Patients › Rehabilitation
Mga ehersisyo bilang inpatient — shoulder replacement
Early in-hospital exercises after a shoulder replacement (total, reverse, or for fracture) — gentle hand, elbow and shoulder movement, with sleep-in-sling precautions for the first six weeks.

Ito ang mga marahang ehersisyo na sisimulan sa ospital pagkatapos ng iyong shoulder replacement (total, reverse, o replacement para sa isang bali). Pinapanatili nitong gumagalaw ang kamay, siko at balikat habang naghihilom ang repair.
Your exercises¶
Kieran Hirpara 4.0
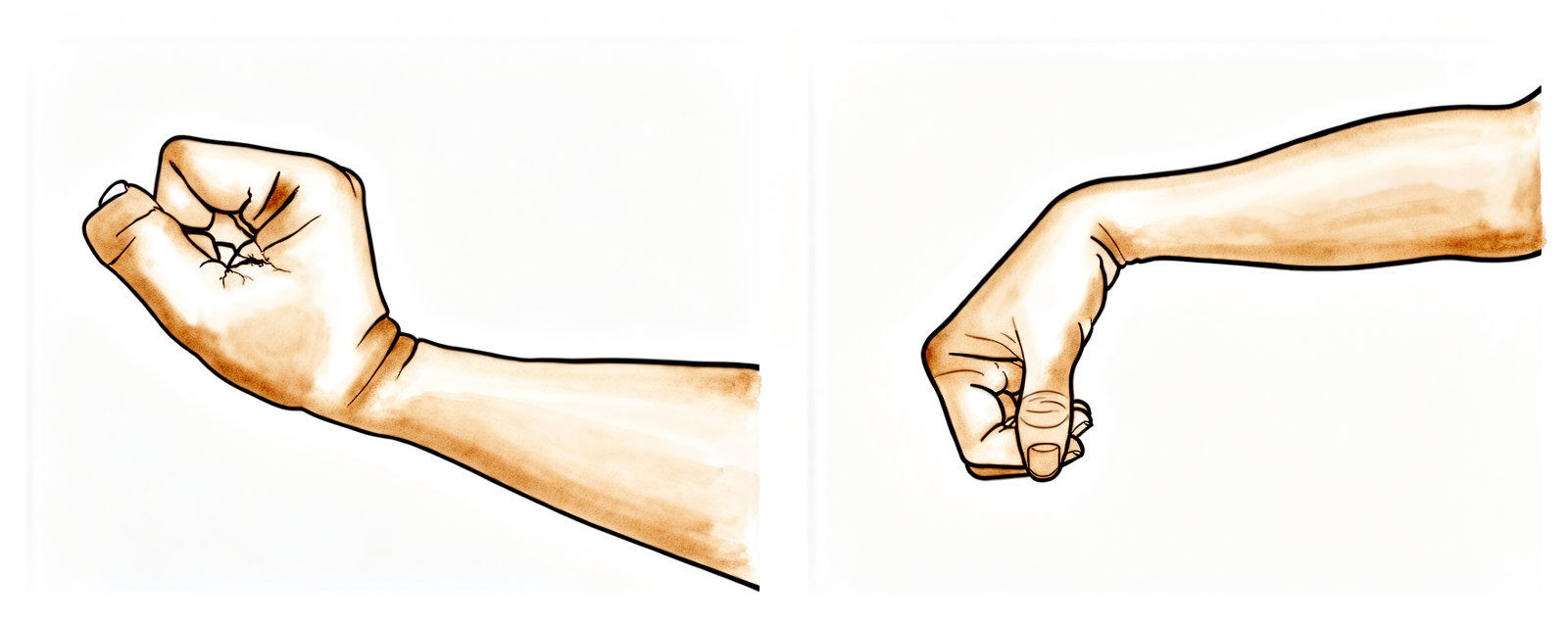
Paggalaw ng pulso
Panatilihing gumagalaw ang iyong kamay sa pamamagitan ng pagyuko ng iyong pulso pasulong, paurong at patagilid.
10 beses, 3 beses bawat araw
Kieran Hirpara 4.0
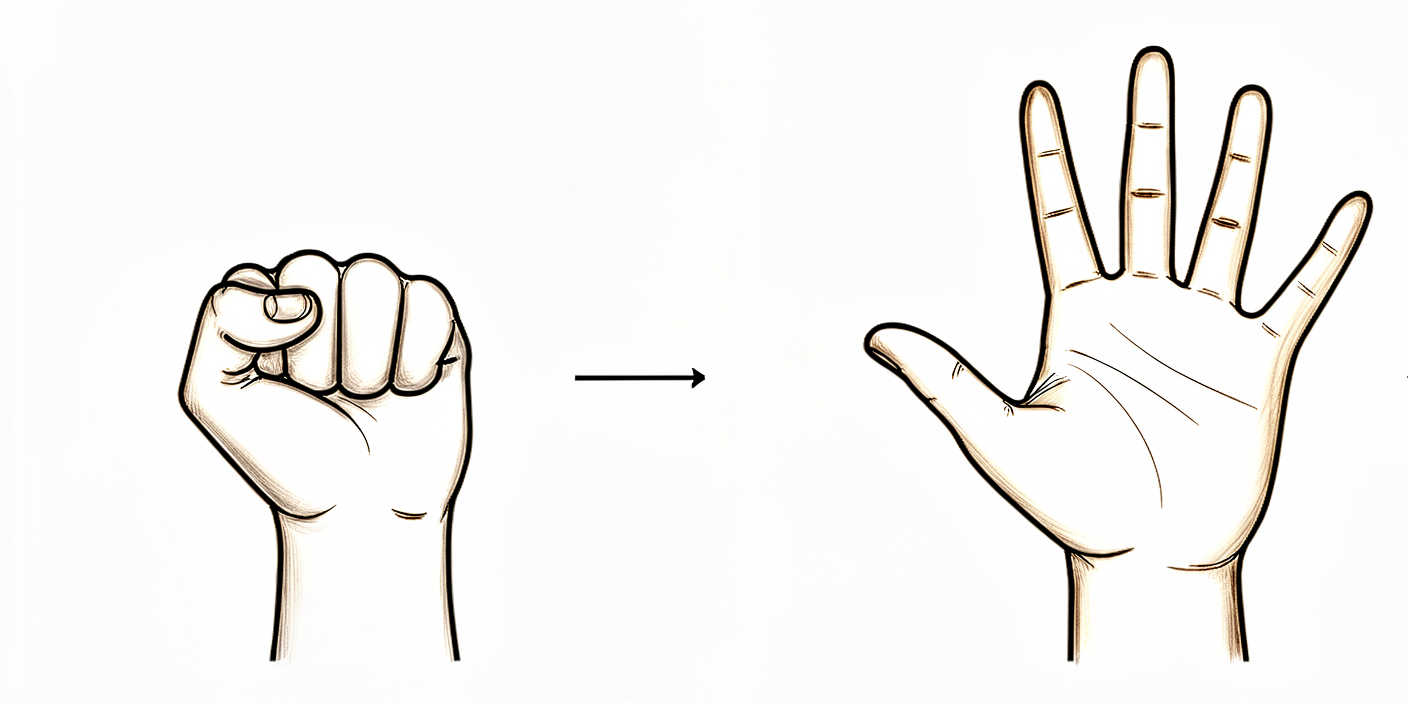
Pagbukas at pagsara ng kamay
Panatilihing gumagalaw ang iyong kamay at mga daliri sa pamamagitan ng pagbukas at pagsara ng mga ito, o sa pamamagitan ng pagpiga ng isang stress ball.
10 beses, 3 beses bawat araw

Kieran Hirpara 4.0
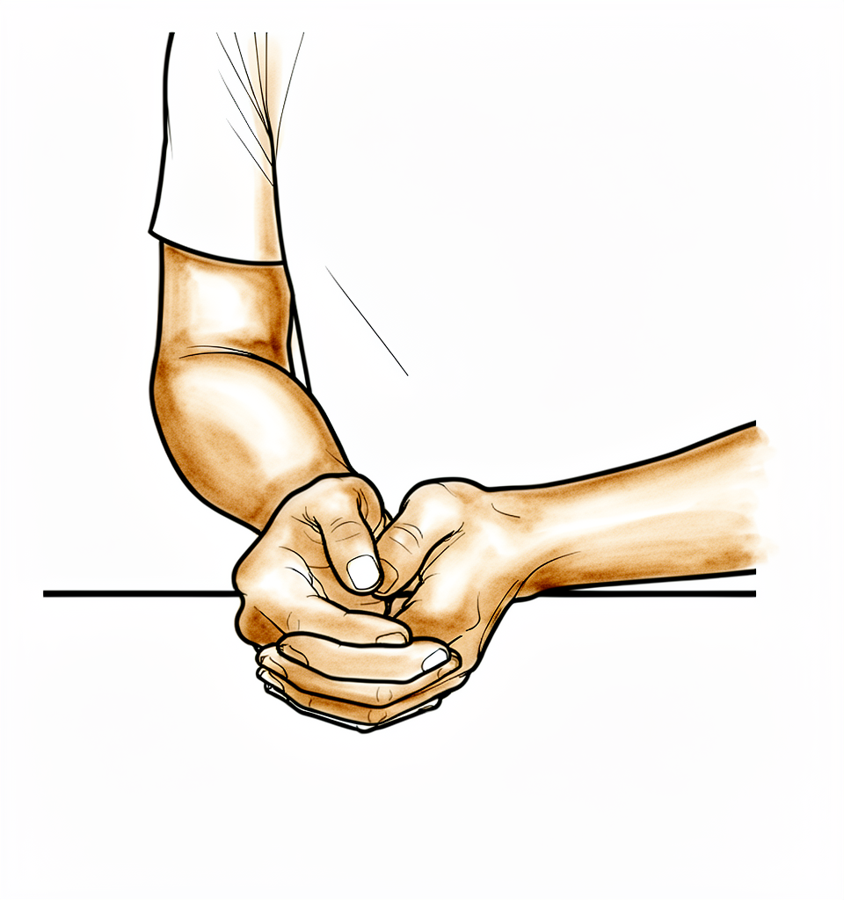
Pagbaluktot ng siko
Baluktutin at ituwid ang iyong siko.
10 beses, 3 beses bawat araw
Kieran Hirpara 4.0
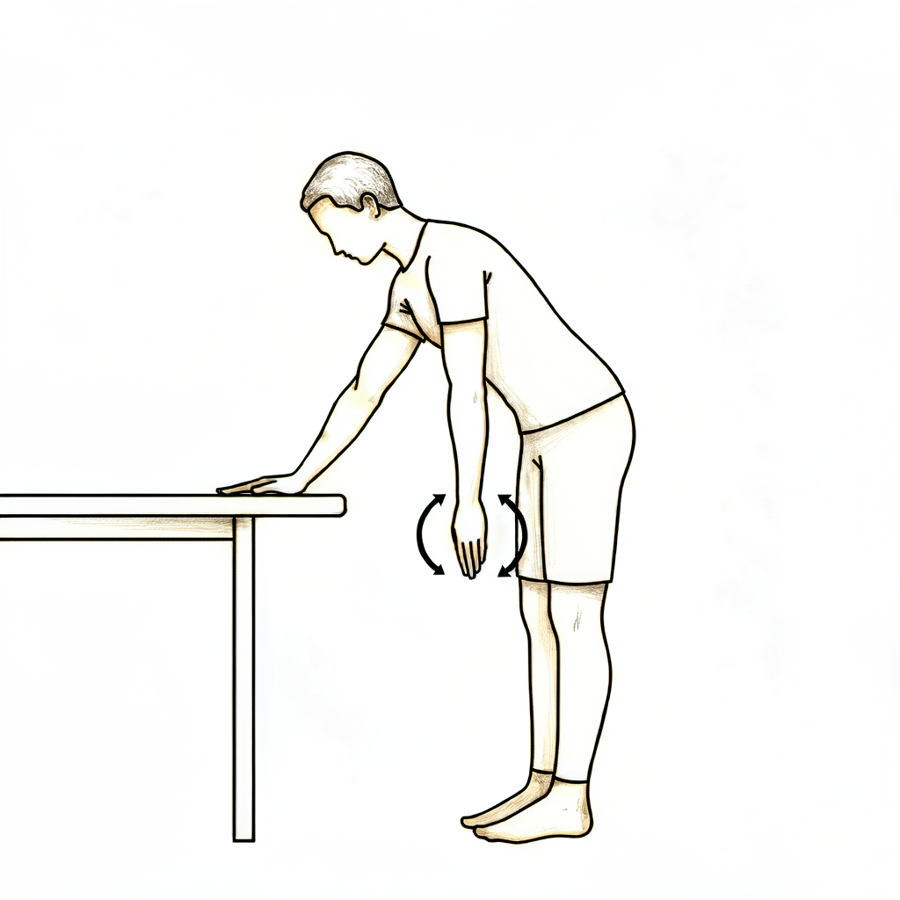
Mga pendulum
Ito ay isang passive na ehersisyo. Yumuko pasulong at hayaang lumuwag pababa ang iyong braso. Gamitin ang iyong katawan upang marahang igalaw ang braso nang pakanan o pakaliwang paikot, kasabay ng pasulong, paurong at patagilid.
Mga 30 segundo bawat direksyon, 3 beses bawat araw
Kieran Hirpara 4.0
Assisted forward flexion
Habang nakaupo sa upuan at nakayuko pasulong, kalungin ang iyong inoperahang braso gamit ang kabilang braso at marahang igalaw ito paitaas sa harap mo. Ibaba ito muli sa tulong ng iyong hindi inoperahang braso. Maaari mo ring higaan ang iyong likod sa kama at tulungan ang braso paitaas kung mas gusto mo.
10 beses, 3 beses bawat araw

Kieran Hirpara 4.0
Assisted abduction
Habang nakaupo sa upuan at nakayuko pasulong, kalungin muli ang braso at tulungan itong ilabas patagilid (tulad ng pag-uga sa isang sanggol).
10 beses, 3 beses bawat araw
Kieran Hirpara 4.0
External rotation
Habang nakaupo sa upuan, igalaw lang ang iyong braso mula sa kinalalagyan nito sa sling patungo sa pagtuturo nang diretso sa harap mo. Huwag nang lumagpas palabas.
10 beses, 3 beses bawat araw
Kieran Hirpara 4.0
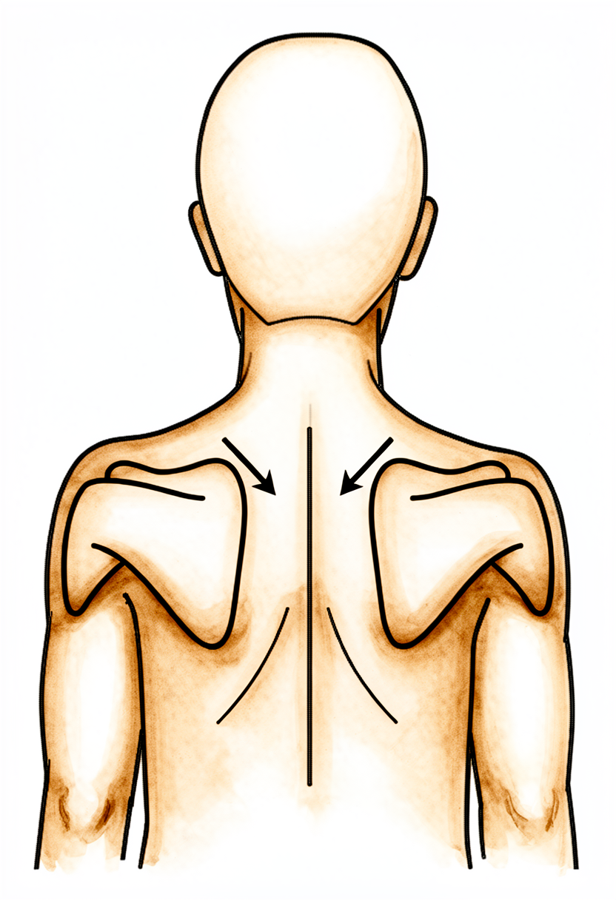
Lower trapezius setting
Pilipitin ang iyong mga balikat pababa at magkalapit.
Hawakan nang 5 segundo, 5 beses, 3 beses bawat araw
Kieran Hirpara 4.0
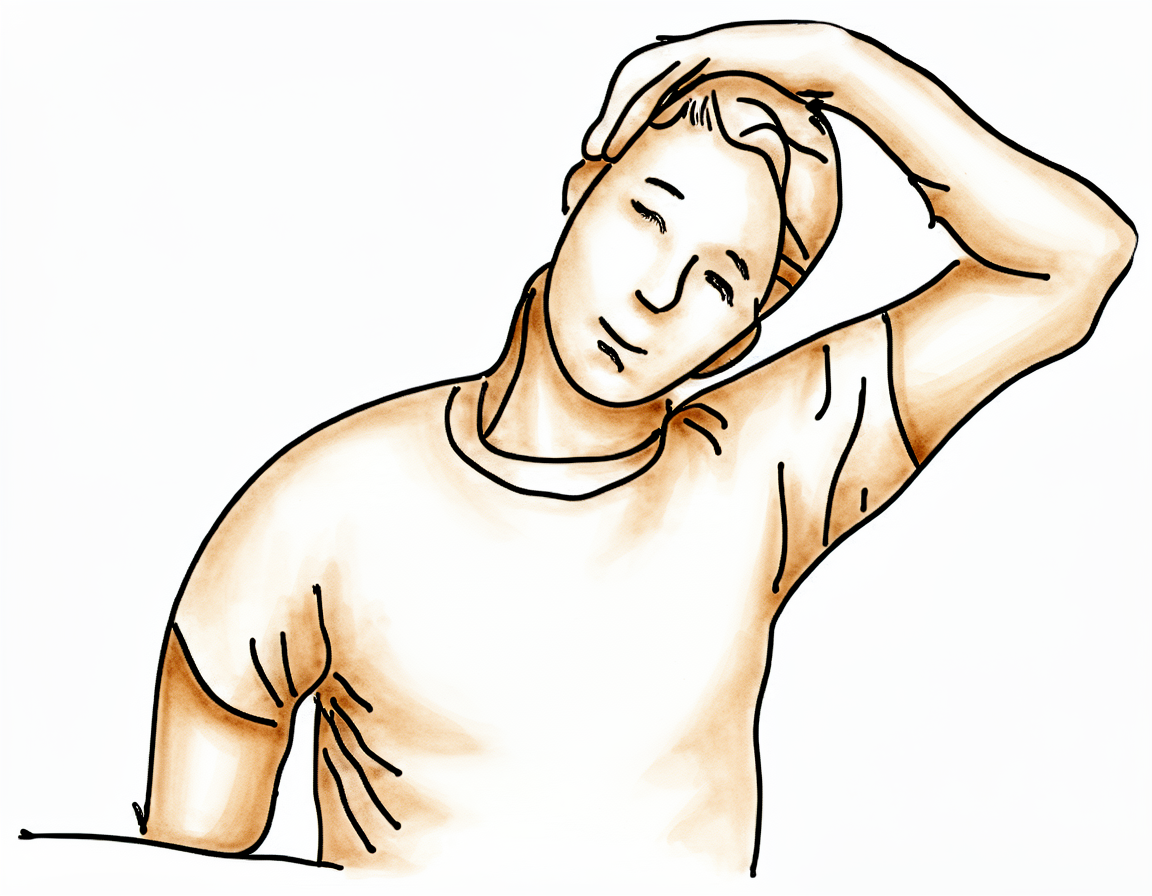
Upper trapezius stretch
Gamitin ang iyong hindi inoperahang braso upang ilapit ang iyong tainga sa iyong balikat, palayo mula sa inoperahang panig.
Hawakan nang 10 segundo, 3 beses, 3 beses bawat araw
Kieran Hirpara 4.0
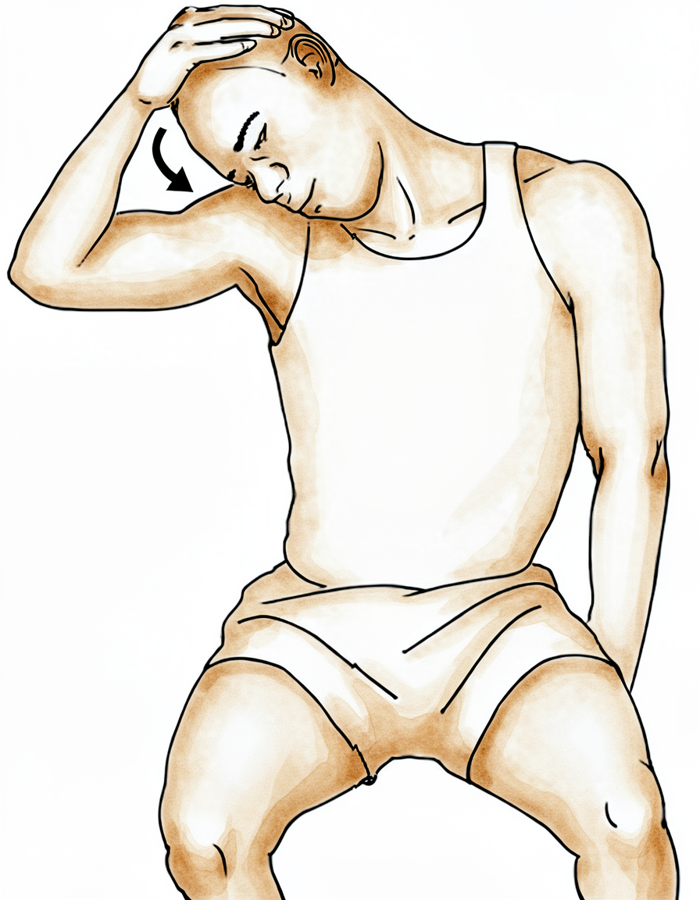
Levator scapulae stretch
Gamitin ang iyong hindi inoperahang braso upang ilapit ang iyong ilong sa bahagi ng iyong kilikili, palayo mula sa inoperahang panig.
Hawakan nang 10 segundo, 3 beses, 3 beses bawat araw
Kieran Hirpara 4.0
Rhythmic stabilisation
Habang suportado ang iyong braso sa harap mo sa mga taas ng balikat, hayaan ang iyong physiotherapist (o ang iyong magaling na kamay) na maglapat ng maliliit, marahang pagtulak mula sa iba't ibang direksyon habang pinapanatili mong nakatigil at matatag ang braso — huwag itong hayaang gumalaw. Sinasanay nito ang mga nagpapatatag na kalamnan ng balikat na tumugon. Panatilihing marahan ang lahat ng pagsisikap.
Ayon sa gabay ng iyong physiotherapist
Simulan ang mga marahang ehersisyong ito sa ospital at ipagpatuloy ang mga ito sa bahay. Dapat itong maging komportable; bumawi kung tumitindi ang sakit.
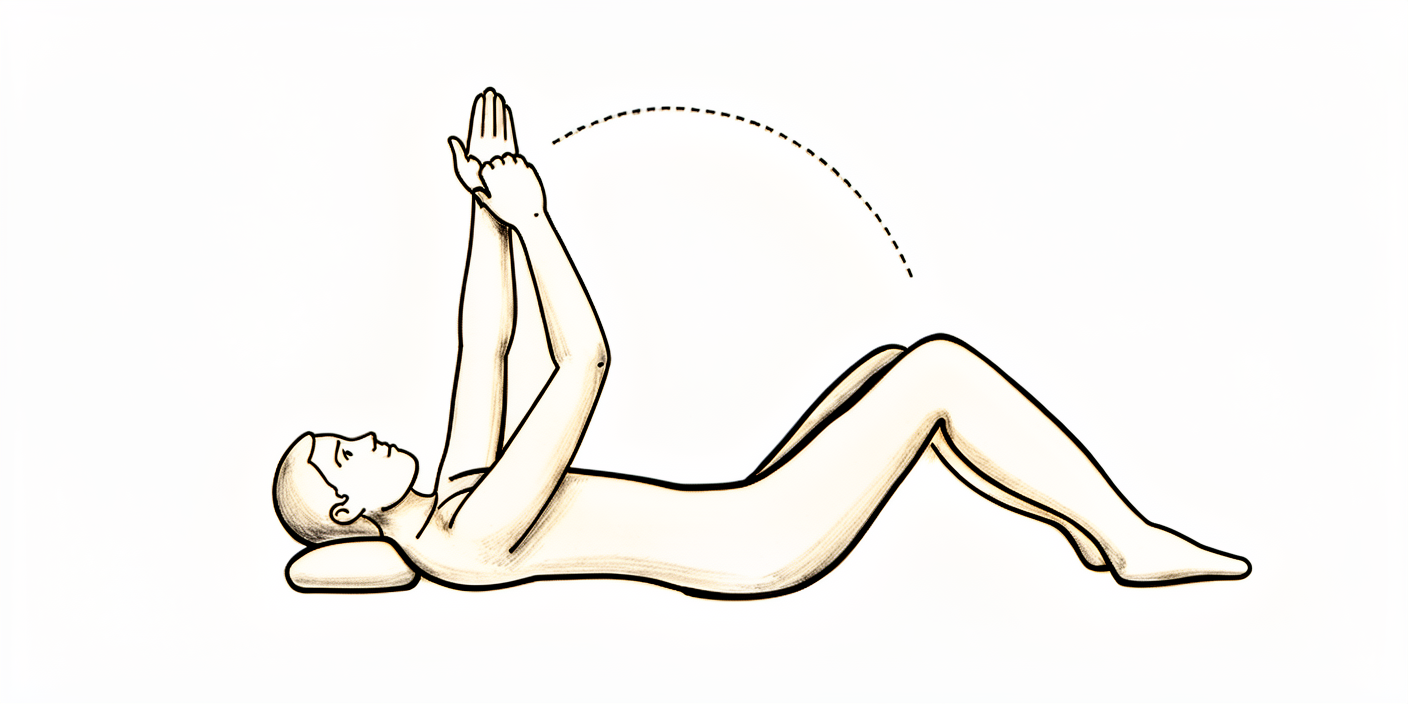
Kung nagkaroon ka ng reverse replacement, maaari mong simulang igalaw ang balikat nang maaga; magsimula sa mga assisted at gravity-assisted na paggalaw (pinakamadali kapag nakahiga sa iyong likod, hayaang tumulong ang gravity), pagkatapos ay magdagdag ng marahang aktibong paggalaw ayon sa kaya ng iyong kaginhawaan, na nananatili sa loob ng nararamdamang komportable. Iwasan lamang ang mga posisyong nakalista sa "Wearing your sling."
Kung nagkaroon ka ng total (anatomic) replacement o isang replacement para sa isang bali, panatilihing assisted at marahan ang iyong maagang mga paggalaw gaya ng ipinakita; hayaang ang iyong kabilang braso ang gumawa ng trabaho, at huwag itulak ang inoperahang braso palabas nang lampas sa hinihingi ng mga ehersisyo, upang maprotektahan ang naghihilom na repair sa harap ng balikat.
Wearing your sling¶
Ang tagal ng iyong pagsuot ng sling ay nakadepende sa kung anong replacement ang naganap sa iyo; mangyaring sundin ang panuntunan para sa iyong operasyon.
Kung nagkaroon ka ng reverse replacement:
- Ang sling ay pangunahin para sa kaginhawaan at suporta, at isusuot mo ito nang mga 2 linggo sa halip na buong panahon nang 6 na linggo.
- Maaari mong ilabas ang iyong braso mula sa sling para sa iyong mga ehersisyo at para sa pagligo.
- Maaari kang magsimula ng marahang mga paggalaw ng balikat kaagad (tingnan ang iyong mga ehersisyo); hindi na kailangang panatilihing ganap na nakatigil ang braso.
- May ilang posisyong dapat iwasan sa mga unang linggo habang nag-aayos ang lahat: huwag iabot ang iyong braso sa likod ng iyong katawan o sa likod ng iyong likuran, huwag pagsamahin ang pag-abot paurong sa pagbaling ng braso papasok, huwag magbuhat ng anuman, at huwag magtulak paitaas gamit ang iyong mga kamay (halimbawa, ang pagtulak ng iyong sarili paitaas palabas ng upuan). Tatalakayin ng iyong physiotherapist ang mga ito sa iyo.
Kung nagkaroon ka ng total (anatomic) replacement, o isang replacement para sa isang bali:
- Kailangan mong matulog nang naka-sling.
- Pinapayagan kang ilabas ang iyong braso mula sa sling para sa iyong mga ehersisyo at para sa pagligo.
- Kailangan mong isuot ang iyong sling nang 6 na linggo, lalo na kapag nasa labas ng bahay.
- Ang isang repair sa harap ng iyong balikat ay nangangailangan ng panahon upang maghilom, kaya ang iyong maagang mga paggalaw ay mas marahan at mas iniingatan; manatili sa mga assisted na ehersisyong ipinakita at huwag pilitin ang braso palabas nang lampas sa hinihingi ng mga ehersisyo.
Para sa lahat:
- Gumamit ng yelo para sa ginhawa sa sakit kung kinakailangan.
- Kapag nakasuot ng iyong sling, i-relax ang iyong balikat at hayaang ang sling ang bumuhat sa bigat ng iyong braso.
- Inumin ang iyong mga gamot sa sakit bago mo gawin ang iyong mga ehersisyo, at bago ang iyong mga appointment sa physiotherapy.
- Maliban kung ikaw mismo ang nag-ayos ng iyong sariling physiotherapy, may appointment nang ginawa para sa iyo at nakadetalye ito sa iyong discharge pack.
- Kung mayroon kang anumang problema, makipag-ugnayan sa mga rooms o ipaalam sa iyong physiotherapist.
When you go home¶
Kapag nasa bahay ka na, nagpapatuloy ang iyong paggaling sa buong rehabilitation protocol para sa iyong operasyon: reverse shoulder replacement; total shoulder replacement; shoulder replacement para sa bali.
Ang ebidensyang nasa likod ng maagang yugtong ito sa loob ng ospital (kung bakit mahalaga ang sling at ang marahang mga paggalaw, kung bakit maaaring gumalaw nang maaga at malaya ang isang reverse replacement na ang pangunahing pag-iingat ay ang paglayo ng braso sa pag-abot sa likod ng katawan, at kung bakit mas iniingatan ang isang total replacement na may limitadong external rotation upang protektahan ang repair sa harap ng balikat) ay nabuod sa seksyon ng ebidensya, na makukuha bilang PDF mula sa itaas ng pahinang ito.
Evidence & references
Inpatient (In-Hospital) Phase After Shoulder Replacement — Early Rehabilitation Evidence¶
Topic scope: This page covers only the early in-hospital phase of recovery after a shoulder replacement — the first days on the ward and the principles of the first protected weeks — for anatomic total shoulder arthroplasty (TSA), reverse total shoulder arthroplasty (RSA), and shoulder replacement performed for a proximal-humerus fracture. The companion patient page (the synthesis) lists the actual in-hospital exercises and sling rules; this page sets out the evidence behind them. The full course of rehabilitation for each operation lives in its own protocol — follow that one once you are home: total shoulder replacement, reverse shoulder replacement, and shoulder replacement for fracture, each of which carries its own detailed evidence page.
Defining principle of the early phase: the two pathways now differ. A reverse replacement is run on an accelerated, permissive footing, while an anatomic total replacement (and a replacement for a fracture) remains protective. In every case the hand/wrist/elbow are kept active from the start, but what the shoulder itself is allowed to do — and what is being protected — differs by operation:
- Anatomic TSA protects the subscapularis repair. To put the ball-and-socket implant in, the surgeon detaches and re-attaches the subscapularis tendon (or its bone block) at the front of the shoulder. Early external rotation is limited, active and resisted internal rotation is delayed, and shoulder elevation is kept passive/assisted — because these are the positions that strain the healing repair. This is why the in-hospital ER exercise only moves the arm from the sling position to pointing straight ahead — and no further. The sling is worn full-time for about 6 weeks.
- Reverse TSA is accelerated. Often there is no subscapularis repair to protect, and the deltoid (not the cuff) powers the arm, so the shoulder can move early. The sling is for comfort and support only (~2 weeks), and active-assisted and active-as-tolerated shoulder motion begins from the start (supine/gravity-assisted first), within comfort. The main early constraint is dislocation precautions, whose at-risk position is hand-behind-the-back (combined extension + adduction + internal rotation): avoid reaching the arm behind the body or behind the back, no lifting, and no pushing up through the hands. This aligns with the accelerated reverse literature (see the reverse protocol's evidence page).
- Replacement for fracture adds a third constraint: the tuberosities (the bony muscle attachments) must heal, so this pathway follows the protective line (like anatomic TSA) and is usually the most protective of the three.
Common to all three: the hand/wrist/elbow are kept active immediately, and adequate analgesia makes early gentle motion possible. The sling duration and how freely the shoulder moves then differ — permissive for reverse, guarded for anatomic and fracture.
The early in-hospital phase, in brief¶
Most patients stay in hospital a short time after a shoulder replacement — commonly about one to two nights, and selected patients are now safely discharged the same day. Before discharge the ward physiotherapist fits the sling, teaches independent sling management, and starts the gentle exercises shown in the synthesis: keeping the hand, wrist and elbow active; pendulums; and shoulder elevation — assisted (passive) and limited in external rotation after an anatomic repair, but active-assisted and active-as-tolerated from the start after a reverse replacement. The arm is commonly numb from a nerve block when you wake, with sensation returning over roughly 24 hours. The job of this phase is pain control, swelling reduction, keeping the non-shoulder joints moving, and protecting the new joint while it settles — not building strength, which comes later in the home protocol.
Evidence by theme¶
1. Length of stay is short, and same-day discharge appears safe in selected patients¶
Shoulder replacement has traditionally been an inpatient operation, but length of stay is short and falling. At an orthopaedic specialty hospital the average stay was about 1.3 days versus ~1.85 days at a general centre [RAG corpus — 10.1016/j.jse.2016.01.010]. A large series found same-day discharge was not inferior to a longer in-hospital stay for 90-day readmissions [RAG corpus — 10.1016/j.jse.2019.09.037], and outpatient TSA in an ambulatory centre was reported as a safe alternative to inpatient care in a matched cohort (2016 Neer Award) [RAG corpus — 10.1016/j.jse.2016.07.011]. Same-day discharge appears safe even in patients aged ≥65 with appropriate selection [RAG corpus — 10.1016/j.jse.2021.02.022]. Whether you stay one night or go home the same day is an individual decision; the early-exercise and sling principles are the same either way.
Evidence: MODERATE (cohort / matched-cohort data).
2. Pain control is the patient's and the system's primary early concern¶
When patients consider shorter stays, perioperative pain control is their primary concern [RAG corpus — 10.1016/j.jse.2022.07.009] — which is why the synthesis emphasises taking analgesia before exercises and physiotherapy. Adequate pain relief is also what makes early gentle motion possible. A regional nerve block is commonly used, explaining the early numbness that recovers over about a day.
Evidence: MODERATE (survey / practice data).
3. Early motion depends on the operation — accelerated for reverse, guarded for anatomic¶
The ward starts active hand/wrist/elbow motion immediately after every replacement. What the shoulder is allowed to do then splits by operation. For reverse replacement the conservative-versus-early question has been tested directly: randomised trials show that earlier motion and shorter (or even no) immobilisation do not increase dislocation or complications, including a 3-week-versus-no-immobilisation RCT in primary RSA [RAG corpus — 10.1016/j.jse.2025.02.015], and home-based physiotherapy matched formal outpatient therapy after RSA [RAG corpus — 10.1016/j.jse.2023.03.023]. Dr Hirpara's reverse pathway now follows this accelerated line: a short (~2-week) comfort sling, and active-assisted and active-as-tolerated shoulder motion (supine/gravity-assisted first) from the start, within comfort — with dislocation precautions (no arm behind the body, no lifting, no pushing through the hands) the main early constraint. By contrast, anatomic TSA and replacement for fracture keep the protective early line — passive/assisted elevation only, no active shoulder lifting, and the front-of-shoulder repair (or the tuberosities) guarded — because there is a repair that the reverse construct does not have.
Evidence: MODERATE–STRONG for RSA early motion (RCTs), which the reverse pathway now reflects; the specific in-hospital timings are consensus/surgeon preference.
4. Why external rotation is limited after anatomic TSA but freer after reverse¶
In anatomic TSA the subscapularis must be detached to seat the implant and then repaired, and external rotation (especially with the arm out to the side) puts the greatest strain on that repair — so early ER is restricted while forward elevation and scaption, which do not load the repair, are allowed sooner [literature — Brigham & Women's Faulkner TSA guideline; subscapularis management review]. Typical published protocols cap early external rotation at around 20–30° and release it at about 6 weeks; the synthesis applies this by moving the arm only from the sling position to "pointing straight ahead." After reverse replacement there is usually no subscapularis repair to protect, so ER is more permissive and the dominant precaution is instead the hand-behind-the-back dislocation position [parent reverse protocol — RAG corpus 10.1016/j.jse.2016.12.073; 10.1016/j.jse.2020.05.019].
Evidence: MODERATE (biomechanical + protocol consensus); no single defining rehab RCT for the early in-hospital window.
Phased timeline — the early phase only¶
This focuses on the in-hospital and immediately-post-discharge window. The complete multi-phase course (intermediate, transitional, advanced strengthening, return to sport) lives in each parent protocol; the rows below are intentionally consistent with the Phase I content of those pages.
| Phase | Window | Sling | Shoulder motion | Operation-specific note |
|---|---|---|---|---|
| In hospital | Days 0–2 | Reverse: comfort/support. Anatomic + fracture: worn incl. overnight | Active hand/wrist/elbow (all); pendulums. Reverse: active-assisted + active-as-tolerated from the start (supine/gravity-assisted first). Anatomic + fracture: passive/assisted elevation, limited assisted ER | Ward physio fits sling, teaches management, starts the synthesis exercises before discharge |
| Early protection | Weeks 0–3 | Reverse: ~2 weeks for comfort. Anatomic + fracture: full-time (worn overnight) | Reverse: continue active-assisted/active motion within comfort; dislocation precautions (no arm behind body, no lifting, no pushing through hands). Anatomic TSA: passive/assisted only, no active lifting, ER limited (sling-to-straight-ahead), IR delayed. Fracture: most protective | Pain + swelling control; keep adjacent joints moving |
After this early window, follow the full protocol for your specific operation (linked above), where the sling is weaned, active motion is progressed, and strengthening begins.
Key controversies / evidence quality¶
- Inpatient vs same-day discharge. Cohort evidence supports same-day discharge in selected patients, but selection matters and pain control is the limiting factor; whether you stay overnight is a clinical judgement, not a fixed rule. Moderate.
- How protective to be early. Randomised data (strongest for reverse) show early motion and shorter immobilisation are safe. The reverse pathway now applies this accelerated approach (short comfort sling, early active-assisted/active motion, dislocation precautions). The anatomic pathway stays protective because it has a subscapularis repair to guard — there the protective early phase is a deliberate surgeon clinical decision, not an oversight relative to the accelerated literature. Moderate–strong evidence; applied per operation.
- The in-hospital protocol itself is consensus/expert. The specific early exercises and ROM limits are drawn from published institutional protocols and surgeon guidance, not from a rehab RCT of the in-hospital window. Weak/consensus.
Evidence-strength flags (summary)¶
- MODERATE (cohort): short length of stay; same-day discharge non-inferior for readmissions and safe in selected and older patients; pain control as the primary patient concern.
- MODERATE–STRONG (RCT, mainly reverse): early motion / shorter immobilisation safe after RSA; home-based PT equivalent to formal outpatient PT after RSA.
- MODERATE (biomechanical + protocol consensus): ER restriction protects the subscapularis repair in anatomic TSA; reverse rehab more permissive in ER but constrained by the dislocation position.
- WEAK / CONSENSUS: the specific in-hospital exercise set and early-phase timings (institutional protocols + surgeon preference; no defining rehab RCT of the inpatient window).
Citations¶
RAG corpus (180,000+ Orthopaedic articles) — real DOIs returned by search¶
- Length of stay after shoulder arthroplasty — the effect of an orthopedic specialty hospital. J Shoulder Elbow Surg. 2016. DOI: 10.1016/j.jse.2016.01.010
- Same-day discharge is not inferior to longer length of in-hospital stay for 90-day readmissions following shoulder arthroplasty. J Shoulder Elbow Surg. 2020. DOI: 10.1016/j.jse.2019.09.037
- Outpatient total shoulder arthroplasty in an ambulatory surgery center is a safe alternative to inpatient total shoulder arthroplasty in a hospital: a matched cohort study (2016 Neer Award). J Shoulder Elbow Surg. 2016. DOI: 10.1016/j.jse.2016.07.011
- Is outpatient shoulder arthroplasty safe in patients aged ≥65 years? A comparison of readmissions and complications in inpatient and outpatient settings. J Shoulder Elbow Surg. 2021. DOI: 10.1016/j.jse.2021.02.022
- Perioperative pain control represents the primary concern for patients considering outpatient shoulder arthroplasty: a survey-based study. J Shoulder Elbow Surg. 2022. DOI: 10.1016/j.jse.2022.07.009
- Three-week immobilization vs. no immobilization in primary reverse total shoulder arthroplasty: a randomized controlled trial. J Shoulder Elbow Surg. 2025. DOI: 10.1016/j.jse.2025.02.015
- Home-based physical therapy results in similar outcomes to formal outpatient physical therapy after reverse total shoulder arthroplasty: a randomized controlled trial. J Shoulder Elbow Surg. 2023. DOI: 10.1016/j.jse.2023.03.023
- The American Society of Shoulder and Elbow Therapists' consensus statement on rehabilitation for anatomic total shoulder arthroplasty. J Shoulder Elbow Surg. 2020. DOI: 10.1016/j.jse.2020.05.019
- Dislocation following reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2017. DOI: 10.1016/j.jse.2016.12.073
Literature (URLs)¶
- The effect of subscapularis-specific rehabilitation following total shoulder arthroplasty: a prospective, double-blinded, randomized controlled trial. J Hand Ther / ScienceDirect. 2023. https://pubmed.ncbi.nlm.nih.gov/37263480/
- Management of the subscapularis tendon during total shoulder arthroplasty (early ER strains the repair most). J Hand Ther / ScienceDirect. 2016. https://www.sciencedirect.com/science/article/abs/pii/S1058274616305791
Published rehabilitation protocols (basis for the early-phase structure)¶
- Brigham & Women's Faulkner Hospital — Department of Rehabilitation Services: Total Shoulder Arthroplasty Guideline (early ER restriction to protect the subscapularis repair). https://www.brighamandwomensfaulkner.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/total-shoulder-arthroplasty-guideline.pdf
- Massachusetts General Brigham Sports Medicine — Rehabilitation Protocol for Total Shoulder Arthroplasty and Hemiarthroplasty (Revised December 2018). https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-total-shoulder-arthroplasty-and-hemi.pdf
- Massachusetts General Brigham Sports Medicine — Rehabilitation Protocol for Reverse Shoulder Arthroplasty (Revised December 2018). https://www.massgeneral.org/assets/mgh/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-reverse-shoulder-arthroplasty.pdf