Patients › Rehabilitation
Thay khớp ngón tay (PIP)
Kế hoạch phục hồi được bảo vệ sau khi thay thế khớp giữa của ngón tay bị mòn (khớp PIP) bằng silicone, trong đó tốc độ bắt đầu vận động phụ thuộc vào việc bác sĩ phẫu thuật tiếp cận từ phía trước (mặt lòng bàn tay) hay phía sau của ngón tay.
Hướng dẫn này hỗ trợ quá trình hồi phục của bạn sau khi thay thế khớp giữa bị mòn của một ngón tay (khớp liên đốt gần (PIP), khớp giữa) bằng một miếng đệm silicone linh hoạt, do Bác sĩ Kieran Hirpara thực hiện tại Bệnh viện Tư nhân Mater Rockhampton. Hướng dẫn bắt đầu bằng chương trình bài tập tại nhà của bạn, tiếp theo là phác đồ lâm sàng có cấu trúc dành cho chuyên lý trị liệu bàn tay của bạn. Hãy mang theo trang này hoặc file PDF của nó đến buổi trị liệu đầu tiên để quá trình phục hồi chức năng được phối hợp nhịp nhàng. Chuyên gia trị liệu của bạn có thể điều chỉnh kế hoạch tùy thuộc vào tiến trình hồi phục của bạn.
Nếu bạn có bất kỳ lo ngại nào về vết mổ sau phẫu thuật, hãy liên hệ với phòng khám. Việc chụp ảnh vết mổ và gửi qua email để xem xét thường rất hữu ích.
Những điều cần biết¶
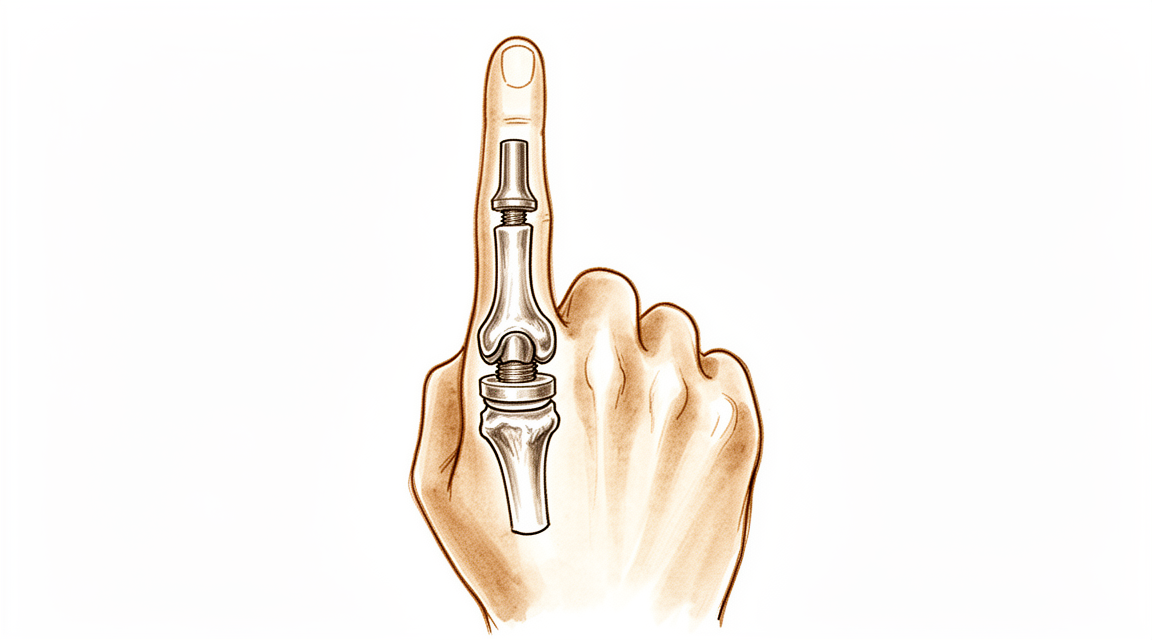
Khớp giữa của ngón tay bạn đã bị mòn do viêm xương khớp, gây đau và cứng. Trong ca phẫu thuật này, các bề mặt khớp bị mòn được loại bỏ và một khoảng cách bằng silicone linh hoạt (cấy ghép loại Swanson) được đặt giữa hai xương. Khoảng cách này không phải là một khớp bản lề cơ học cứng; nó là một khoảng cách linh hoạt giữ cho các xương tách rời, cho phép ngón tay uốn cong và để mô sẹo của chính bạn hình thành một lớp bao hỗ trợ mới xung quanh nó. Lợi ích chính và đáng tin cậy nhất là giảm đau. Bạn cũng nên mong đợi một cung uốn cong hữu ích, ở mức độ vừa phải (thường khoảng 40 đến 60 độ) thay vì phạm vi chuyển động hoàn toàn bình thường. Hầu hết mọi người đều rất hài lòng vì cơn đau đã biến mất và ngón tay trở nên thoải mái khi sử dụng.
Điều quan trọng nhất về quá trình hồi phục của bạn là đường rạch phẫu thuật của bác sĩ, vì điều đó quyết định thời điểm bạn có thể bắt đầu vận động:
- Từ phía trước (mặt lòng bàn tay, tiếp cận lòng bàn tay): gân duỗi ở mặt sau của ngón tay được giữ nguyên vẹn. Vì không có gì ở mặt sau phải lành lại, bạn thường có thể bắt đầu vận động ngón tay trong vòng vài ngày.
- Từ phía sau (tiếp cận lưng): gân duỗi (chấn thương lớp trung tâm) phải được rạch hoặc nâng lên để tiếp cận khớp, sau đó được sửa chữa. Vết sửa chữa này phải được bảo vệ trước tiên, vì vậy ngón tay được nẹp thẳng ngay từ đầu và việc uốn cong được đưa vào dần dần hơn, dưới sự hướng dẫn của chuyên viên trị liệu tay của bạn.
Chuyên viên trị liệu tay của bạn sẽ tuân theo kế hoạch dựa trên đường rạch phẫu thuật của bạn. Bác sĩ Hirpara sẽ thông báo cho họ đường rạch nào đã được sử dụng, và các thời điểm dưới đây được điều chỉnh phù hợp với nó. Bất kể bạn có đường rạch nào, khớp mới là một khớp bản lề: nó thích uốn cong và duỗi thẳng theo một đường thẳng, nhưng nó không thích bị đẩy hoặc xoắn sang bên. Bảo vệ nó khỏi căng thẳng sang ngang là cách duy trì sự ổn định lâu dài cho nó.
Các biện pháp phòng ngừa và hạn chế¶
- Chỉ cử động ngón tay theo đường thẳng (gập và duỗi) và tránh mọi lực ngang hoặc xoắn lên ngón tay đã phẫu thuật. Khớp mới là khớp bản lề và lực bên có thể làm lỏng hoặc biến dạng nó.
- Đeo nẹp theo chỉ định và sử dụng dán cố định ngón tay khi hoạt động để giữ cho ngón tay di chuyển thẳng.
- Nếu phẫu thuật của bạn ở mặt sau ngón tay, KHÔNG ĐƯỢC tự ý duỗi ngón tay vượt quá giới hạn được hướng dẫn trong giai đoạn đầu: gân duỗi đang trong quá trình lành.
- KHÔNG ĐƯỢC thực hiện các động tác nắm chặt, bóp mạnh hoặc các nhiệm vụ nặng hoặc có lực xoắn cho đến khi chuyên viên trị liệu tay cho phép tăng cường sức mạnh (thường là từ khoảng sáu tuần).
- Duy trì cử động các khớp ngón tay còn lại, cổ tay và vai ngay từ đầu, và sử dụng tay cho các nhiệm vụ nhẹ nhàng hàng ngày trong phạm vi chịu đựng được.
Để quản lý vết mổ, sưng và sẹo, xem hướng dẫn chăm sóc vết mổ của phòng khám.
Các bài tập của bạn¶
Đây là các bài tập từ tài liệu hướng dẫn của bạn. Chỉ bắt đầu thực hiện chúng theo sự hướng dẫn của Bác sĩ Hirpara và nhà trị liệu tay của bạn, duy trì trong phạm vi và giới hạn đã được chỉ định. Giai đoạn đầu giúp ngón tay vận động theo đường thẳng mà không chịu lực bên: uốn cong được bảo vệ, duỗi nhẹ, buộc ngón tay với nhau (buddy strapping) và trượt gân. Nếu phẫu thuật của bạn được thực hiện ở mặt sau của ngón tay, bài tập duỗi chủ động là bài tập cần được bảo vệ sớm và tăng dần dần. Bài tập tăng cường lực nắm thuộc về giai đoạn sau và không nên bắt đầu cho đến khi bạn được bác sĩ cho phép cụ thể. Ngừng bất kỳ hoạt động nào gây đau nhói hoặc khiến ngón tay cảm thấy không ổn định.
Giao thức lâm sàng của bạn¶
Phần còn lại của trang này là giao thức lâm sàng theo từng giai đoạn để phục hồi chức năng sau phẫu thuật thay khớp ngón tay (PIP) bằng implant silicone. Phần này sẽ được cung cấp cho nhà trị liệu bàn tay của bạn, và mỗi giai đoạn bắt đầu bằng một giải thích bằng tiếng Anh đơn giản về những gì đang diễn ra. Giao thức phụ thuộc vào phương pháp tiếp cận, và đây là điểm rẽ nhánh trung tâm: một phương pháp tiếp cận lòng bàn tay (volar) giữ nguyên cơ chế duỗi và cho phép vận động chủ động sớm trong vòng vài ngày; trong khi đó, một phương pháp tiếp cận mu bàn tay (dorsal) sẽ cắt hoặc tách gân duỗi trung tâm, do đó việc lành gân duỗi phải được bảo vệ trước tiên bằng nẹp duỗi và vận động uốn cong dần dần. Trong suốt quá trình, implant silicone là một khoảng cách linh hoạt, sự ổn định lâu dài của nó phụ thuộc vào bao quanh implant, vì vậy ứng lực theo mặt phẳng冠状 (lateral) được tránh và vận động được duy trì trong một cung thuần túy theo mặt phẳng sagittal.
Trước khi điều trị, hãy xác nhận với bác sĩ phẫu thuật điều trị về phương pháp tiếp cận phẫu thuật (lòng bàn tay so với mu bàn tay), tình trạng/sửa chữa của gân duỗi trung tâm và dây chằng bên, cũng như bất kỳ cung vận động nào trong quá trình phẫu thuật. Bác sĩ Hirpara sẽ chỉ định phương pháp tiếp cận; hãy chọn đường đi vận động chủ động sớm (lòng bàn tay) hoặc bảo vệ duỗi (mu bàn tay) tương ứng. Mục tiêu chức năng dự kiến là một cung vận động không đau khoảng 40–60°, không phải toàn bộ phạm vi vận động.
Giai đoạn I — bảo vệ và khởi động vận động (tuần 0 đến 3)¶
Những tuần đầu tiên nhằm bảo vệ các mô mềm trong khi ngăn ngừa cứng khớp, với tốc độ phục hồi hoàn toàn phụ thuộc vào phương pháp phẫu thuật. Cấy ghép ổn định trong các chuyển động gập–duỗi nhưng dễ bị tổn thương do tải trọng bên, do đó mọi chuyển động đều được duy trì trong mặt phẳng sagittal thuần túy và ngón tay được hỗ trợ bằng băng dính kèm ngón bên cạnh (buddy strapping) và nẹp.
Đối với chuyên viên trị liệu tay của bạn:
Giáo dục và các biện pháp phòng ngừa - Xác định phương pháp phẫu thuật và tuân theo lộ trình tương ứng: - Phương pháp qua lòng bàn tay (Volar approach): cơ chế duỗi còn nguyên vẹn → bắt đầu vận động chủ động khớp PIP/DIP từ ngày thứ 3–5. Đeo nẹp chặn duỗi/lò xo dạng volar cho phép cung gập ngắn (thường ban đầu khoảng ~30°), tăng dần theo thời gian. - Phương pháp qua mu bàn tay (Dorsal approach) (chẻ/sửa chữa gân duỗi trung tâm): bảo vệ duỗi. PIP được nẹp ở tư thế duỗi gần như tối đa suốt ngày đêm; đưa vào vận động chủ động gập trong cung ngắn hạn chế dưới sự giám sát, tôn trọng vết sửa chữa gân duỗi trung tâm. (Có thể sử dụng sơ đồ vận động tương đối/duỗi động lực theo sở thích của bác sĩ phẫu thuật.) - Tuyệt đối tránh ứng suất theo mặt phẳng coronal (bên/bán kính–cánh tay trụ) lên khớp phẫu thuật: dùng băng dính kèm ngón bên cạnh để hướng dẫn chuyển động thuần túy theo mặt phẳng sagittal. - Không cầm nắm, bóp hoặc sử dụng có kháng cự/tải trọng.
Quản lý điều trị - Vết mổ: băng phẫu thuật theo chỉ định; theo dõi nhiễm trùng - Phù nề: kê cao, mát-xa nhẹ nhàng theo hướng ngược dòng, băng ép nhẹ - Bài tập: vận động chủ động gập–duỗi khớp PIP/DIP được bảo vệ trong cung đã quy định; trượt gân; vận động chủ động các khớp không liên quan (DIP, MCP, cổ tay, ngón cái); bắt đầu dùng băng dính kèm ngón bên cạnh khi vận động - Đeo nẹp suốt ngày đêm giữa các buổi tập
Tiêu chí để chuyển giai đoạn - Vết mổ lành tốt; không xuất hiện lag duỗi (đối với lộ trình qua mu bàn tay); vận động thoải mái, kiểm soát được trong cung hiện tại
Giai đoạn II — tăng cường vận động (tuần 3 đến 6)¶
Cung vận động gập được mở rộng và, đối với các ngón tiếp cận từ phía sau, việc bảo vệ duỗi được nới lỏng dần dần khi gân trung tâm (central slip) lành vững. Mục tiêu của giai đoạn này là đạt được cung vận động hữu ích (≈40–60°) trước khi sự hình thành sẹo cố định phạm vi vận động.
Đối với nhà trị liệu tay của bạn:
Đánh giá - Cung vận động gập chủ động và bị động của khớp PIP; độ trễ duỗi (đường đi phía sau); ổn định mặt phẳng冠状; đau và phù nề; xem xét vết thương/vết sẹo
Giáo dục và các biện pháp phòng ngừa - Dần dần tăng cung vận động gập được phép hướng tới mục tiêu chức năng (≈40–60°) - Bụng (Volar): thúc đẩy gập chủ động khi bệnh nhân dung nạp được; thêm gập bị động nhẹ nếu duỗi hoàn toàn và ổn định - Sau (Dorsal): giảm dần đeo nẹp duỗi theo quá trình lành của gân trung tâm (thường giảm hỗ trợ ban ngày trong các tuần 4–6); đề phòng độ trễ duỗi: không theo đuổi gập bằng cách hy duỗi chủ động - Tiếp tục tránh tuyệt đối tải trọng bên/xoắn; chưa tập tăng sức đề kháng
Quản lý - Bài tập: gập–duỗi PIP chủ động và chủ động hỗ trợ theo mức độ; bài tập chặn để tập trung vào vận động PIP; tiếp tục trượt gân và băng ngón bạn bè; bắt đầu xoa sẹo khi vết thương đã lành - Duy trì vận động đầy đủ của các khớp lân cận
Tiêu chí để chuyển giai đoạn - Vết thương đã lành; khớp ổn định ở mặt phẳng冠状; cung vận động không đau đạt được chức năng; độ trễ duỗi tối thiểu (phía sau)
Giai đoạn III — tăng cường và trở lại (từ tuần 6 đến 12 và xa hơn)¶
Khi tầm vận động đã được thiết lập và các mô mềm ổn định (khoảng sáu tuần), việc tăng cường sức mạnh nhẹ bắt đầu và được xây dựng dần dần. Việc tăng cường sức mạnh được duy trì theo hướng trục (nắm chặt và tải trọng đường thẳng) trong khi vẫn tôn trọng các ứng suất bên/xoắn lên implant về lâu dài.
Đối với nhà trị liệu tay của bạn:
Đánh giá - Nắm chặt và bóp so với bên đối diện; cung khớp PIP cuối cùng; ổn định mặt phẳng coronal; kiểm tra chức năng và theo nhiệm vụ cụ thể
Giáo dục và các biện pháp phòng ngừa - Bắt đầu tăng cường sức mạnh nắm chặt nhẹ từ khoảng sáu tuần, xây dựng dần dần - Giới thiệu tải trọng bóp một cách thận trọng và tiếp tục tránh các tải trọng bên/xoắn mạnh lên khớp đã phẫu thuật mãi mãi (để kéo dài tuổi thọ của implant) - Đặt ra kỳ vọng thực tế: giảm đau bền vững là lợi ích chính; cung cuối cùng là khiêm tốn (≈40–60°) và chủ yếu được thiết lập vào khoảng 3 tháng
Quản lý - Bài tập: tăng dần cường độ nắm chặt/làm việc với bột tập; tải trọng chức năng và theo công việc được phân cấp; tiếp tục bất kỳ công việc nào còn sót lại về khả năng vận động và sẹo - Cân nhắc xuất viện khi một ngón tay ổn định, thoải mái, có chức năng với một cung không đau hữu ích đã đạt được - Chuyển lại cho bác sĩ điều trị nếu quá trình phục hồi bị đình trệ, khớp trở nên không ổn định/lệch, hoặc nghi ngờ hỏng implant
Tiêu chuẩn xuất viện / trở lại - Khớp thoải mái, không đau, ổn định mặt phẳng coronal với một cung chức năng; lực nắm đủ; có thể đáp ứng các yêu cầu hàng ngày và công việc
Trở lại làm việc và hoạt động¶
Việc sử dụng tay nhẹ nhàng trong sinh hoạt hàng ngày (ăn uống, viết lách, tự chăm sóc bản thân ở mức độ nhẹ) được khuyến khích ngay từ đầu, trong phạm vi cảm thấy thoải mái, miễn là ngón tay vẫn giữ ở tư thế thẳng và tránh các lực đẩy sang hai bên hoặc xoắn lên ngón tay đã phẫu thuật. Bạn thường có thể lái xe khi có thể nắm chặt vô lăng một cách thoải mái và kiểm soát xe an toàn, đã tháo nẹp cố định hạn chế vận động, và không còn sử dụng các loại thuốc giảm đau mạnh, thường là sau khoảng hai tuần, và điều này được xác nhận tại buổi tái khám.
Các động tác nắm chặt hơn và các nhiệm vụ chịu tải phải chờ đến khoảng sáu tuần, sau đó được tăng dần. Công việc nặng hoặc có động tác xoắn là những hoạt động cuối cùng được quay trở lại, và phụ thuộc vào việc ngón tay đạt được sự thoải mái, ổn định cùng lực nắm đủ mạnh, được đánh giá bởi Bác sĩ Hirpara và chuyên trị liệu tay của bạn, chứ không chỉ dựa trên thời gian. Hãy nhớ rằng kết quả lâu dài của ca phẫu thuật này là: giảm đau đáng tin cậy và một cung vận động hữu ích khoảng 40 đến 60 độ, đồng thời tránh các lực căng sang hai bên lên khớp về lâu dài để bảo vệ implant (cấy ghép).
Sau khi hoàn thành phác đồ¶
Phác đồ này được thực hiện song song với các lời khuyên chung về phục hồi chức năng của phòng khám; xem quản lý đau sau phẫu thuật, chăm sóc vết thương và quản lý sẹo. Kế hoạch theo từng giai đoạn nêu trên phản ánh các hướng dẫn phục hồi chức năng đã được công bố sau khi phẫu thuật thay khớp đốt sống giữa ngón tay bằng silicone PIP, và quá trình phục hồi tiếp theo của bạn sẽ được Dr Hirpara và chuyên viên trị liệu tay của bạn hướng dẫn cá nhân hóa dựa trên phương pháp phẫu thuật đã được sử dụng và tiến triển của ngón tay bạn.
Evidence & references
Silicone PIP Joint Replacement — Procedure Outcomes & Post-operative Rehabilitation (Swanson-type Arthroplasty for PIP Osteoarthritis)¶
Topic scope: post-operative rehabilitation after silicone (Swanson-type) proximal interphalangeal (PIP) joint arthroplasty for primary osteoarthritis. The worn joint surfaces are excised and a flexible silicone spacer is implanted; this is an interposition / encapsulation arthroplasty, not a rigidly-fixed mechanical hinge. The implant works as a flexible spacer around which a peri-implant fibrous capsule forms to provide stability. The dominant, reliable benefit is pain relief; the functional gain is a modest active arc (~40–60°), not restoration of normal range.
Defining principle of the rehab here: the rehabilitation pathway is dictated by the surgical approach, because the rate-limiting tissue is the extensor mechanism, not the implant. A volar (palmar) approach leaves the central slip and extensor mechanism intact → it permits immediate / early active motion (within 3–5 days). A dorsal approach must split or reflect the central slip to reach the joint → the extensor repair must be protected first with extension orthotics and a graded, short-arc flexion programme. Across both pathways the silicone spacer is stable in the sagittal (flexion–extension) plane but vulnerable in the coronal plane, so the programme deliberately avoids lateral / torsional load and tracks the joint in a pure sagittal arc (buddy strapping). Therapy aims to bank the useful arc before scar maturation fixes it while protecting extension and the implant — it is not an immobilise-to-heal construct in the volar case.
A. PROCEDURE OUTCOMES (silicone PIP arthroplasty for osteoarthritis)¶
Silicone PIP arthroplasty is a reliable pain-relieving operation with predictable but modest motion; the principal debates are over surgical approach and implant choice (silicone vs surface-replacement/pyrocarbon), not whether arthroplasty relieves pain.
- Pain relief is high and durable; motion gains are modest. A long-term series of Swanson silicone PIP arthroplasty for osteoarthritis (mean ~10-year follow-up) reported excellent pain relief (mean VAS ~0.4) with essentially unchanged arc (≈55° pre-op → ≈50° post-op) and high patient satisfaction — patients would have the surgery again despite limited motion gain [Bales, Wall & Stern, J Hand Surg Am 2014]. Moderate (level-IV long-term cohort).
- The volar approach can improve the active arc. A volar-approach silicone PIP series reported the active arc improving from ~33° to ~72°, with good function and satisfaction, by preserving the extensor mechanism and enabling early motion [Proubasta et al., J Hand Surg Am 2014]. Moderate–weak (level-IV).
- Radiographic implant deformation/fracture is common but poorly correlated with symptoms. In the long-term Swanson series most implants deformed and many fractured radiographically, yet clinical revision was uncommon (survivorship ~90% at ~10 years) and there was no correlation between radiographs and satisfaction [Bales, Wall & Stern 2014]. Strong natural-history signal within a cohort.
- Silicone vs surface-replacement and pyrocarbon implants give broadly comparable clinical results; no implant is clearly superior. Systematic review across implants/approaches found comparable outcomes with implant-/approach-specific complication profiles [Yamamoto et al., Plast Reconstr Surg 2017; Carlson Strother, Moran & Rizzo, JAAOS 2023]. Moderate (SR + narrative review).
- Pyrocarbon and resurfacing implants carry their own failure modes (subsidence, squeaking, intra-operative periprosthetic fracture, instability), informing implant choice rather than rehab [Watts et al., J Hand Surg Am 2012; Wagner et al. medium-term 2018 & intra-op fractures 2015; Branam et al. resurfacing-vs-silicone 2007]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE¶
The central rehab questions are (1) how soon to move and (2) how to splint, and the answer to both is set by the surgical approach and the extensor mechanism. The evidence base is low-level (expert consensus / single-cohort therapy series) — there are no RCTs comparing PIP arthroplasty rehab pathways.
- Approach dictates the timeline (the core principle). Surgical reviews establish that a volar approach preserves the central slip and permits immediate active and passive motion, while a dorsal approach requires post-operative protection of the split/repaired central slip before flexion is advanced [Renfree, Bone Joint J 2022 (surgical approaches); Herren, Hand Clin 2017; Yamamoto et al. 2017]. Moderate (surgical evidence) — strong mechanistic basis.
- A structured 12-week, splint-based therapy programme is the consensus framework (dorsal pathway). Feldscher's hand-therapy protocol for PIP (pyrocarbon, central-slip-splitting dorsal approach) uses a volar static finger orthosis allowing a limited short-arc PIP/DIP active arc that is increased over the rehab course, with a hand-based resting splint (MCP flexed, PIP/DIP near 0°) for full-time use except during template-splint exercise [Feldscher, J Hand Ther 2010]. Weak (expert-consensus protocol).
- A defined controlled-motion program exists and reports good arcs. A controlled-motion rehabilitation program for PIP arthroplasty reported favourable range-of-motion outcomes, supporting graded controlled motion over rigid immobilisation [Ramanathan, Koludrovich & Evans, J Hand Ther 2021]. Weak (cohort / programme description).
- Static and dynamic extension splinting give similar results. A comparison of static vs dynamic splinting after PIP pyrocarbon arthroplasty found comparable outcomes, favouring static splinting for simplicity and patient convenience [Jennings & Livingstone / static-vs-dynamic cohort, J Hand Ther 2011]. Weak–moderate (comparative cohort).
- Coronal-plane protection is the durable, lifelong caveat. Collateral integrity and avoidance of lateral stress underpin long-term implant stability; collateral compromise drives instability/deviation [Carlo et al., collateral reconstruction, J Hand Surg Am 2016; Carlson Strother et al. 2023]. Consensus / mechanistic.
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint (by approach) | Hand-therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Protect & initiate motion | Week 0–3 | Volar: active motion at 3–5 days, short flexion arc (~30°) in template/extension-block splint. Dorsal: PIP splinted near extension full-time; supervised short-arc flexion only | Protected sagittal PIP/DIP motion; tendon glides; buddy strapping; uninvolved-joint motion; no lateral/torsional load | None (no grip/pinch) | Implant stable in flexion–extension, vulnerable coronally |
| II — Advance motion | Week 3–6 | Progressively increase flexion arc toward ~40–60°. Dorsal: wean extension splint as central slip consolidates (≈wk 4–6); guard against extensor lag | Graded active/AAROM flexion–extension; blocking; scar massage once healed; continue buddy strapping | Still no resisted strengthening | Bank the useful arc before scar maturation fixes it |
| III — Strengthen & return | Week 6–12+ | Lifting/grip restrictions progressively lifted; lateral/twisting load avoided indefinitely | Light grip → cautious pinch; functional & work-specific loading | Grip from ~6 wk, graded | Pain relief is the durable gain; final arc (~40–60°) largely set by ~3 months |
(Phase windows mirror the precautions in the patient protocol; they are typical guides — not trial-derived deadlines — and the volar vs dorsal split is the dominant variable.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Volar vs dorsal approach (the rehab-defining question). The volar approach spares the extensor mechanism and permits early active motion (and a better reported arc), at the cost of being more technically demanding; the dorsal approach is more familiar but mandates extensor protection and a slower, splint-led flexion programme. Choice is surgeon-dependent and drives the entire rehab pathway. Moderate surgical evidence; no head-to-head rehab RCT.
- Implant choice (silicone vs surface-replacement vs pyrocarbon). No implant is clearly superior on clinical outcomes; silicone is durable for pain relief with high radiographic deformation/fracture that poorly predicts symptoms, while pyrocarbon/resurfacing trade different complication profiles (subsidence, instability, intra-operative fracture). Moderate (SR + cohorts).
- Static vs dynamic splinting (dorsal pathway). Comparable outcomes; static splinting is favoured for simplicity and convenience. Weak–moderate.
- Motion gain is modest and that is expected, not failure. Patients reliably lose pain but gain little arc (especially via dorsal/silicone); mislabelling the modest arc as a poor result misframes a successful pain-relieving operation. Counsel the ~40–60° expectation up front. Strong natural-history signal.
- Lifelong coronal-stress avoidance. Long-term stability depends on the peri-implant capsule and collaterals; forceful lateral/twisting load risks deviation, instability and implant failure. Consensus.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (mechanistic / natural-history): the surgical-approach principle (volar preserves extensor mechanism → early motion; dorsal splits central slip → protect extension first); the modest-arc / reliable-pain-relief outcome pattern; radiographic implant deformation poorly predicting symptoms.
- MODERATE: procedure outcomes are level-IV case series (long-term Swanson silicone series; volar approach series); implant-comparison systematic review/narrative review; surgical-approach reviews.
- WEAK / EXPERT CONSENSUS: the specific rehabilitation regimen — short-arc controlled motion, 12-week splint-based programme, static-vs-dynamic splinting equivalence, exact phase timings. These are low-level, expert-consensus / single-cohort therapy descriptions, not trial-derived; individualise to the operative approach and tissue quality.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2013.11.008
- Proubasta IR, Lamas CG, Natera L, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014;39(6). DOI: 10.1016/j.jhsa.2014.03.033
- Weistra K, Kan HJ, van Alebeek VAHJ, et al. Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex in 72 cases. HAND. 2022. DOI: 10.1177/15589447221122829
- Branam BR, Tuttle HG, Stern PJ, et al. Resurfacing arthroplasty versus silicone arthroplasty for proximal interphalangeal joint osteoarthritis. J Hand Surg Am. 2007. DOI: 10.1016/j.jhsa.2007.04.006
- Yamamoto M, Malay S, Fujihara Y, et al. A systematic review of different implants and approaches for proximal interphalangeal joint arthroplasty. Plast Reconstr Surg. 2017. DOI: 10.1097/prs.0000000000003260
- Renfree KJ. Surgical approaches for proximal interphalangeal joint arthroplasty. Bone Joint J. 2022;104-B(12). DOI: 10.1302/0301-620x.104b12.bjj-2022-0946
- Herren DB. Current European practice in the treatment of proximal interphalangeal joint arthritis. Hand Clin. 2017. DOI: 10.1016/j.hcl.2017.04.002
- Carlson Strother CR, Moran SL, Rizzo M. Small joint arthroplasty of the hand: an update on indications, outcomes, and complications. J Am Acad Orthop Surg. 2023;31(15). DOI: 10.5435/jaaos-d-23-00034
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. DOI: 10.1016/j.jht.2009.10.011
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. DOI: 10.1016/j.jht.2019.04.003
- Watts AC, Hearnden AJ, Trail IA, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: minimum two-year follow-up. J Hand Surg Am. 2012. DOI: 10.1016/j.jhsa.2012.02.012
- Wagner ER, Weston JT, Houdek MT, et al. Medium-term outcomes with pyrocarbon proximal interphalangeal arthroplasty: a study of 170 consecutive arthroplasties. J Hand Surg Am. 2018. DOI: 10.1016/j.jhsa.2018.06.020
- Wagner ER, Van Demark R, Kor DJ, et al. Intraoperative periprosthetic fractures in proximal interphalangeal joint arthroplasty. J Hand Surg Am. 2015. DOI: 10.1016/j.jhsa.2015.06.101
- McGuire DT, White CD, Carter SL, et al. Pyrocarbon proximal interphalangeal joint arthroplasty: outcomes of a cohort study. J Hand Surg Eur Vol. 2011;37(6). DOI: 10.1177/1753193411434053
- Carlo J, Dell PC, Matthias R, et al. Collateral ligament reconstruction of the proximal interphalangeal joint. J Hand Surg Am. 2016;41(1). DOI: 10.1016/j.jhsa.2015.10.007
- Aversano FJ, Calfee RP. Salvaging a failed proximal interphalangeal joint implant. Hand Clin. 2018. DOI: 10.1016/j.hcl.2017.12.011
PIP arthroplasty rehabilitation literature (URLs)¶
- Feldscher SB. Postoperative management for PIP joint pyrocarbon arthroplasty. J Hand Ther. 2010. https://pubmed.ncbi.nlm.nih.gov/20036511/
- Ramanathan D, Koludrovich J, Evans P. A new controlled motion program for rehabilitation of the proximal interphalangeal joint arthroplasty. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/31481342/
- Static versus dynamic splinting for proximal interphalangeal joint pyrocarbon implant arthroplasty: a comparison of current and historical cohorts. J Hand Ther. 2011. https://pmc.ncbi.nlm.nih.gov/articles/PMC3143198/
- Proubasta IR, et al. Silicone proximal interphalangeal joint arthroplasty for primary osteoarthritis using a volar approach. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24799141/
- Bales JG, Wall LB, Stern PJ. Long-term results of Swanson silicone arthroplasty for PIP joint osteoarthritis. J Hand Surg Am. 2014. https://pubmed.ncbi.nlm.nih.gov/24559624/
- The dorsal approach to silicone implant arthroplasty of the proximal interphalangeal joint. J Hand Surg Am. 2007. https://www.sciencedirect.com/science/article/abs/pii/S0363502307004662
- Proximal interphalangeal joint arthroplasty using a silicone implant: a comparison between Integra and NeuFlex. HAND. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC10953532/