05394-7
- Distal radius fracture: HEP versus supervised therapy — a systematic review. J Hand Ther.
- DOI: 10.1016/j.jht.2013.08.017
- Prescribed exercise programs may not be effective in reducing impairments and improving activity during upper limb fracture rehabilitation: a systematic review. J Physiother. 2017. DOI: 10.1016/j.jphys.2017.08.009
- Is therapy needed after distal radius fracture treatment — what is the evidence? Hand Clinics.
- DOI: 10.1016/j.hcl.2021.02.012
- Rehabilitation after distal radius fractures: is there a need for immobilization and physiotherapy? Arch Orthop Trauma Surg. 2020. DOI: 10.1007/s00402-020-03367-w
- Management of complications of distal radius fractures. Hand Clinics. 2015. DOI: 10.1016/j.hcl.2014.12.002
- A comparison of the accuracy of two sets of diagnostic criteria in the early detection of complex regional pain syndrome following surgical treatment of distal radial fractures. J Hand Surg Eur Vol. 2012. DOI: 10.1177/1753193412469142
Distal radius / rehabilitation literature (URLs)¶
- AAOS/ASSH Clinical Practice Guideline Summary: Management of Distal Radius Fractures (full summary). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9196973/
- Practical application of the 2020 distal radius fracture AAOS/ASSH clinical practice guideline: a clinical case. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9035062/
- Rehabilitation for distal radial fractures in adults (Cochrane-style review). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9250132/
- Rehabilitation after distal radius fractures: opportunities for improvement. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC10569825/
- Rehabilitation following surgically treated distal radius fractures: do immobilization and physiotherapy affect the outcome? PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8343619/
Published rehab protocols (surgeon / hand-therapy — basis for the phase structure)¶
- British Society for Surgery of the Hand / British Association of Hand Therapists — Distal Radius Fractures Working Group rehabilitation guidance (2024). https://www.hand-therapy.co.uk/_userfiles/pages/files/distal_radius_fractures_working_group_2024.pdf
- Colles' Fracture Post-Operative Rehabilitation Protocol. Physiopedia. https://www.physio-pedia.com/Colles%E2%80%99_Fracture_Post_Operative_Rehabilitation_Protocol
- Distal Radius ORIF Rehabilitation Guidelines. University of Virginia Department of Orthopaedic Surgery. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Distal-radius-ORIF.pdf
- Distal Radius ORIF Rehabilitation. Jared Lee, MD. https://jaredleemd.com/pdf/distal-radius-orif-rehabilitation/