Patients › Rehabilitation
Gãy xương cổ tay xa (ORIF)
Staged rehabilitation after plate fixation of a distal radius fracture, from the first days to return to full activity.
Hướng dẫn này hỗ trợ quá trình hồi phục của bạn sau phẫu thuật cố định gãy xương cẳng tay xa (cổ tay) (nội soi và cố định bên trong, ORIF) với Bác sĩ Kieran Hirpara tại Bệnh viện tư nhân Mater Rockhampton. Hướng dẫn bắt đầu bằng chương trình bài tập tại nhà của bạn, tiếp theo là phác đồ lâm sàng có cấu trúc được viết dành cho nhà vật lý trị liệu hoặc chuyên gia trị liệu tay của bạn: hãy mang theo trang này hoặc file PDF của nó đến buổi trị liệu đầu tiên để quá trình phục hồi chức năng của bạn được phối hợp nhịp nhàng. Chuyên gia trị liệu của bạn có thể điều chỉnh kế hoạch tùy thuộc vào tiến triển hồi phục của bạn.
Nếu bạn có bất kỳ lo ngại nào về vết mổ sau phẫu thuật, hãy liên hệ với phòng khám. Thường thì việc chụp ảnh vết mổ và gửi qua email để xem xét sẽ rất hữu ích.
Những điều cần biết¶
Để biết thông tin về chăm sóc vết thương, giảm sưng và quản lý sẹo, vui lòng tham khảo hướng dẫn chăm sóc vết thương của phòng khám.
Sau phẫu thuật, bạn có thể được giới thiệu đến chuyên trị liệu viên tay để chế tạo nẹp nhựa nhiệt dẻo. Trong trường hợp này, nẹp sẽ được đeo tạm thời để tăng sự thoải mái và bảo vệ, và bạn vẫn cần tháo nẹp ra để thực hiện chương trình bài tập tại nhà. Nếu được giới thiệu để đeo nẹp, bạn sẽ nhận được thêm thông tin chi tiết về cách đeo và chăm sóc nẹp.
Các bài tập dưới đây rất quan trọng để khôi phục tầm vận động của các ngón tay, cổ tay và cẳng tay. Chườm nóng và chườm lạnh là các phương pháp thường được sử dụng để khôi phục tầm vận động, phục hồi chức năng và cải thiện sự thoải mái. Sau khi vết thương đã lành, bạn có thể chườm nóng trước khi tập; một túi chườm đá có thể được sử dụng sau đó để ngăn ngừa hoặc làm giảm tình trạng viêm.
Quản lý sẹo (đặc biệt là massage) rất quan trọng sau phẫu thuật xương trụ xa, để các gân chạy dưới đường rạch vết mổ có thể trượt tự do và không bị dính (bám chặt) vào sẹo đang lành.
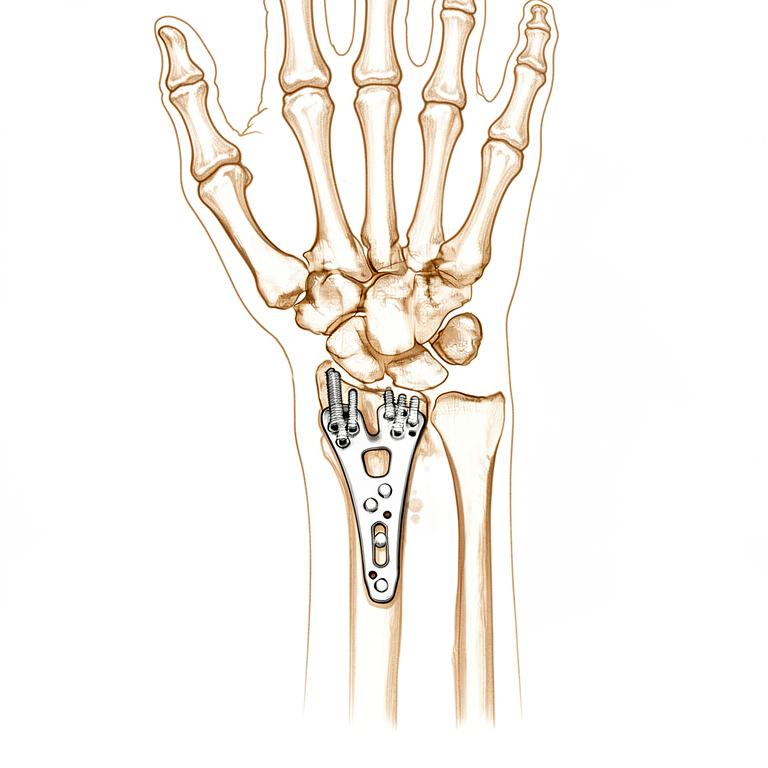
Tấm vít khóa mặt lòng được thiết kế để cố định ổ gãy chắc chắn đủ để bắt đầu vận động sớm, và phác đồ này được xây dựng dựa trên nguyên tắc đó. Các nghiên cứu so sánh vận động cổ tay sớm với bất động trong vài tuần sau cố định bằng tấm vít mặt lòng cho thấy việc bắt đầu vận động sớm có thể cải thiện tầm vận động ngắn hạn, lực nắm và sự thoải mái mà không làm ảnh hưởng đến vị trí của ổ gãy [1][2]. Đồng thời, các thử nghiệm so sánh việc bắt đầu vận động cổ tay ở khoảng hai tuần với việc bắt đầu ở khoảng sáu tuần cho thấy cả hai nhóm đều có kết quả tương tự sau ba đến sáu tháng [3], vì vậy mặc dù có lợi ích ban đầu, không cần phải vội vàng, và sự tiến triển ổn định được nêu dưới đây đã được hỗ trợ bởi nhiều bằng chứng. Quá trình liền xương diễn ra theo tiến trình riêng của nó bất kể cổ tay cảm thấy thế nào, đó là lý do tại sao các biện pháp phòng ngừa sau (không chịu tải, không nâng vật nặng hoặc tham gia các môn thể thao tiếp xúc cho đến 12 tuần sau khi gãy xương) vẫn được duy trì ngay cả khi vận động đã trở nên thoải mái.
Các biện pháp phòng ngừa và hạn chế¶
Việc sử dụng tay nhẹ nhàng trong các hoạt động chức năng hàng ngày như tự chăm sóc bản thân, ăn uống, mặc quần áo, viết và gõ máy tính là được khuyến khích.
Điều quan trọng là tránh nâng vật, nắm chặt, chịu tải trọng và tác động trong vòng 8 tuần sau phẫu thuật. Các bài tập tăng cường sức mạnh nhẹ nhàng được bắt đầu dần dần từ khoảng tuần thứ 4, khởi đầu với các bài tập nhẹ cho ngón tay và các bài tập đẳng trương cho cổ tay, sau đó được tăng cường cẩn thận để không làm mất đi sự bảo vệ ban đầu này.
Đây là các bài tập từ tài liệu hướng dẫn của bạn, nhằm khôi phục khả năng vận động của ngón tay, cổ tay và cẳng tay. Nếu bạn đang đeo nẹp, hãy tháo nó ra trước khi thực hiện các bài tập. Bắt đầu thực hiện các bài tập theo hướng dẫn của Bác sĩ Hirpara và chuyên viên trị liệu của bạn.
Bài tập của bạn¶
Giao thức lâm sàng của bạn¶
Phần còn lại của trang này là giao thức lâm sàng tăng tốc cho một trường hợp gãy xương cẳng tay xa được điều trị bằng phẫu thuật nắn mở và cố định nội khoa với tấm xương lòng bàn tay. Phần này sẽ được cung cấp cho nhà vật lý trị liệu hoặc chuyên gia trị liệu bàn tay của bạn, và mỗi giai đoạn dưới đây bắt đầu bằng một giải thích bằng ngôn ngữ thông thường về những gì đang xảy ra.
Những ngày 1–4 sau phẫu thuật¶
Trong vài ngày đầu, trọng tâm là bảo cố định, giảm sưng và duy trì vận động các ngón tay, cổ tay, cẳng tay, khuỷu tay và vai. Băng phẫu thuật được giữ nguyên cho đến ngày thứ 3, khi đó băng được tháo bớt và vết thương được băng lại. Giữ tay ở tư thế nâng cao khi nghỉ ngơi, sử dụng tay cho các công việc hàng ngày nhẹ (dưới 1–2 kg) trong giới hạn thoải mái, và tránh chịu tải trọng qua cánh tay, nắm chặt hoặc nâng vật nặng. Nẹp không được yêu cầu thường quy, nhưng có thể được chuẩn bị nếu bệnh nhân quay trở lại làm việc hoặc cổ tay đau nhiều hơn.
Dành cho nhà vật lý trị liệu:
Trước khi điều trị, kiểm tra phim X-quang, báo cáo phẫu thuật và tiền sử bệnh (PMHx) của bệnh nhân, và phối hợp với bác sĩ phẫu thuật điều trị về độ ổn định của cố định gãy xương và tiên lượng dự kiến.
Giáo dục và các biện pháp phòng ngừa
- Tránh chịu tải trọng qua cánh tay, nắm chặt hoặc nâng vật nặng
- Khuyến khích sử dụng tay bị ảnh hưởng cho các hoạt động sống hàng ngày (ADL) nhẹ (dưới 1–2 kg) trong giới hạn đau và các mẫu vận động bình thường
Quản lý
- Nẹp: Không yêu cầu, nhưng có thể sử dụng nếu bệnh nhân quay trở lại làm việc hoặc trong trường hợp đau tăng; xem xét sử dụng nẹp nhiệt dẻo hoặc hỗ trợ có sẵn
- Vết thương: Băng phẫu thuật/băng gạc được giữ nguyên cho đến ngày thứ 3; tháo bớt băng và băng lại vết thương từ ngày thứ 3 sau phẫu thuật; giáo dục về quản lý vết thương
- Phù nề: Cung cấp giáo dục về tư thế nâng cao; cung cấp liệu pháp chèn ép và mát-xa ngược dòng khi cần thiết
- Bài tập: Cung cấp bài tập "sáu gói" chủ động để duy trì tầm vận động (ROM) của các ngón tay; cung cấp bài tập tầm vận động chủ động của cổ tay, cẳng tay và ngón tay; khuyến khích tầm vận động chủ động thường xuyên của khuỷu tay và vai
Tuần 2–4 sau phẫu thuật¶
Chỉ khâu được tháo ra vào ngày 10–14, và xoa sẹo bắt đầu khi vết thương đã lành đủ. Chương trình tập luyện tiếp tục (các bài tập sáu gói ngừng lại khi các ngón tay của bạn phục hồi hoàn toàn tầm vận động) và bắt đầu tăng cường sức mạnh cổ tay đẳng trương (isometric) nhẹ nhàng. Trong giai đoạn này, cổ tay vẫn chỉ nên di chuyển dưới sức mạnh cơ của chính nó: không ai, kể cả bạn, nên đẩy hoặc kéo giãn cổ tay một cách thụ động, vì gãy xương vẫn đang liền. Tiếp tục tránh chịu tải, nắm chặt và nâng vật; các hoạt động hàng ngày nhẹ dưới 1–2 kg được khuyến khích. Bạn không được lái xe khi cổ tay còn trong nẹp; việc lái xe sẽ được tiếp tục khi bạn tháo nẹp ra, như đã xác nhận tại buổi tái khám.
Dành cho nhà vật lý trị liệu của bạn:
Đánh giá
- Đánh giá tự báo cáo: Đánh giá Cổ tay do Bệnh nhân Tự báo cáo (PRWE), Khuyết tật của Cánh tay, Vai và Tay (DASH)
- Đo chu vi phù nề
- Thang đo đau tương tự trực quan (VAS) hoặc thang đo điểm số
- Đo góc vận động chủ động (AROM): bàn tay, cổ tay
- Đánh giá chủ quan, bao gồm sự tuân thủ của bệnh nhân với phác đồ, việc sử dụng chức năng của bàn tay trong các hoạt động sinh hoạt hàng ngày (ADL), và các vấn đề/nỗi lo ngại
Giáo dục và thận trọng
- Tránh chịu tải qua cánh tay, nắm chặt hoặc nâng vật
- Không vận động cổ tay thụ động
- Khuyến khích sử dụng bàn tay bị ảnh hưởng cho các hoạt động sinh hoạt hàng ngày (ADL) nhẹ (dưới 1–2 kg) trong giới hạn đau và các mẫu vận động bình thường
- Không lái xe khi đang mang nẹp; việc lái xe sẽ được tiếp tục khi tháo nẹp ra, được xác nhận tại buổi tái khám
Quản lý
- Vết thương/sẹo: tháo chỉ khâu vào ngày 10–14; bắt đầu quản lý sẹo phù hợp, phụ thuộc vào tiến trình lành thương
- Phù nề: xem xét sử dụng băng chèn ép, xoa bóp ngược dòng, di động phù nề bằng tay (MEM), tắm nước nóng/lạnh xen kẽ và/hoặc nâng cao nếu cần thiết
- Bài tập: ngừng các bài tập sáu gói chủ động khi đạt được tầm vận động hoàn toàn của các ngón tay; xem xét các bài tập thụ động cho ngón tay và ngón cái, bao gồm đặt/giữ, nếu tầm vận động chủ động chưa hoàn toàn ở bàn tay; tiếp tục các bài tập vận động cổ tay chủ động; khuyến khích vận động khuỷu tay và vai chủ động thường xuyên; bắt đầu tăng cường sức mạnh cổ tay đẳng trương
Xử lý sự cố
- Theo dõi các dấu hiệu nhiễm trùng vết thương, thay đổi cảm giác ở bàn tay, hoặc các dấu hiệu sớm của hội chứng đau vùng phức tạp (CRPS)
- Xác định các mẫu vận động bất thường và can thiệp khi cần thiết
Tuần 4–6 sau phẫu thuật¶
Giai đoạn này bắt đầu các bài tập tăng cường sức mạnh một cách nhẹ nhàng: từ tuần thứ 4, bắt đầu các bài tập tăng cường sức mạnh cho các ngón tay với lực kháng thấp, trong khi các bài tập đẳng trương (isometric) cho cổ tay tiếp tục được duy trì và dần dần nâng cấp. Nếu phim X-quang cho kết quả khả quan và cố định ổn định, các bài tập duỗi cổ tay thụ động nhẹ nhàng (trong đó cổ tay được di chuyển bằng sự hỗ trợ của tay kia hoặc của nhà trị liệu) có thể bắt đầu từ tuần 4–6. Việc khôi phục phạm vi chuyển động vẫn được ưu tiên hơn việc xây dựng sức mạnh. Tiếp tục tránh chịu trọng lượng qua cánh tay và nâng vật nặng, trong khi vẫn tiếp tục sử dụng bàn tay cho các công việc hàng ngày nhẹ nhàng.
Dành cho nhà vật lý trị liệu của bạn:
Đánh giá
- Đo chu vi giảm phù nề
- Thang điểm đau tương tự trực quan (VAS) hoặc thang điểm đánh giá số
- Đo góc vận động chủ động (AROM) và chất lượng của các mẫu chuyển động
- Đánh giá chủ quan, bao gồm mức độ tuân thủ phác đồ của bệnh nhân, khả năng sử dụng chức năng của bàn tay trong các hoạt động sống thường ngày (ADL), và các vấn đề/nỗi lo ngại
- Đo lực nắm bằng lực kế (3 lần mỗi bên chi)
Giáo dục và các biện pháp phòng ngừa
- Tránh chịu trọng lượng qua cánh tay hoặc nâng vật nặng
- Khuyến khích sử dụng bàn tay bị ảnh hưởng cho các công việc sinh hoạt thường ngày (ADL) nhẹ nhàng (dưới 1–2 kg) trong giới hạn chịu đau và các mẫu chuyển động bình thường
Quản lý điều trị
- Sẹo: tiếp tục quản lý sẹo theo yêu cầu
- Phù nề: tiếp tục liệu pháp chèn ép, mát-xa ngược dòng, MEM (kỹ thuật vận động cơ bắp chủ động thụ động) và kê cao chi theo yêu cầu; ngừng ngâm nước đối kháng
- Bài tập: tiếp tục các bài tập thụ động cho ngón tay và ngón cái nếu phạm vi vận động (ROM) chưa đầy đủ; tiếp tục các bài tập vận động chủ động cho cổ tay; bắt đầu các bài tập tăng cường sức mạnh cho ngón tay với lực kháng thấp từ tuần thứ 4; bắt đầu các bài tập thụ động nhẹ nhàng cho cổ tay từ tuần 4–6 nếu cố định bằng phẫu thuật (ORIF) ổn định và phim X-quang cho kết quả khả quan; khuyến khích vận động chủ động thường xuyên cho khuỷu tay và vai; tiếp tục/nâng cấp các bài tập tăng cường sức mạnh đẳng trương cho cổ tay
Xử lý các vấn đề phát sinh
- Đánh giá lại các dấu hiệu của hội chứng đau vùng phức tạp (CRPS) và đau vai
- Cân nhắc khối lượng bài tập trong chương trình tại nhà và ưu tiên phạm vi vận động (ROM) hơn sức mạnh
- Nếu phạm vi vận động cổ tay bị hạn chế đáng kể, hãy cân nhắc bắt đầu các bài tập vận động thụ động nhẹ nhàng (PROM) cho cổ tay trong giới hạn VAS dưới 4/10, với sự chấp thuận của bác sĩ phẫu thuật
Tuần thứ 6–8 sau phẫu thuật¶
Giai đoạn này bắt đầu quá trình trở lại hoạt động bình thường một cách có kiểm soát trong 3 tuần tới. Việc tăng cường sức mạnh cổ tay được nâng lên mức sử dụng trọng lượng nhẹ (0,5–1,0 kg) hoặc dây kháng lực theraband có độ kháng thấp, và mức độ kháng lực cho việc tăng cường sức mạnh ngón tay cũng được tăng lên. Vẫn còn hai giới hạn nghiêm ngặt: không chịu tải, nâng vật nặng hoặc tham gia các môn thể thao tiếp xúc cho đến khi đủ 12 tuần sau khi gãy xương. Chuyên viên vật lý trị liệu của bạn sẽ xem xét cho xuất viện khi bạn có phạm vi vận động đầy đủ và sự phục hồi chức năng phù hợp.
Dành cho chuyên viên vật lý trị liệu của bạn:
Đánh giá
- Đo chu vi phù nề khi cần thiết
- Thang điểm đau tương tự trực quan (VAS) hoặc thang điểm đánh giá số
- Đo góc vận động chủ động (AROM)
- Sức mạnh nắm tay
- Đánh giá chủ quan
Giáo dục và các biện pháp phòng ngừa
- Trở lại hoạt động bình thường một cách có kiểm soát trong 3 tuần tới
- Tránh chịu tải, nâng vật nặng và các môn thể thao tiếp xúc cho đến khi đủ 12 tuần sau khi gãy xương
Quản lý điều trị
- Sẹo: tiếp tục quản lý sẹo theo yêu cầu
- Phù nề: tiếp tục quản lý phù nề theo yêu cầu
- Bài tập: tiếp tục các bài tập thụ động cho ngón tay và ngón cái nếu phạm vi vận động chưa đầy đủ; tiếp tục các bài tập vận động thụ động và chủ động cho cổ tay nếu cần thiết; tăng mức độ kháng lực trong các bài tập tăng cường sức mạnh ngón tay; bắt đầu các bài tập tăng cường sức mạnh cổ tay bằng cách sử dụng trọng lượng 0,5–1,0 kg hoặc dây kháng lực theraband có độ kháng thấp; nâng cấp trọng lượng và mức độ kháng lực sử dụng trong chương trình tăng cường sức mạnh cổ tay khi bệnh nhân dung nạp tốt
Xử lý các vấn đề phát sinh
- Cân nhắc/bắt đầu nẹp tuần tự tiến triển ban đêm, nẹp dạng bao tay hoặc nẹp động lực học nếu phạm vi vận động cải thiện chậm
- Theo dõi bất kỳ dấu hiệu nào của sự không ổn định cổ tay và điều trị thích hợp
- Cân nhắc xuất viện khi có phạm vi vận động đầy đủ và sự phục hồi chức năng phù hợp
- Cân nhắc giới thiệu lại cho bác sĩ điều trị nếu tình trạng bị đình trệ và/hoặc có kết quả điều trị kém
Phác đồ này được viết với sự hợp tác của Sarah Farrell, BOccThy AHT, và Kristy Gerlach, BOccThy AHT.
Sau khi thực hiện phác đồ của bạn¶
Phác đồ này được thực hiện song song với các lời khuyên chung về phục hồi chức năng của phòng khám; xem quản lý đau sau phẫu thuật, chăm sóc vết thương và cơ bản về trị liệu tay. Về ca phẫu thuật và chấn thương mà nó điều trị, xem cố định xương quay xa (ORIF) và gãy xương quay xa. Kế hoạch theo từng giai đoạn ở trên phù hợp với các bằng chứng được công bố về phục hồi chức năng sau cố định bằng tấm khóa mặt lòng, và quá trình phục hồi tiếp theo của bạn được hướng dẫn cá nhân hóa bởi bác sĩ vật lý trị liệu hoặc chuyên gia trị liệu tay dựa trên sự tiến triển của cổ tay bạn.
Tài liệu tham khảo¶
[1] Quadlbauer S, Pezzei C, Jurkowitsch J, et al. Vận động sớm các gãy xương cẳng tay dưới được cố định bằng tấm khóa mặt lòng cho kết quả ngắn hạn tốt hơn so với bất động trong năm tuần: một thử nghiệm ngẫu nhiên có đối chứng. Arch Orthop Trauma Surg. 2022;142(5):1–11. https://pubmed.ncbi.nlm.nih.gov/34852677/ [2] Gutiérrez-Espinoza H, Araya-Quintanilla F, Olguín-Huerta C, et al. Hiệu quả của vận động sớm so với vận động muộn ở bệnh nhân gãy xương cẳng tay dưới được điều trị bằng tấm khóa mặt lòng: một đánh giá hệ thống và phân tích tổng hợp. Hand Surg Rehabil. 2020;39(4):261–271. https://www.sciencedirect.com/science/article/abs/pii/S2468122920302231 [3] Lozano-Calderón SA, Souer S, Mudgal C, Jupiter JB, Ring D. Vận động cổ tay sau cố định bằng tấm mặt lòng các gãy xương phần dưới xương quay. J Bone Joint Surg Am. 2008;90(6):1297–1304. https://pubmed.ncbi.nlm.nih.gov/18519324/ [4] Miller LK, Jerosch-Herold C, Shepstone L. Hiệu quả của các kỹ thuật quản lý phù nề trong điều trị phù nề bàn tay giai đoạn dưới cấp tính: một đánh giá hệ thống. J Hand Ther. 2017;30(4):432–446. https://pubmed.ncbi.nlm.nih.gov/28807598/
Evidence & references
Distal Radius Fracture (ORIF) — Post-operative Rehabilitation Evidence Brief¶
Topic scope: post-operative rehabilitation after open reduction and internal fixation (ORIF) of a distal radius fracture with a volar locking plate. This brief backs an early-motion-but-protected hand/wrist pathway delivered with hand therapy, where wrist motion begins early while bone-dependent loading (weight-bearing, heavy lifting, contact sport) is deferred until ~12 weeks. It does not cover the indications for surgery vs casting, nor fragment-specific/dorsal/bridge-plate constructs (which carry their own loading rules).
Defining principle of the rehab here: a volar locking plate is a fixed-angle construct stable enough to permit immediate wrist motion — the screws lock to the plate and hold the articular reduction independent of the cast. So (unlike a cast-treated fracture, and unlike a tendon or ligament repair) the wrist does not need weeks of immobilisation to protect the reduction: the rehab is an early-movement pathway — finger/forearm/wrist active motion and oedema control from day one, splint for comfort only, isometric then progressive strengthening from ~weeks 4–6. The one timeline that is not negotiable is bone healing: union takes ~6–12 weeks regardless of how the wrist feels, which is why weight-bearing, heavy lifting and impact are held to 12 weeks even once motion is comfortable.
A. PROCEDURE & CONSTRUCT — what the rehab is protecting¶
Volar locking plate fixation is the dominant operative construct for displaced distal radius fractures and is the reference standard against which other techniques are compared. Key surgical-outcome facts that shape the rehab:
- Volar locking plates restore and hold articular reduction reliably, and across randomised comparisons give equivalent or better functional outcomes than non-operative care and competing fixation methods (dorsal plating, intramedullary nailing, fragment-specific), with most differences favouring early function rather than final endpoint [JAAOS controversies review 2014; Hand Clinics plate-fixation review 2021; IM-nail-vs-volar-plate RCTs].
- The fixed-angle construct is the rationale for early motion. Because the locking screws hold the subchondral fragments rigidly, the plate — not a cast — maintains the reduction, so wrist motion can start before union without displacing the fracture [Hand Clinics 2021; accelerated-rehab RCT, JBJS 2014].
- In older patients the operative-vs-conservative outcome gap is small. A 3-year RCT in patients >70 found volar plating and non-operative care converged on similar patient-reported function — context that keeps post-operative rehab pragmatic and patient-centred rather than aggressive [BMC Musculoskelet Disord 2022; Hand Clinics geriatric review 2021].
- Recovery is gradual. Range, grip and patient-reported scores improve steadily over the first 3–6 months; the construct permits early motion but does not accelerate the biology of healing or the return of grip strength.
B. REHABILITATION / HAND-THERAPY EVIDENCE¶
The central rehab questions for this construct are (1) when to start wrist motion, (2) how much supervised therapy is needed, and (3) what the strengthening timeline should be. The evidence is clear on the first, nuanced on the second, and consensus-driven on the third.
- Early motion is safe and gives a short-term advantage. Multiple RCTs and a systematic review show that starting wrist motion early after volar plating improves short-term ROM, grip and comfort without compromising the radiographic reduction [accelerated-rehab RCT, JBJS 2014; early-vs-late motion RCT, HAND 2018; Hand Therapy systematic review 2020]. This is the direct warrant for the day-1 finger/forearm/wrist program in this protocol.
- "Early" need not mean "immediate," and the advantage washes out by 3–6 months. The landmark trial comparing wrist mobilisation at ~2 weeks vs ~6 weeks found the two groups equivalent by 3–6 months [Lozano-Calderón / JBJS 2008]. So there is a genuine early benefit but no penalty for a measured, comfort-led progression — which is exactly why this protocol can be unhurried.
- Routine supervised physiotherapy adds little over a coached home program for most patients. Systematic reviews and RCTs repeatedly find that a structured home exercise program preceded by instruction/coaching performs as well as formal supervised therapy for uncomplicated cases, and that prescribed exercise programs add limited benefit over advice for impairment/activity outcomes [HEP-vs-supervised SR, J Hand Ther 2014; J Physiother SR 2017; Hand Clinics "is therapy needed?" 2021; Arch Orthop Trauma Surg 2020]. This supports a home-program-first model with hand-therapy review, escalating supervision for stiffness, oedema or slow progress — the structure of this protocol.
- Oedema control and scar/tendon-glide management are standard therapy elements. Elevation, retrograde massage, manual oedema mobilisation and (early) compression are the evidence-informed oedema toolkit [edema-management SR, J Hand Ther 2017]; scar massage to keep the flexor tendons gliding under the volar incision is consensus hand-therapy practice rather than RCT-derived.
Phased post-op timeline (volar locking plate, early-motion pathway)¶
Phases match this topic's synthesis.md. Timings are post-operative weeks; the 12-week
loading limit is referenced to the fracture (injury) date.
| Phase | Window | Splint | Motion / use | Strengthening | Notes |
|---|---|---|---|---|---|
| I — Protect & move | Days 1–4 | Comfort only, not routine | Active finger (six-pack), wrist, forearm, elbow & shoulder ROM from day 1; light ADL < 1–2 kg within pain limits | — | Surgical bandage to day 3, then redress. Oedema control + elevation. No weight-bearing, gripping or lifting |
| II — Active range & oedema | Week 2–4 | Comfort/work only (no driving while splinted) | Continue active wrist ROM (no passive yet); six-pack stops once fingers full | Isometric wrist activation begins | Sutures out day 10–14; start scar massage once healed. Watch for CRPS. PRWE/DASH baseline |
| III — Passive range & light load | Week 4–6 | Off | Add gentle passive wrist stretches at 4–6 wk if x-ray satisfactory & fixation stable | Finger strengthening (low resistance) from wk 4; upgrade isometrics | Movement still prioritised over strength |
| IV — Graded strengthening & return | Week 6–8 | Off | Restore/maintain full active & passive ROM | Wrist strengthening with 0.5–1.0 kg / light theraband, progress as tolerated | Graded return over ~3 wk. No weight-bearing, heavy lifting or contact sport until 12 weeks post-fracture. Discharge on full ROM + functional return |
The phase structure mirrors published surgeon/hand-therapy ORIF protocols (early ROM → scar + oedema → passive range + light resistance → progressive strengthening, with heavy load/sport held to ~12–16 weeks) [Physiopedia Colles' ORIF protocol; institutional ORIF rehab guidelines].
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- How early to mobilise. Early motion (immediate–2 wk) gives a real short-term ROM/grip/comfort advantage that equalises by 3–6 months vs starting at ~6 weeks. The evidence therefore supports early motion but does not mandate aggression — a measured progression is fully defensible. Moderate–strong (multiple RCTs + SR).
- Supervised therapy vs coached home program. For uncomplicated fractures the best available evidence finds no consistent benefit of routine formal physiotherapy over a well-instructed home program; supervision is best targeted to stiffness, oedema, CRPS risk or slow progress. Moderate (SRs/RCTs), but heterogeneous.
- Strengthening and return-to-load timing. The week-by-week strengthening ramp and the 12-week loading hold are construct- and biology-based consensus, drawn from surgeon/hand- therapy protocols rather than a strengthening-timing RCT. Weak/consensus.
- Whether the wrist needs any immobilisation at all. Some trials report that omitting post-op immobilisation does not worsen outcomes after volar plating, supporting the "splint for comfort only" stance here. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG / MODERATE–STRONG (RCT / SR): early wrist motion after volar plating is safe and improves short-term ROM/grip/comfort without loss of reduction (accelerated-rehab RCT JBJS 2014; early-vs-late RCT HAND 2018; Hand Therapy SR 2020); ~2-wk vs ~6-wk mobilisation equivalent by 3–6 months (Lozano-Calderón JBJS 2008).
- MODERATE: volar locking plate is a reliable fixed-angle construct with equivalent/favourable outcomes vs alternatives (JAAOS 2014; Hand Clinics 2021); operative-vs-conservative outcomes converge in the elderly (BMC 2022); coached home program ≈ supervised therapy for uncomplicated cases (J Hand Ther 2014; J Physiother 2017; Hand Clinics 2021); evidence-based oedema management (J Hand Ther 2017).
- WEAK / CONSENSUS: the detailed strengthening ramp and 12-week loading limit (surgeon & hand-therapy protocols; biology- and construct-based, not trial-derived); scar/tendon-glide massage practice.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Accelerated rehabilitation compared with a standard protocol after distal radial fractures treated with volar open reduction and internal fixation. J Bone Joint Surg Am. 2014. DOI: 10.2106/jbjs.m.00860
- Wrist mobilization following volar plate fixation of fractures of the distal part of the radius. J Bone Joint Surg Am. 2008. DOI: 10.2106/jbjs.g.01368
- Early versus late motion following volar plating of distal radius fractures. HAND. 2018. DOI: 10.1177/1558944718787880
- A systematic review of how daily activities and exercises are recommended following volar plating of distal radius fractures and the efficacy and safety of early versus late mobilisation. Hand Therapy. 2020. DOI: 10.1177/1758998320967032
- AAOS/ASSH Clinical Practice Guideline Summary: Management of Distal Radius Fractures. J Am Acad Orthop Surg. 2022. DOI: 10.5435/jaaos-d-21-00719
- Controversies in the management of distal radius fractures. J Am Acad Orthop Surg. 2014. DOI: 10.5435/jaaos-22-09-566
- Plate fixation of distal radius fractures. Hand Clinics. 2021. DOI: 10.1016/j.hcl.2021.02.008
- Non-operative treatment or volar locking plate fixation for dorsally displaced distal radius fractures in patients over 70 years — a three-year follow-up of a randomized controlled trial. BMC Musculoskelet Disord. 2022. DOI: 10.1186/s12891-022-05394-7
- Distal radius fracture: HEP versus supervised therapy — a systematic review. J Hand Ther.
- DOI: 10.1016/j.jht.2013.08.017
- Prescribed exercise programs may not be effective in reducing impairments and improving activity during upper limb fracture rehabilitation: a systematic review. J Physiother. 2017. DOI: 10.1016/j.jphys.2017.08.009
- Is therapy needed after distal radius fracture treatment — what is the evidence? Hand Clinics.
- DOI: 10.1016/j.hcl.2021.02.012
- Rehabilitation after distal radius fractures: is there a need for immobilization and physiotherapy? Arch Orthop Trauma Surg. 2020. DOI: 10.1007/s00402-020-03367-w
- Management of complications of distal radius fractures. Hand Clinics. 2015. DOI: 10.1016/j.hcl.2014.12.002
- A comparison of the accuracy of two sets of diagnostic criteria in the early detection of complex regional pain syndrome following surgical treatment of distal radial fractures. J Hand Surg Eur Vol. 2012. DOI: 10.1177/1753193412469142
Distal radius / rehabilitation literature (URLs)¶
- AAOS/ASSH Clinical Practice Guideline Summary: Management of Distal Radius Fractures (full summary). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9196973/
- Practical application of the 2020 distal radius fracture AAOS/ASSH clinical practice guideline: a clinical case. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9035062/
- Rehabilitation for distal radial fractures in adults (Cochrane-style review). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC9250132/
- Rehabilitation after distal radius fractures: opportunities for improvement. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC10569825/
- Rehabilitation following surgically treated distal radius fractures: do immobilization and physiotherapy affect the outcome? PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8343619/
Published rehab protocols (surgeon / hand-therapy — basis for the phase structure)¶
- British Society for Surgery of the Hand / British Association of Hand Therapists — Distal Radius Fractures Working Group rehabilitation guidance (2024). https://www.hand-therapy.co.uk/_userfiles/pages/files/distal_radius_fractures_working_group_2024.pdf
- Colles' Fracture Post-Operative Rehabilitation Protocol. Physiopedia. https://www.physio-pedia.com/Colles%E2%80%99_Fracture_Post_Operative_Rehabilitation_Protocol
- Distal Radius ORIF Rehabilitation Guidelines. University of Virginia Department of Orthopaedic Surgery. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Distal-radius-ORIF.pdf
- Distal Radius ORIF Rehabilitation. Jared Lee, MD. https://jaredleemd.com/pdf/distal-radius-orif-rehabilitation/