Clinicians › Wrist
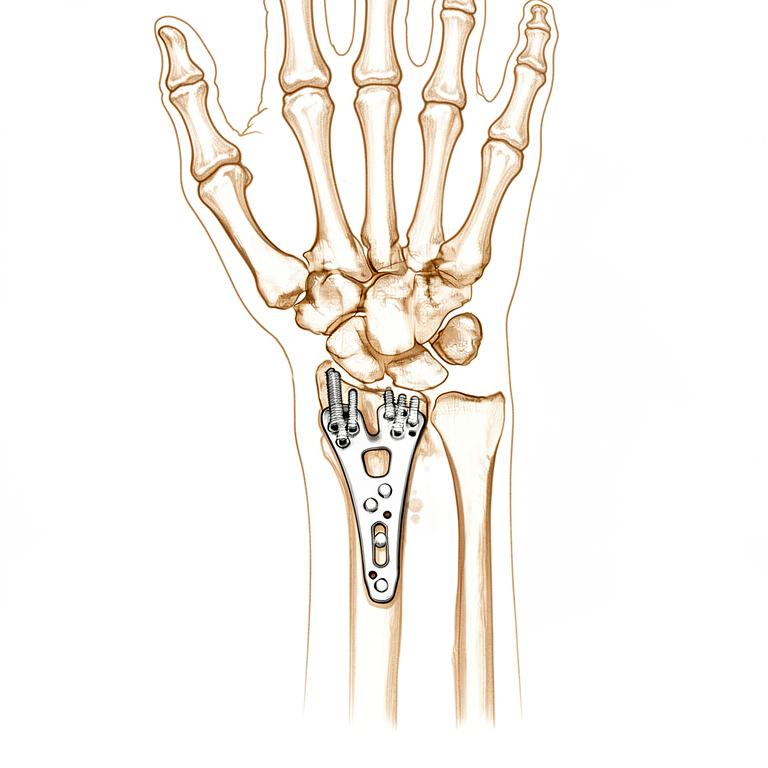
Distal Radius ORIF
Open reduction and volar plate fixation of the distal radius — operation, recovery, rehabilitation.
For patients: a plain-language version of this topic is available. See the patient guide.
Overview¶
Open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture regarding early and sustained functional recovery [5] and reduction in fracture healing complications [5]. Early mobilization for patients treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1], with mean differences in DASH scores at 6 weeks surpassing the minimal clinically important difference [1]. Radial column plating of the distal radius is a safe treatment modality [6] and a valuable adjunct in the setting of complex distal radius fractures [6], though there is a 28% chance that hardware removal may be required for patients undergoing this technique [6].
Treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9]. However, technical precision is critical; placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8]. While substantial variations in surgical direct costs for distal radius ORIF exist [2], implant choice is the predominant driver of this cost variation [2]. Additionally, the length of stay can be calculated for the Lift-Off Screw technique in a distal radius fracture model [3], and this technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft [3].
Anatomy & Pathophysiology¶
Osseous Architecture¶
Distal radius fractures represent the most common upper extremity fracture in the United States, affecting over 300,000 patients annually with a bimodal distribution driven by high-energy trauma in youth and low-energy falls in the elderly [27]. The distal radius articular surface is biconcave with distinct scaphoid and lunate facets, while the metaphysis features a thin cortex vulnerable to bending forces [27]. In a normal wrist with neutral ulnar variance, the distal radius bears 80% of the axial load [27]. Normal anatomical parameters include a radial height of 11 mm (accepting <5 mm shortening), radial inclination of 22 degrees (accepting <5-degree change), and volar tilt of 11 degrees (accepting <10-degree dorsal angulation) [27]. The brachioradialis insertion on the radial styloid acts as a deforming force in these fractures [27].
The carpus functions as a bridge between the forearm and hand, comprising two rows of eight bones [16]. The proximal row (scaphoid, lunate, triquetrum) serves as a key intercalated segment with no direct tendon attachments; its motion derives from bone shape, interaction, and ligamentous support [16]. The pisiform is excluded from this row as a sesamoid bone within the flexor carpi ulnaris sheath [16]. The distal row (trapezium, trapezoid, capitate, hamate) articulates proximally with the proximal row and distally with the metacarpals [16]. Specific articulations include the trapezium with the first metacarpal, trapezoid with the second, capitate with the third, and hamate with the fourth and fifth [16]. The capitate and trapezoid are tightly connected to the metacarpals, while the metacarpotrapezial joint allows 30 to 40 degrees of flexion–extension and rotation [16]. Motion of the distal row is controlled by extrinsic wrist flexors and extensors [16].
The scaphoid is an S-shaped tubular bone located on the radial aspect of the proximal row, lying at a 45-degree plane to the wrist axes [21]. It articulates with the radius, lunate, capitate, and trapezium/trapezoid [21]. The proximal articular surface is convex, while the distal surface features facets for the trapezium and trapezoid forming the scaphotrapeziotrapezoid (STT) joint [21]. The scaphoid gently pronates and flexes distally, positioning the distal pole ulnarly angulated relative to the proximal pole [21]. Over 80% of the scaphoid surface is covered with articular cartilage [21]. The scaphoid acts as a midcarpal bridge linking and synchronizing proximal and distal row motions [21].
Metacarpals form a Roman arch-like cascade where the index and small fingers are borders and the middle finger is the keystone [20]. The middle and ring fingers possess the most inherent stability due to central location, whereas border digits are prone to shortening, rotation, and angulation [20]. Metacarpal fractures are third in frequency only to phalangeal and distal radius fractures, with 70% occurring in the second and fifth decades [17]. The vast majority are inherently stable and treatable via closed means with early range of motion [17]. The metacarpal diaphysis has a tubular structure with thick cortices providing better fixation purchase than the thinner metaphyseal cortex [20]. The metacarpal head is cam-shaped in the sagittal plane and trapezoidal in the transverse plane, contributing to inherent stability during MCP flexion [20]. Collateral ligaments attach dorsally on the metacarpal head, elongating in flexion [20]. Metacarpal necks are susceptible to fracture during punching, and the fifth metacarpal has the most anterior–posterior arc at the CMC joint [20].
Ligamentous Stability¶
Wrist stability is predominantly maintained by extrinsic and intrinsic ligaments contained within the joint capsule [16]. Extrinsic palmar radiocarpal ligaments include the transverse carpal, radioscaphocapitate (RSC), radioscapholunate (RSL), radial collateral, long radiolunate (RLT), and short radiolunate ligaments [23]. Extrinsic ulnocarpal ligaments include the ulnotriquetral (dorsal and palmar), ulnolunate, and ulnocapitate ligaments [23]. Strong oblique extrinsic palmar radial ligaments prevent medial carpal translation on the angulated distal radius slope [23]. A V-shaped ligamentous band connects the forearm to the proximal row proximally and the distal row distally [23]. Between the radial and ulnar palmar ligaments lies the space of Poirier, a V-shaped interligamentous sulcus over the capitolunate articulation that is maximal in dorsiflexion [23]. The arcuate ligament, formed from interdigitation of the RSC, ulnocapitate, triquetrocapitate, and volar scaphotriquetral ligaments, forms a support sling for the midcarpal region and capitate head [23]. Extrinsic dorsal carpal ligaments include the dorsal radiocarpal (DRC) and dorsal intercarpal ligaments [23]. The ulnodorsal capsule is reinforced by the ulnolunate, ulnotriquetral ligaments, and floors of the fifth and sixth extensor compartments [23]. Some studies suggest an essential role for dorsal carpal ligaments in scapholunate stability [23].
Intrinsic ligaments connect individual carpal bones and include palmar midcarpal, proximal interosseous, and distal interosseous ligaments [23]. Ligaments associated with the pisiform include the pisotriquetral and pisohamate ligaments [23]. Apart from the scaphocapitate ligament, carpal ligaments are not described consistently across anatomical studies [16]. The radioscapocapitate ligament does not attach to the bone itself but crosses the scaphoid waist as a sling allowing rotation [21]. Ligamentous attachments of the scaphoid are predominantly found on the nonarticular dorsoradial surface, which also serves as the insertion for the dorsal component of the scapholunate and intercarpal ligaments [21]. There are no tendon attachments to the scaphoid [21].
Vascular Supply¶
The scaphoid has a reduced capacity for periosteal healing and an increased tendency for delayed union and nonunion [21]. Blood supply is provided by two vascular pedicles from the radial artery: the dorsal branch enters via foramina along the spiral groove and dorsal ridge to supply 70% to 80% of the scaphoid proximally, including the proximal pole [21]. The volar branch enters via the scaphoid tubercle to supply the remaining 20% to 30% of the distal scaphoid [21]. The scaphoid waist has minimal or no perforating vasculature, and no vessels perforate the proximal dorsal cartilaginous area or through the scapholunate ligament [21]. Proximal fractures are inexorably associated with at least temporary disruption of the interosseous blood supply to the proximal pole [21].
Kinematics and Pathophysiology¶
The distal radioulnar joint (DRUJ) is the articulation between the radius and ulna at the sigmoid notch [27]. Lister tubercle is a dorsal prominence serving as a landmark for the dorsal wrist approach and a cause of attritional rupture of the extensor pollicis longus (EPL) after distal radius fracture [27]. Radiocarpal dislocation or "inferior arc" injury is purely ligamentous or associated with styloid fracture, is highly unstable, and difficult to reduce closed [27]. DRUJ involvement is assessed on a true lateral radiograph for alignment [27]. Ligamentous injuries to consider include scapholunate (SL), lunotriquetral (LT), or triangular fibrocartilage complex (TFCC) injuries [27].
Surgical Approaches and Fixation¶
The flexor carpi radialis (FCR) approach provides excellent exposure for volar plating; incising the FCR sheath on its radial aspect may avoid injury to the palmar cutaneous branch of the median nerve [26]. After retracting the FPL tendon ulnarly, the pronator quadratus is elevated [26]. A brachioradialis tenotomy removes a deforming force [26]. Repair of the pronator quadratus did not result in better outcomes at 12 months in a randomized trial of 72 patients [26]. The extended FCR approach facilitates adequate distal exposure including the volar ulnar corner by biasing the skin incision midline to develop the interval between digital flexors and the ulnar neurovascular bundle [26]. Retracting carpal tunnel contents radially provides excellent visualization of the lunate facet fragment, an exposure that is extensile with an open carpal tunnel release [26]. A radial column approach requires protection of the superficial branch of the radial nerve and utilizes the deep interval through the first dorsal compartment or between the first and second compartments [26].
The dorsal approach is traditional for plating but enthusiasm waned due to extensor tendon complications [26]. It may be necessary to reduce and stabilize the dorsal ulnar facet fragment, with elevation of the fourth dorsal compartment on its ulnar aspect exposing the dorsal ulnar corner [26]. Unlike the volar approach, the dorsal approach affords visualization of the articular surface through a dorsal capsulotomy [26]. External fixation carries a pin tract infection rate exceeding 30%, though deep infection requiring removal occurs in less than 2% of cases [22]. Radial nerve injury occurs in 1% of external fixation cases [22]. Increased distraction leads to digit stiffness and CRPS risk, as excessive distraction decreases flexion ability [22]. Some level of distraction aids reduction via ligamentotaxis and carpal ligament tightening [22]. The large tenaculum clamp facilitates anatomical restoration of volar tilt and translation while allowing intraoperative fluoroscopy and potentially minimizing flexor tendon abrasion or rupture [36].
Imaging and Assessment¶
Computed tomography (CT) is used for detail of complex intraarticular patterns [27]. Magnetic resonance imaging (MRI) is used for occult fracture, bone contusion, and associated soft tissue injury [27]. Ulnar variance is assessed with the forearm in neutral rotation and compared with the contralateral side [27]. Malrotation can be difficult to assess in metacarpal fractures despite specific assessment methods [17].
Classification¶
Radial Column Plating: This modality is a safe treatment option and serves as a valuable adjunct for complex distal radius fractures [6]. However, there is a 28% chance that hardware removal may be required for patients undergoing this procedure [6].
Plate Positioning: In displaced intra-articular distal radius fractures, the treatment outcomes for dorsally versus volarly placed interlocking plate systems are similar [9]. Regarding screw placement in comminuted intra-articular fractures, positioning the distal row of screws greater than 3mm from subchondral bone is associated with increased odds of worsening ulnar variance [8].
Lift-Off Screw Technique: The length of stay (LOS) can be calculated for this technique in a distal radius fracture model [3]. This technique can potentially be utilized with any distal radius periarticular locking plate that includes locking options in the shaft [3].
Other Considerations: Open reduction and internal fixation with a plate provides the best results for adult patients regarding early and sustained functional recovery as well as a reduction in fracture healing complications [5]. Early mobilization for patients treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1]. Mean differences in DASH scores at 6 weeks for early mobilization surpass the minimal clinically important difference [1]. Substantial variations in surgical direct costs exist, with implant choice being the predominant driver of this cost variation [2].
Clinical Presentation¶
Early mobilization following open reduction and internal fixation (ORIF) of distal radius fractures yields beneficial functional effects at earlier stages compared to late mobilization [1]. Patients treated with early mobilization demonstrate mean differences in DASH scores at 6 weeks that surpass the minimal clinically important difference [1]. While implant choice is the predominant driver of substantial variations in surgical direct costs for distal radius ORIF, the specific technique of radial column plating remains a safe modality for complex fractures [2, 6].
Surgical Approach and Outcomes: Open reduction and internal fixation with a plate offers the best results for adult patients regarding early and sustained functional recovery and reduction in fracture healing complications [5]. The Lift-Off Screw technique can be utilized with any distal radius periarticular locking plate possessing locking options in the shaft to calculate length of stay and correct sagittal tilt [3]. Treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrates similar clinical results [9]. However, placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular fractures is associated with increased odds of worsening ulnar variance [8].
Galeazzi Fracture Patterns: Because the forearm functions as a ring, an isolated radial shaft fracture is uncommon in adults; fractures within 7.5 cm of the radiocarpal joint are more likely to represent a Galeazzi fracture [35]. Galeazzi fractures with rare exceptions require surgical fixation to restore the structural integrity of the forearm ring [35]. The goal of surgery is anatomic reduction of the radial shaft, especially the radial bow, and restoration of a stable distal radioulnar joint (DRUJ) [35]. Closed management of displaced forearm axis fractures in adults results in poor outcomes [35].
Physical Examination and Radiographic Assessment: Examination may reveal a prominent ulnar head in cases of dorsal DRUJ subluxation or dislocation [35]. Radiographic parameters associated with DRUJ injury include fracture of the base of the ulnar styloid, widening of the DRUJ on the AP wrist radiograph, dislocation of the ulna relative to the radius on a true lateral wrist radiograph, and more than 5 mm of shortening of the radius relative to the ulna (ulnar positive variance) when compared with the contralateral wrist [35]. Radial shaft fracture line obliquity greater than 30° is a statistically significant predictor of DRUJ instability [35].
Operative Management and Stability Testing: ORIF for Galeazzi fractures is typically performed through a volar Henry approach with a 3.5-mm dynamic compression plate, though a dorsal Thompson approach can be used for radial shaft fractures in the proximal third [35]. Intramedullary fixation is rarely used because it is difficult to restore the anatomic radial bow [35]. After fixation, the DRUJ is examined in full pronation and supination to assess stability [35]. If the ulna can be dislocated from the sigmoid notch with the forearm in supination, the DRUJ supporting ligaments including the triangular fibrocartilage complex (TFCC) are incompetent [35]. If the DRUJ is stable after translation or shuck stress testing, the extremity is immobilized in a long arm splint or cast in the position of greatest stability [35].
Stabilization Techniques and Complications: Stabilization of the DRUJ can be achieved by transradioulnar extra-articular Kirschner wires, which should protrude enough on the radial cortex so that if the wires break, the ends can be retrieved from both the radius and ulna without difficulty [35]. Displaced ulnar styloid fractures can be internally fixed with specialty plates, a tension band wire, or suture [35]. The DRUJ can also be stabilized by retensioning and reinsertion of the TFCC attachment with a suture anchor or transosseous suture [35]. Unreducible or complex ulnar head dislocations require arthrotomy to retrieve possible interposed extensor carpi ulnaris, extensor digitorum communis, or extensor digiti minimi tendons [35]. Other structures that can impede closed reduction include a metaphyseal fragment buttonholed through the capsule, the periosteum, or an avulsed styloid fracture fragment from the fovea [35]. After reduction and stabilization, the arm is immobilized in a long arm cast or splint for 4 to 6 weeks, and true lateral radiographs should document a reduced DRUJ [35].
Complications: Patients undergoing radial column plating should be counseled that there is a 28% chance that hardware removal may be required [6]. Complications following management of Galeazzi fractures include nonunion, malunion with limited forearm rotation, nerve or vessel injury, infection, complex regional pain syndrome, and persistent DRUJ instability [35].
Investigations¶
Plain radiography: Initial assessment of the wrist requires four standard views: posteroanterior with ulnar deviation, lateral, semi-pronated oblique, and semi-supinated oblique [24]. An anteroposterior view with a clenched fist is added if scapholunate injury is suspected [24]. In the lateral view, the axes of the radius, lunate, capitate, and third metacarpal must be co-linear, while the scaphoid projects at approximately 45 degrees to the radius [24]. Dorsal intercalated segmental instability (DISI) is characterized by dorsal tilting of the lunate and volar tilting of the scaphoid, whereas volar intercalated segmental instability (VISI) involves volar tilting of both bones [24]. For suspected scaphoid fractures, AP, lateral, and two oblique views are standard, though 10 to 15% of these fractures are not visible on initial X-rays [24]. In cases of ulnar translation, radiographs may show the lunate positioned just distal to the ulna with a large space between the radial styloid and scaphoid [25]. Standard scaphoid views detect most carpal injuries, but perilunate dislocations can be missed; assessment of Gilula's lines aids in diagnosing these dislocations [31]. Multiple views and repeated examinations may be necessary to detect undisplaced cracks [24].
MRI: MRI is the definitive method to confirm or exclude a scaphoid fracture diagnosis when available and reduces uncertainty in suspected cases [24][30]. It is also useful for detecting suspected fractures, avascular necrosis (AVN) of the carpus, and determining the extent of ligamentous disruption in radiocarpal instability [25][31].
CT: CT is more sensitive than X-rays for diagnosing scaphoid fractures and is required to better define associated bony injuries in radiocarpal instability [25][30]. Two-dimensional and three-dimensional CT are used to assess suspected carpal fractures, fracture displacement, malunion, nonunion, and bone loss [31]. CT is also useful for assessing union in suspected carpal fractures [31].
Bone scan: Bone scintigraphy is utilized for suspected carpal fractures and avulsion injuries [31].
Other Considerations: Assessment of metacarpal fractures requires evaluation of skin integrity, neurovascular status, ligamentous evaluation, tendon function, and malrotation [17]. The incidence of metacarpal fractures is third only to phalangeal and distal radius fractures in the upper limb, with approximately 70% occurring in the second and fifth decades [17]. The vast majority of metacarpal fractures are inherently stable and treated via closed means with early range of motion [17]. Understanding the anatomy of the eight carpal bones is essential for diagnosis; the proximal row (scaphoid, lunate, triquetrum) serves as a key intercalated segment, while the distal row includes the trapezium, trapezoid, capitate, and hamate [16]. Inherent stability is provided by extrinsic and intrinsic ligaments reinforcing the carpal capsule, though carpal ligaments (except the scaphocapitate) are not described consistently across studies [16]. Scaphoid fractures account for almost 75% of all carpal fractures but are rare in children and the elderly [30]. The usual mechanism is forced hyperextension, with fractures occurring at the distal tubercle, waist, or proximal pole [30]. The blood supply arises from the dorsal distal pole, making the proximal pole less likely to heal due to poor vascularity [30]. Some scaphoid fractures, particularly distal oblique and waist types, are unstable and predispose to non-union or malunion [30]. Diagnostic signs include precisely localized tenderness in the anatomical snuffbox, pressure over the scaphoid tubercle, palpation of the proximal pole, and telescoping of the thumb base [30]. If X-rays are normal but clinical features suggest a fracture, the patient must be immobilized and not discharged [30]. Secondary imaging modalities, including ultrasound, dynamic CT, arthrography, and wrist arthroscopy, are predominantly used for assessing intercarpal ligament injury and instability [31]. Ultrasound provides an additional tool for detecting carpal ligament injuries [31]. Dynamic CT is used by some for ligament injuries [31]. Arthrography ± videofluoroscopy is used for ligament injuries [31]. Wrist arthroscopy aids in diagnosing ligament injuries and fracture displacement [31]. Live/video fluoroscopic evaluation provides diagnostic clarity for dynamic instability with sensitivities between 86% and 95% and specificity between 80% and 97% for scapholunate ligament injury [31]. Radiographic measurements include the lateral intrascaphoid angle (cut-off >35 degrees for displacement), AP intrascaphoid angle, dorsal cortical angle (abnormal if >160 degrees), and scaphoid height-to-length ratio (abnormal if >0.65) [31]. The DISI pattern is most commonly associated with displaced scaphoid fractures and scapholunate dissociation [31]. A cortical ring sign with the wrist in flexion, pronation, and ulnar deviation helps localize the ulnar aspect of the proximal pole of the scaphoid [32]. For scaphoid fixation, a stab or mini-open incision avoids soft tissue injury; the wire is pulled distally from the palmar side until the proximal guidewire clears the radiocarpal joint, then advanced retrograde to exit dorsally [32]. Screw length must be measured carefully with several millimeters subtracted to avoid prominence, and larger screws are biomechanically stronger [32]. Cannulated screws improve central placement compared with Herbert screws [32]. In the context of proximal humerus fractures, patients with glenoid vault CT Hounsfield units less than 160 HU have a significantly increased risk of ORIF failure [38].
Treatment¶
Operative¶
Indications: Open reduction and internal fixation with a plate is the recommended option for adult patients with distal radius fractures, offering the best results for early and sustained functional recovery as well as a reduction in fracture healing complications [5]. For elderly patients aged 70 years or older with extra-articular distal humeral fractures, open reduction and internal fixation is indicated when conservative treatment has failed [19]. Radial column plating of the distal radius serves as a safe treatment modality and a valuable adjunct in the setting of complex distal radius fractures [6].
Surgical Approach / Technique: Early mobilization for patients treated with ORIF may have a beneficial effect on function at earlier stages compared to late mobilization [1]. Mean differences in DASH scores at 6 weeks for early mobilization surpass the minimal clinically important difference [1]. The Lift-Off Screw technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft, and the length of stay for this technique can be calculated within a distal radius fracture model [3]. In comminuted intra-articular distal radius fractures, placing the distal row of screws greater than 3mm from subchondral bone was associated with increased odds of worsening ulnar variance [8]. The treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results [9].
Implant Selection: Implant choice is the predominant driver of cost variation for distal radius ORIF, contributing to substantial variations in surgical direct costs [2]. Hardware removal may be required in 28% of patients undergoing radial column plating of the distal radius [6]. In the specific case of proximal plate migration after internal fixation of a pediatric distal radius fracture, the patient required washout and hardware removal, resulting in resolution of symptoms [40].
Complications¶
Stiffness / Arthrofibrosis: Early mobilization following ORIF may yield beneficial functional outcomes at earlier stages compared to late mobilization, with mean differences in DASH scores at 6 weeks surpassing the minimal clinically important difference [1].
Hardware Removal: Radial column plating is a safe treatment modality, though patients should be counseled regarding a 28% chance that hardware removal may be required [6].
Other Considerations: Open reduction and internal fixation with a plate offers the best results for adult patients regarding early and sustained functional recovery and a reduction in fracture healing complications [5]. Treatment of displaced intra-articular fractures with dorsally versus volarly placed interlocking plate systems demonstrates similar clinical results [9]. A low overall complication rate of 12.3% was observed in volar locking plate fixation, comprising 4.8% major and 7.5% minor complications [39]. Substantial variations in surgical direct costs exist, with implant choice serving as the predominant driver [2]. The length of stay can be calculated, and the lift-off screw technique can potentially be used with any distal radius periarticular locking plate possessing locking options in the shaft [3]. In comminuted intra-articular fractures, placing the distal row of screws greater than 3mm from subchondral bone is associated with increased odds of worsening ulnar variance [8].
Recovery¶
Light activity (weeks): Early mobilization is recommended for patients undergoing open reduction and internal fixation (ORIF) to optimize function at earlier stages compared to late mobilization [1]. This approach yields mean differences in DASH scores at 6 weeks that surpass the minimal clinically important difference [1].
Full activity (months): Open reduction and internal fixation with a plate provides the best results for adult patients regarding early and sustained functional recovery [5]. Radial column plating is a safe treatment modality and a valuable adjunct in the setting of complex distal radius fractures [6].
Complete recovery / outcome plateau (months): While functional recovery is optimized with plating, the trajectory may be influenced by technical factors; placing the distal row of screws greater than 3mm from subchondral bone in comminuted intra-articular distal radius fractures was associated with increased odds of worsening ulnar variance [8].
Rehabilitation protocol: The evidence supports early mobilization protocols to enhance early functional outcomes [1]. Surgeons should be aware that there is a 28% chance that hardware removal may be required for patients undergoing radial column plating of the distal radius [6].
Functional milestones: Validated outcome measures indicate that early mobilization leads to DASH score improvements at 6 weeks exceeding the minimal clinically important difference [1]. Open reduction and internal fixation with a plate offers the best results for adult patients in terms of reduction in fracture healing complications [5].
Other Considerations: Substantial variations in surgical direct costs for distal radius ORIF exist, with implant choice identified as the predominant driver of this cost variation [2].
Key Evidence¶
- [L1] Functionally, at earlier stages, early mobilization for patients with distal radius fractures treated with ORIF may have a beneficial effect compared to late mobilization, with mean differences in DASH scores at 6 weeks surpassing the minimal clinically important difference. [1] (10.1186/s13018-021-02837-0)
- [L3] Substantial variations in surgical direct costs for distal radius ORIF exist, and implant choice is the predominant driver. [2] (10.1016/j.jhsa.2018.04.015)
- [L5] The LOS length can be calculated, and this technique can potentially be used with any distal radius periarticular locking plate with locking options in the shaft. [3] (10.1016/j.jhsa.2018.02.011)
- [L1] A network meta-analysis of randomized trials revealed that open reduction and internal fixation with a plate offers the best results for adult patients with a distal radius fracture, in terms of early and sustained functional recovery and a reduction in fracture healing complications. [5] (10.5435/jaaos-d-18-00424)
- [L4] Radial column plating of the distal radius is a safe treatment modality and a valuable adjunct in the setting of complex distal radius fractures, but patients should be counseled that there is a 28% chance that hardware removal may be required. [6] (10.1177/1558944718760861)
- [L4] In this two-center retrospective cohort of comminuted intra-articular distal radius fractures, placing the distal row of screws greater than 3mm from subchondral bone was associated with increased odds of worsening ulnar variance. [8] (10.1016/j.jhsa.2025.03.016)
- [L3] The treatment of displaced intra-articular distal radius fractures with a dorsally versus a volarly placed interlocking plate system demonstrated similar clinical results. [9] (10.1177/1558944716675129)
- [L4] Osteosynthesis by open reduction and internal fixation is a recommended option for extra-articular distal humeral fractures in elderly patients aged 70 years or older in whom conservative treatment has failed. [19] (10.1016/j.jse.2017.08.024)
- [L4] The large tenaculum clamp facilitates anatomical restoration of volar tilt and volar translation while allowing intraoperative fluoroscopy, potentially minimizing complications such as flexor tendon abrasion or rupture. [36] (10.1016/j.jhsa.2018.11.017)
- [L3] Patients with computed tomography Hounsfield units (CTHU) of the glenoid vault < 160 HU who sustain a proximal humerus fracture have a significantly increased risk of ORIF failure, necessitating subsequent revision to arthroplasty. [38] (10.1016/j.jse.2025.09.008)
- [L4] A low overall complication rate of 12.3% was found, with 4.8% major and 7.5% minor complications. [39] (10.1016/j.jhsa.2022.11.012)
- [L4] The patient required washout and hardware removal, with resolution of his symptoms. [40] (10.1177/15589447221130083)
See Also¶
References¶
[1] In adults, early mobilization may be beneficial for distal radius fractures treated with open reduction and internal fixation: a systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research. 2021. DOI: 10.1186/s13018-021-02837-0
[2] Evaluation of Factors Driving Cost Variation for Distal Radius Fracture Open Reduction Internal Fixation. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2018.04.015
[3] Lift-Off Screw Results in Accurate Sagittal Tilt Correction in a Distal Radius Fracture Model. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2018.02.011
[5] Interventions for Distal Radius Fractures: A Network Meta-analysis of Randomized Trials. Journal of the American Academy of Orthopaedic Surgeons. 2019. DOI: 10.5435/jaaos-d-18-00424
[6] Complications of Radial Column Plating of the Distal Radius. HAND. 2018. DOI: 10.1177/1558944718760861
[8] The Association Between Distal Screw and Articular Subsidence in the Open Treatment of Intra-articular Distal Radius Fractures. The Journal of Hand Surgery. 2026. DOI: 10.1016/j.jhsa.2025.03.016
[9] Management of Intra-Articular Distal Radius Fractures: Volar or Dorsal Locking Plate—Which Has Fewer Complications?. HAND. 2016. DOI: 10.1177/1558944716675129
[16] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Pathoanatomy and Applied Anatomy Relating to Carpal Fractures and Dislocations.
[17] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Metacarpal Fractures.
[19] Open reduction and internal fixation for nonunion of extra-articular distal humeral fractures in patients 70 years and older. Journal of Shoulder and Elbow Surgery. 2018. DOI: 10.1016/j.jse.2017.08.024
[20] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Pathoanatomy and Applied Anatomy Relating to Metacarpal Fractures.
[21] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Pathoanatomy and Applied Anatomy Related to Scaphoid Fractures.
[22] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > External Fixation of the Distal Radius: Preoperative Checklist > Bridging External Fixation of the Distal Radius: Key Surgical Steps.
[23] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Extrinsic Ligaments.
[24] Apley And Solomon S Concise System Of Orthopaedics And Trauma. FRACTURES OF THE DISTAL RADIUS IN CHILDREN > Imaging.
[25] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Assessment of Radiocarpal Instability.
[26] Orthopaedic Knowledge Update Trauma. Fractures of the Forearm and Distal Radius > Surgical Approaches.
[27] Miller S Review Of Orthopaedics. SECTION 16 PATELLAR TRACKING IN TOTAL KNEE ARTHROPLASTY > DISTAL RADIUS FRACTURES.
[28] Miller S Review Of Orthopaedics. DISTAL RADIUS FRACTURES.
[30] Apley And Solomon S Concise System Of Orthopaedics And Trauma. FRACTURES OF THE DISTAL RADIUS IN CHILDREN > FRACTURE OF THE SCAPHOID.
[31] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Secondary Imaging Methods.
[32] Rockwood And Green S Fractures In Adults. 42: Fractures of the Distal Radius and Ulna > Dorsal Approach.
[35] Orthopaedic Knowledge Update Trauma. Fractures of the Forearm and Distal Radius > Forearm Fractures > Galeazzi Fractures.
[36] Use of a Large Tenaculum Clamp as a Reduction Technique for Treatment of Distal Radius Fractures. The Journal of Hand Surgery. 2019. DOI: 10.1016/j.jhsa.2018.11.017
[38] Low glenoid vault bone density is a risk factor for failure of proximal humerus fracture fixation. Journal of Shoulder and Elbow Surgery. 2026. DOI: 10.1016/j.jse.2025.09.008
[39] Complications After Volar Locking Plate Fixation of Distal Radius Fractures: A Retrospective Study of 822 Patients. The Journal of Hand Surgery. 2024. DOI: 10.1016/j.jhsa.2022.11.012
[40] Proximal Plate Migration After Internal Fixation of a Pediatric Distal Radius Fracture. HAND. 2023. DOI: 10.1177/15589447221130083