Patients › Wrist
Phẫu thuật hợp nhất một phần cổ tay (Hợp nhất bốn xương và hợp nhất xương thuyền với xương nguyệt)
Patient-facing topic for four-corner and capitolunate (two-corner) fusion of the wrist — joint-preserving alternative to total wrist fusion that retains some bending motion.
Lý do phẫu thuật này được đề xuất¶
Bác sĩ phẫu thuật của bạn đã đề nghị thực hiện phẫu thuật hợp nhất một phần cổ tay, còn được gọi là hợp nhất xương thuyền-xương nguyệt (four-corner arthrodesis) hoặc hợp nhất xương thuyền-xương nguyệt-xương trụ (capitolunate arthrodesis), để điều trị thoái hóa khớp mức độ nặng ở cổ tay. Thủ thuật này thường được chỉ định khi các phương pháp điều trị không phẫu thuật không mang lại đủ sự giảm đau và tổn thương khớp cụ thể của bạn liên quan đến vùng xương thuyền-xương nguyệt. Phẫu thuật nhằm giảm đau và tăng cường độ ổn định bằng cách hợp nhất các xương còn lại khỏe mạnh với nhau.
Mục tiêu chính của phẫu thuật này là mang lại chức năng bền vững và ổn định theo thời gian. Bằng cách loại bỏ xương bị tổn thương và nối các xương còn lại, phẫu thuật nhằm mục đích ngăn chặn tình trạng ma sát gây đau đớn trong khi vẫn bảo tồn tối đa phạm vi vận động. Phương pháp này cung cấp một lựa chọn thay thế hiệu quả so với thay khớp cổ tay toàn phần hoặc hợp nhất khớp rộng rãi hơn, giúp bạn trở lại các hoạt động hàng ngày với ít khó chịu hơn.
Trước khi phẫu thuật¶
Bác sĩ phẫu thuật của bạn có thể sẽ chỉ định chụp X-quang, xét nghiệm máu hoặc MRI để kiểm tra cổ tay và tình trạng sức khỏe tổng quát trước khi phẫu thuật. Bạn cần nhịn ăn trong vài giờ trước thủ thuật và ngừng sử dụng một số loại thuốc theo hướng dẫn của bác sĩ phẫu thuật. Vui lòng sắp xếp để một người bạn hoặc người thân đưa bạn về nhà, vì bạn không thể tự lái xe. Mang theo danh sách đầy đủ tất cả các loại thuốc hiện tại và mặc quần áo thoải mái, rộng rãi khi đến bệnh viện. Phẫu thuật này được thực hiện thông qua một vết rạch mở duy nhất ở mặt sau cổ tay của bạn. Đội ngũ phẫu thuật sẽ xem xét tất cả các hướng dẫn cụ thể với bạn trực tiếp.
Vào ngày phẫu thuật¶
Bạn sẽ đến bệnh viện và gặp bác sĩ gây mê để thảo luận về kế hoạch chăm sóc của bạn. Phẫu thuật này được thực hiện dưới gây mê toàn thân. Bạn sẽ hoàn toàn bất tỉnh trong suốt quá trình phẫu thuật. Một số bệnh nhân cũng có thể được gây tê vùng thần kinh để giảm đau sau phẫu thuật; bác sĩ gây mê sẽ quyết định vào ngày phẫu thuật dựa trên tình trạng cá nhân của bạn.
Bác sĩ phẫu thuật sẽ thực hiện thủ thuật thông qua một vết rạch mở duy nhất ở cổ tay của bạn. Sau đó, bạn sẽ được chuyển đến khu vực hồi sức để tỉnh lại một cách an toàn. Bạn sẽ được theo dõi chặt chẽ trong khi tác dụng của thuốc gây mê dần hết.
Thủ thuật phẫu thuật bao gồm¶
Bác sĩ phẫu thuật của bạn sẽ thực hiện một vết rạch duy nhất ở mặt sau cổ tay để tiếp cận khớp. Phương pháp tiếp cận mở này cho phép tiếp cận trực tiếp vào các xương bên trong. Tùy thuộc vào bệnh viêm xương khớp cụ thể của bạn, bác sĩ phẫu thuật có thể loại bỏ xương thuyền (scaphoid) hoặc tái tạo bề mặt của xương đầu xương cổ tay (capitate) bằng một loại cấy ghép đặc biệt.
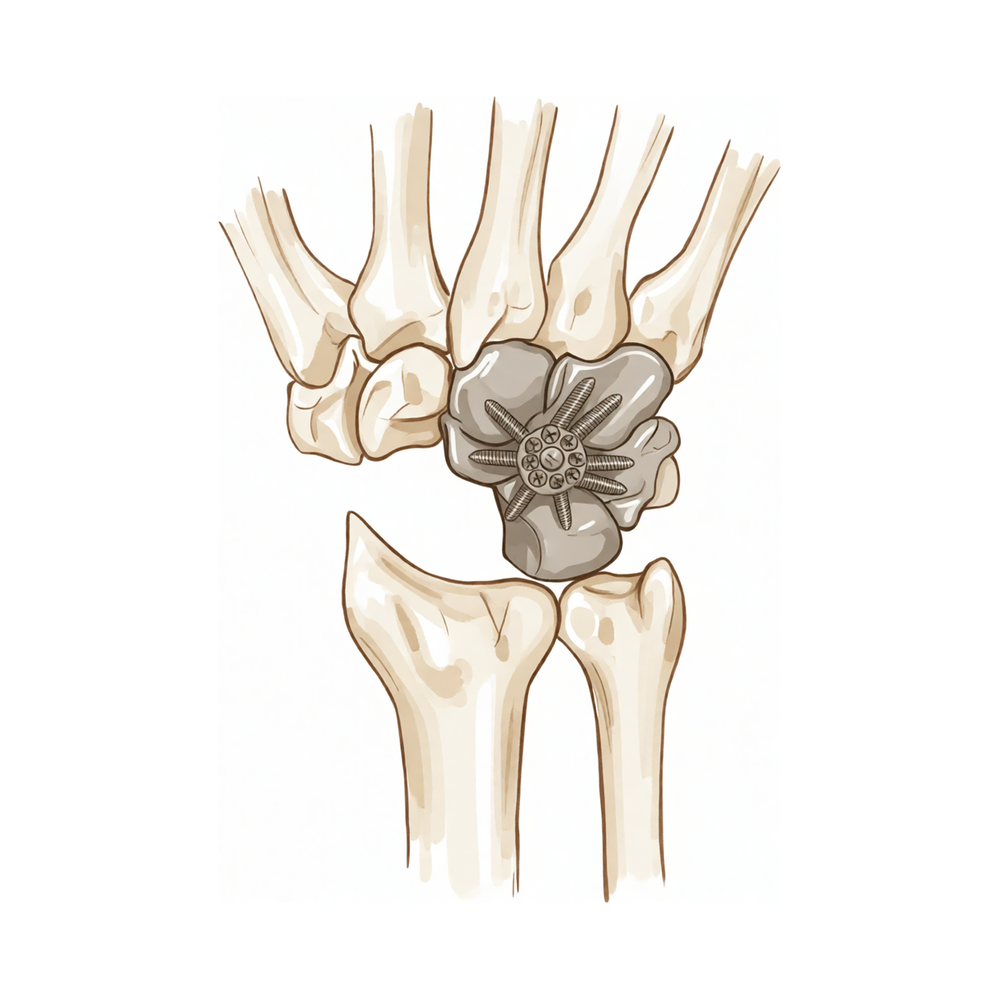
Tiếp theo, bác sĩ phẫu thuật chuẩn bị các bề mặt khớp để hợp nhất. Nếu bạn đang trải qua quá trình hợp nhất bốn góc (four-corner fusion), bác sĩ phẫu thuật sẽ loại bỏ xương thuyền và nối bốn xương cổ tay còn lại với nhau. Đối với quá trình hợp nhất đầu xương cổ tay và xương nguyệt (capitolunate fusion), chỉ có xương đầu xương cổ tay và xương nguyệt được nối với nhau. Bác sĩ phẫu thuật sử dụng vít, ghim hoặc tấm kim loại để giữ các xương này cố định trong khi chúng lành lại. Mảnh ghép xương tại chỗ có thể được thêm vào để hỗ trợ các xương phát triển liền nhau.
Cuối cùng, bác sĩ phẫu thuật khâu vết rạch và băng bó. Mục tiêu là tạo ra một cổ tay ổn định, không đau trong khi vẫn giữ được nhiều chuyển động nhất có thể ở các khớp còn lại. Thủ thuật này được thiết kế cho những cổ tay bị viêm xương khớp giai đoạn nặng, nơi các phương pháp điều trị khác không hiệu quả.
Sau phẫu thuật¶
Bạn sẽ tỉnh dậy tại khoa hồi sức, nơi nhóm bác sĩ sẽ kiểm soát cơn đau của bạn. Bác sĩ phẫu thuật của bạn sử dụng một vết rạch mở duy nhất ở cổ tay. Bạn sẽ ra viện với một lớp băng bó dày và một dây treo hoặc nẹp để bảo vệ cổ tay. Hầu hết bệnh nhân nằm lại bệnh viện qua đêm sau ca phẫu thuật này, mặc dù một số người có thể về nhà cùng ngày. Bạn cần có người ở lại bên cạnh trong 24 giờ đầu để hỗ trợ bạn. Bạn sẽ bắt đầu cử động các ngón tay nhẹ nhàng ngay lập tức. Bác sĩ phẫu thuật của bạn sẽ hướng dẫn bạn cách chăm sóc vết mổ và khi nào có thể bắt đầu sử dụng lại bàn tay.
Phục hồi¶
Sau phẫu thuật mở, bạn có thể sẽ cảm thấy đau và sưng ở cổ tay và bàn tay. Đây là điều bình thường khi cơ thể bạn đang hồi phục. Bác sĩ phẫu thuật của bạn sẽ hướng dẫn cách quản lý sự khó chịu này bằng thuốc và chườm đá. Bạn sẽ đeo nẹp hoặc bột bó để bảo vệ các xương đã được hợp nhất trong khi chúng liền lại.
Trong những ngày đầu, bạn sẽ giữ cánh tay của mình ở tư thế nâng cao để giảm sưng. Bạn sẽ sử dụng dây đeo tay (sling) để hỗ trợ khi di chuyển trong nhà. Các công việc đơn giản như ăn uống hoặc đánh răng vẫn có thể thực hiện được nếu cẩn thận. Chuyên viên vật lý trị liệu của bạn sẽ dạy bạn các bài tập nhẹ nhàng để giữ cho các ngón tay của bạn cử động và ngăn ngừa cứng khớp. Khi sưng giảm và khả năng vận động trở lại, bạn sẽ dần dần bắt đầu sử dụng bàn tay nhiều hơn.
Bác sĩ phẫu thuật và chuyên viên vật lý trị liệu sẽ hướng dẫn bạn khi nào nên ngừng sử dụng nẹp và cách tăng cường lực nắm. Thời gian phục hồi của bạn có thể khác với người khác; bác sĩ phẫu thuật và chuyên viên vật lý trị liệu sẽ hướng dẫn bạn dựa trên quá trình hồi phục của bạn. Bạn sẽ cảm thấy tự tin hơn khi cơn đau giảm dần và cổ tay của bạn trở nên ổn định.
Những biến chứng có thể xảy ra¶
Hầu hết bệnh nhân đều hồi phục tốt, nhưng đôi khi có thể xảy ra các vấn đề. Bác sĩ phẫu thuật và đội ngũ y tế sẽ theo dõi bạn chặt chẽ để phát hiện sớm bất kỳ vấn đề nào.
Đôi khi các xương không liền lại như dự kiến. Bạn có thể nhận thấy cơn đau sâu không giảm với các thuốc giảm đau thông thường hoặc cảm giác cổ tay vẫn còn không vững. Nếu điều này xảy ra, hãy gọi cho bác sĩ phẫu thuật để thảo luận về các bước tiếp theo.
Có một khả năng nhỏ là khớp có thể cần phải được cố định hoàn toàn (nối xương) sau này. Bạn có thể cảm thấy cứng khớp hoặc đau tăng dần, hoặc cơn đau quay trở lại sau một giai đoạn cải thiện. Bác sĩ phẫu thuật sẽ xem lại phim X-quang của bạn và trao đổi với bạn về việc chuyển sang phẫu thuật cố định toàn bộ cổ tay nếu cần thiết.
Trong một số trường hợp, ghép xương hoặc vít có thể không hoạt động như mong đợi. Bạn có thể cảm thấy có tiếng kêu lách cách hoặc cảm giác mài mòn ở cổ tay, hoặc nhận thấy sưng và đau tăng đột ngột. Hãy đề cập đến vấn đề này trong lần tái khám tiếp theo để bác sĩ phẫu thuật có thể kiểm tra các thiết bị cố định.
Nếu bạn có cấy ghép pyrocarbon, kết quả lâu dài có thể khó dự đoán. Bạn có thể trải qua tình trạng đau hoặc mất vận động theo thời gian. Nếu cấy ghép thất bại, phẫu thuật cố định xương vẫn là một lựa chọn để khắc phục vấn đề.
Bảng biến chứng trên trang này liệt kê các tỷ lệ điển hình nếu bạn muốn biết chi tiết.
Khi nào nên gọi cho chúng tôi¶
Gọi cho chúng tôi nếu bạn bị sốt, đỏ tăng dần hoặc có dịch tiết từ vết thương. Liên hệ ngay với bác sĩ phẫu thuật của bạn nếu bạn bị đau dữ dội đột ngột hoặc mất cảm giác ở bàn tay. Đến cơ sở cấp cứu nếu bạn nhận thấy sưng bắp chân hoặc khó thở. Những dấu hiệu này có thể cho thấy có cục máu đông hoặc nhiễm trùng cần được điều trị khẩn cấp.
Evidence & references
Overview¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- The use of a pyrocarbon capitate resurfacing implant may represent a good alternative to total and partial wrist arthrodesis [3].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up [4].
- There are no comparative series or randomized studies for the treatment of midcarpal instability [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- The reduction and association of the scaphoid and lunate procedure should be abandoned due to a majority of patients experiencing early radiographic failure in the short term [7].
- It is difficult to predict long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, but the outcome so far is encouraging [9].
- Conversion to midcarpal fusion remains a salvage option for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis [9].
- Radioscapholunate arthrodesis with compression screws and local autograft is an effective method to perform the procedure in appropriately selected patients with a preserved midcarpal joint [11].
- Radioscapholunate arthrodesis with compression screws and local autograft achieves a 100% union rate at mean follow-up of 12 months with no complications [11].
- Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions [13].
- The use of magnesium-based headless bone screws for partial wrist arthrodesis is not supported due to premature mechanical instability [15].
- Radial wrist hemiarthroplasty implants are not approved by the FDA for use in humans in the United States [23].
- Radial wrist hemiarthroplasty implants must be performed as off-label use with full patient understanding and appropriate institutional review board approval [23].
Anatomy & Pathophysiology¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- A dart-throwing motion (DTM) at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion [10].
- Surgical groups for scapholunate advanced collapse demonstrate decreased wrist kinematic motion and functional performance compared with individuals with normal wrists [16].
- Scaphoid nonunions partially uncouple the proximal and distal carpal rows [17].
- Computed fiber elongations of the dorsal carpal ligaments vary linearly with wrist position [29].
- During simple unresisted wrist motions, force in the scapholunate interosseous ligament does not exceed 20 N [30].
- Kinematic changes in scapholunate instability may predict the development of radioscaphoid arthritis [31].
- Comprehending carpal dysfunctions and instabilities hinges on understanding carpal anatomy and normal biomechanics [32].
- The distal carpal row has negligible intercarpal motion while the proximal row drives motion [33].
- More than half the motion of the carpus when the wrist was loaded in extension occurred at the midcarpal joint [34].
- Static imaging techniques may accurately depict major wrist ligamentous injury, while dynamic ultrasound and videofluoroscopy may demonstrate dynamic instability and kinematic dysfunction [35].
- A pattern of kinematic changes was established after scapholunate ligament injury despite individual variance [38].
- Accurate identification of carpal bone morphology is required to improve understanding of carpal mechanics and pathology [39].
- A wide range of dart-throwing motion planes exists [40].
- Midcarpal arthrodesis adversely affects dart-throwing motion compared with radiocarpal arthrodesis [40].
- During forearm rotation, the contact site of the scaphoid and the lunate on the distal radial articular surface changed minimally [41].
- Reconstruction of both volar and dorsal limbs of the scapholunate interosseous ligament aims to approximate original anatomy and restore normal carpal mechanics [42].
Classification¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- The use of a pyrocarbon capitate resurfacing implant may represent a good alternative to total and partial wrist arthrodesis [3].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up [4].
- There are no comparative series or randomized studies for midcarpal instability treatment options including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- Functional results were good at long-term follow-up for 4-corner fusion for SLAC and SNAC wrist despite radiographic changes in the radiolunate joint in 73% of patients [8].
- Scaphoid nonunions have a dramatic impact on carpal kinematics, partially uncoupling the proximal and distal carpal rows [17].
- Simulated radiocarpal fusion and simulated partial carpal fusion decreased range of motion compared with the intact wrist [53].
- The principal direction of wrist motion along the path of dart-thrower's motion was not significantly altered by simulated radiocarpal fusion or partial carpal fusion [53].
- The LFT and MFT demonstrate similar congruity to the proximal capitate in the sagittal and coronal planes of the wrist [56].
- Simulated radioscapholunate fusion confirmed the dart-thrower's hypothesis as wrist motion was primarily preserved from radial-extension toward ulnar-flexion [59].
- Midcarpal stabilisation and scaphoid and triquetrum excision retains most wrist motion [60].
Clinical Presentation¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- Treatment options for midcarpal instability include partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage [4].
- There are no comparative series or randomized studies regarding treatment options for midcarpal instability [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse [6].
- The reduction and association of the scaphoid and lunate procedure experiences early radiographic failure in the majority of patients in the short term [7].
- Functional results for 4-corner fusion for SLAC and SNAC wrist are good at long-term follow-up despite radiographic changes in the radiolunate joint in 73% of patients [8].
- It is difficult to predict long-term survival for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, though outcomes are currently encouraging [9].
- Conversion to midcarpal fusion remains a salvage option for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis [9].
- A dart-throwing motion (DTM) at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion [10].
- Lunate excision without midcarpal fusion resulted in a disease-free state with good painless range of motion at 6 years [12].
- Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions [13].
- Radiographic carpal collapse and ulnar translocation occurred in scaphocapitate arthrodesis for Kienböck disease, but patients were not symptomatic [19].
- From an 8- to 11-year perspective, patients with distal scaphoid fractures report normal self-assessed hand function as well as good wrist motion and strength [20].
- Parallel K-wire placement across the midcarpal joints with scaphoid leads to a high rate of fusion with good patient outcomes long term [21].
- Ulnar-sided wrist pain is a common cause of upper extremity disability with a complex differential diagnosis [43].
- Both trigger wrist and avascular necrosis of the capitate are rare disorders [49].
- Excision arthroplasty for scapho-trapezial-trapezoid (STT) arthritis can provoke severe malalignment and midcarpal instability [50].
- Midcarpal instability following excision arthroplasty for STT arthritis can lead to an intercarpal arthrodesis with an outcome potentially worse than STT fusion [50].
Investigations¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up [4].
- There are no comparative series or randomized studies regarding treatment options for midcarpal instability [4].
- A dynamic CT scan of the wrist is a user-friendly way of measuring the scapholunate distance, which is minimal in the normal wrist below 40 years of age [57].
- Measurements in the middle of the scapholunate joint in neutral and 30° of ulnar deviation under fluoroscopic imaging best capture all stages of ligamentous disruptions [63].
- Plain radiographs, CT, 3D-CT, and MRI are suboptimal modalities to assess capitate type [64].
- A scaphoid fracture was by far the most common injury in patients with posttraumatic radial wrist tenderness, but it is not clear whether diagnosis of subtle injuries only demonstrated on MRI improves outcomes [62].
- Delayed diagnosis and late reconstructive surgery for traumatic nondissociative carpal instability were associated with no improvement in radiolunate angle [58].
- Delayed diagnosis of intercarpal injuries can result in persistent median nerve dysfunction [27].
Treatment¶
- Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- The use of a pyrocarbon capitate resurfacing implant may represent a good alternative to total and partial wrist arthrodesis [3].
- Treatment options for midcarpal instability including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up, but there are no comparative series or randomized studies [4].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- The reduction and association of the scaphoid and lunate procedure should be abandoned due to a majority of patients experiencing early radiographic failure in the short term [7].
- It is difficult to predict long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, but the outcome so far is encouraging, and conversion to midcarpal fusion remains a salvage option [9].
- Radioscapholunate arthrodesis with compression screws and local autograft is an effective method in appropriately selected patients with a preserved midcarpal joint, achieving a 100% union rate at mean follow-up of 12 months with no complications [11].
- Lunate excision without midcarpal fusion resulted in a disease-free state with good painless range of motion at 6 years, avoiding the recurrence associated with curettage and the motion loss associated with fusion [12].
- Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions [13].
- The results after total wrist joint arthroplasty vary probably as the result of different patient groups, implant types and evolution of prosthetic designs, and are not comparable with the present study [14].
- The authors cannot support the use of magnesium-based screws for partial wrist arthrodesis due to premature mechanical instability [15].
- Load is preferentially transferred to the radiolunate joint after scaphoid excision with four-corner fusion [22].
- Radial wrist hemiarthroplasty implants are not approved by the FDA for use in humans in the United States and must be performed as off-label use with full patient understanding and appropriate institutional review board approval [23].
- Arthroscopic resection of the proximal capitate with tendon interposition for isolated capitolunate osteoarthritis does not preclude the possibility of secondary arthrodesis in case of failure [24].
- Better results were seen when arthrodesis fused in cases of avascular necrosis of the capitate [25].
- The technique of wrist arthrodesis combining proximal row carpectomy and rigid internal fixation has proved to be a highly predictable operation with much less morbidity and fewer complications than with older techniques using distant bone graft [48].
- Radiocarpal fusion aims to alleviate pain and improve range of motion in patients with isolated radiolunate or radioscapholunate arthritis who have failed non-surgical treatment [51].
- Pyrocarbon interposition arthroplasty is an alternative to total wrist arthrodesis when marked degenerative changes exist at the radiolunate joint, capitate head or both, and increases operative options for challenging clinical scenarios [52].
- Locking screws are important in improving the longevity of total wrist arthroplasty by imitating external or internal fixation for bridging large bony defects, allowing the carpal component to remain stable despite complete asymptomatic avascular bone necrosis around the capitate peg [55].
- Arthroscopic interposition tendon arthroplasty for stage 2 scapholunate advanced collapse preserves motion, yields acceptable functional outcome, and reduces pain [61].
- Arthroscopic partial capitate resection for type Ia avascular necrosis provided adequate pain relief and improved the range of wrist motion and grip strength during short-term follow-up [67].
Complications¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients receiving vascularized bone graft with capitate shortening and radial shortening [2].
- Treatment options for midcarpal instability, including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage, are described in small case series with limited follow-up without comparative series or randomized studies [4].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse [6].
- The reduction and association of the scaphoid and lunate procedure experiences early radiographic failure in the majority of patients in the short term [7].
- Radiographic changes in the radiolunate joint occur in 73% of patients at long-term follow-up despite good functional results after 4-corner fusion for SLAC and SNAC wrist [8].
- Long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis is difficult to predict, though conversion to midcarpal fusion remains a salvage option [9].
- Radioscapholunate arthrodesis with compression screws and local autograft achieves a 100% union rate at a mean follow-up of 12 months with no complications in appropriately selected patients [11].
- Magnesium-based headless bone screws can result in premature mechanical instability and implant failure in partial wrist fusion [15].
- Parallel K-wire placement across the midcarpal joints with scaphoid leads to a high rate of fusion with good long-term patient outcomes [21].
- Arthroscopic resection of the proximal capitate with tendon interposition does not preclude the possibility of secondary arthrodesis in case of failure [24].
- While some intercarpal arthrodeses yield good, predictable outcomes, others are infrequently used due to unpredictable results and high complication rates [68].
- Wrist fusion rates are higher in the 4-corner fusion group compared to proximal row carpectomy without a significant difference in readmission rates [70].
- Conversion rates to total wrist arthrodesis are significantly higher with partial wrist arthrodesis (19.2%) than with proximal row carpectomy (4.9%) [71].
- Partial wrist arthrodesis has a greater associated direct cost than proximal row carpectomy [71].
- High complication rates following four-corner arthrodesis with a nonlocking plate have led to the recommendation for fixation with a locking screw plate [74].
Recovery¶
- Resection of over 25% of the scaphoid induces instability and unpredictable kinematics [1].
- Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening [2].
- Pyrocarbon capitate resurfacing may represent a good alternative to total and partial wrist arthrodesis [3].
- Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time [5].
- There is a low rate of conversion to total wrist arthrodesis following scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years [6].
- The reduction and association of the scaphoid and lunate procedure should be abandoned due to a majority of patients experiencing early radiographic failure in the short term [7].
- Functional results were good at long-term follow-up for 4-corner fusion for SLAC and SNAC wrist despite radiographic changes in the radiolunate joint in 73% of patients [8].
- It is difficult to predict long-term survival of pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis, but the outcome so far is encouraging [9].
- Conversion to midcarpal fusion remains a salvage option for pyrocarbon interposition arthroplasty for proximal capitate avascular necrosis [9].
- A dart-throwing motion at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion [10].
- Both surgical groups demonstrated decreased wrist kinematic motion and functional performance compared with individuals with normal wrists [16].
- Further studies need to be performed to address differences in anatomy and wrist movement among patients with different lunate shapes regarding the dart-splint [18].
- From an 8- to 11-year perspective, patients with distal scaphoid fractures report normal self-assessed hand function as well as good wrist motion and strength [20].
- Delayed diagnosis of intercarpal injuries can result in persistent median nerve dysfunction [27].
- Research underscores the importance of considering forearm rotation when developing rehabilitation protocols for scapholunate joint instability [44].
- Radiocapitate range of motion after proximal row carpectomy was sufficient for activities of daily living [45].
- A patient with complex carpal dissociation regained satisfactory function and returned to work at six months with stable carpus on radiographs [46].
- Multicomponent exercise is important in the treatment of wrist instability [47].
- Four-corner bone wrist arthrodesis by dorsal rectangular plating achieves an acceptable preservation of range of motion with good pain relief, an excellent consolidation rate and minimal complications [66].
Key Evidence¶
- [L5] Resection of over 25% of the scaphoid should be avoided or supplemented with partial wrist fusion due to induced instability and unpredictable kinematics. [1] (10.1177/1558944720966717)
- [L4] Fusion of the proximal carpals developed in 3 of 7 patients who received vascularized bone graft with capitate shortening and radial shortening. [2] (10.1016/j.jhsg.2019.09.012)
- [L4] This surgical procedure may represent a good alternative to total and partial wrist arthrodesis. [3] (10.1177/1753193413501730)
- [L5] Treatment options including partial wrist fusions, tenodesis stabilizations, and arthroscopic capsular shrinkage have been described in small case series with limited follow-up, but there are no comparative series or randomized studies. [4] (10.1177/1753193415617756)
- [L4] Scaphoid excision and four-corner fusion remains a viable option for patients with advanced wrist arthritis with reliable, resilient functional results that remain stable over time. [5] (10.1016/j.jhsa.2014.06.118)
- [L4] There is a low rate of conversion to total wrist arthrodesis. [6] (10.1016/j.jhsa.2010.01.025)
- [L4] With a majority of patients experiencing early radiographic failure of the procedure in the short term, our experience suggests that the reduction and association of the scaphoid and lunate procedure should be abandoned despite the relatively low outcomes measures scores. [7] (10.1016/j.jhsa.2014.07.014)
- [L4] Functional results were good at long-term follow-up despite radiographic changes in the radiolunate joint in 73% of patients. [8] (10.1177/1558944716681949)
- [L5] It is difficult to predict long-term survival, but the outcome so far is encouraging, and conversion to midcarpal fusion remains a salvage option. [9] (10.1007/s11552-014-9698-7)
- [L5] Clinically, a DTM at approximately 30° to 45° from the sagittal plane allows continued functional wrist motion while minimizing radiocarpal motion. [10] (10.1016/j.jhsa.2007.08.014)
- [L4] This technique is an effective method to perform radioscapholunate arthrodesis in appropriately selected patients with a preserved midcarpal joint, achieving a 100% union rate at mean follow-up of 12 months with no complications. [11] (10.1016/j.jhsa.2013.01.026)
- [L4] Lunate excision without midcarpal fusion resulted in a disease-free state with good painless range of motion at 6 years, avoiding the recurrence associated with curettage and the motion loss associated with fusion. [12] (10.1177/1753193413488303)
- [L4] Scaphoidectomy and midcarpal fusion is a useful salvage procedure in a variety of degenerative conditions. [13] (10.1177/1753193410395357)
- [L4] The results after total wrist joint arthroplasty vary probably as the result of different patient groups, implant types and evolution of prosthetic designs, and are not comparable with the present study. [14] (10.1186/s12891-018-2172-x)
- [Case_report] Due to this disappointing result of the operation with premature mechanical instability, the authors cannot support the use of magnesium-based screws for partial wrist arthrodesis, at least not in dual use. [15] (10.1155/2016/7049130)
- [L2] Both surgical groups demonstrated decreased wrist kinematic motion and functional performance compared with individuals with normal wrists. [16] (10.1016/j.jhsa.2015.04.035)
- [L4] Scaphoid nonunions have a dramatic impact on carpal kinematics, partially uncoupling the proximal and distal carpal rows. [17] (10.1016/j.jhsa.2008.03.008)
- [L5] Further studies need to be performed to address differences in anatomy and wrist movement among patients with different lunate shapes. [18] (10.1016/j.jht.2015.01.007)
- [L4] Although radiographic carpal collapse and ulnar translocation occurred, patients were not symptomatic. [19] (10.1016/j.jhsa.2014.12.013)
- [L2] From an 8- to 11-year perspective, patients with distal scaphoid fractures report normal self-assessed hand function as well as good wrist motion and strength. [20] (10.1016/j.jhsa.2017.06.016)
- [L4] Parallel K-wire placement across the midcarpal joints with scaphoid leads to a high rate of fusion with good patient outcomes long term. [21] (10.1177/15589447211057302)
- [L5] Our findings suggest that load is preferentially transferred to the radiolunate joint after scaphoid excision with four-corner fusion. [22] (10.1007/s11552-007-9048-0)
- [L5] Radial wrist hemiarthroplasty implants are not approved by the FDA for use in humans in the United States and must be performed as off-label use with full patient understanding and appropriate institutional review board approval. [23] (10.1016/j.jhsa.2012.10.050)
- [L4] This approach does not preclude the possibility of secondary arthrodesis in case of failure. [24] (10.1016/j.jhsa.2025.06.004)
- [L4] Better results were seen when the arthrodesis fused. [25] (10.1177/1753193414524876)
- [Case_report] This case illustrates the importance of careful review of radiographs for evidence of intercarpal injuries, as delayed diagnosis resulted in persistent median nerve dysfunction. [27] (10.1007/s11552-013-9545-2)
- [L5] Despite complex carpal bone anatomy and kinematics, computed fiber elongations were found to vary linearly with wrist position. [29] (10.1016/j.jhsa.2012.04.025)
- [L5] However, during simple unresisted wrist motions, the force did not exceed 20 N. [30] (10.1016/j.jhsa.2015.04.007)
- [L3] These kinematic changes may predict the development of radioscaphoid arthritis and help identify a kinematically abnormal wrist. [31] (10.1177/17531934241242676)
- [L4] Comprehending carpal dysfunctions and instabilities hinges on understanding carpal anatomy and normal biomechanics. [32] (10.1016/j.jht.2023.09.011)
- [L5] Advances in 3-dimensional and 4-dimensional imaging have provided clearer insight into carpal kinematics, establishing that the distal carpal row has negligible intercarpal motion while the proximal row drives motion. [33] (10.1016/j.jhsa.2016.07.105)
- [L4] More than half the motion of the carpus when the wrist was loaded in extension occurred at the midcarpal joint. [34] (10.1016/j.jhsa.2012.10.035)
- [L4] Static imaging techniques may accurately depict major wrist ligamentous injury, while dynamic ultrasound and videofluoroscopy may demonstrate dynamic instability and kinematic dysfunction. [35] (10.1177/1753193415610515)
- [L5] Despite individual variance, a pattern of kinematic changes was established after scapholunate ligament injury. [38] (10.1177/1753193415600669)
- [L5] Accurate identification of carpal bone morphology is required to improve our understanding of carpal mechanics and pathology. [39] (10.1016/j.jhsa.2009.03.002)
- [L5] This report updates information on wrist dart-throwing motion based on recent research regarding its kinematics, kinetics, and clinical applications, noting that a wide range of DT planes exists and that midcarpal arthrodesis adversely affects DT motion compared with radiocarpal arthrodesis. [40] (10.1016/j.jhsa.2014.02.035)
- [L5] During forearm rotation, the contact site of the scaphoid and the lunate on the distal radial articular surface changed minimally. [41] (10.1016/j.jhsa.2013.01.021)
- [L4] The technique aims to approximate the original anatomy and restore normal carpal mechanics to prevent progression to scapholunate advanced collapse arthritis. [42] (10.1016/j.jhsa.2013.05.026)
- [L5] Ulnar-sided wrist pain is a common cause of upper extremity disability with a complex differential diagnosis. [43] (10.1016/j.jhsa.2012.04.036)
- [L5] This research underscores the importance of considering forearm rotation when developing rehabilitation protocols for scapholunate joint instability and provides a valuable perspective in line with current rehabilitation principles. [44] (10.1016/j.jht.2023.09.012)
- [L5] Radiocapitate range of motion after PRC was sufficient for activities of daily living. [45] (10.1016/j.jhsa.2006.10.014)
- [Case_report] The patient regained satisfactory function and returned to work at six months with stable carpus on radiographs. [46] (10.1016/j.jhsa.2007.07.025)
- [L4] These results highlight the importance of multicomponent exercise in the treatment of wrist instability. [47] (10.1016/j.jht.2023.08.010)
- [L4] This technique of wrist arthrodesis combining proximal row carpectomy and rigid internal fixation has proved to be a highly predictable operation with much less morbidity and fewer complications than with older techniques using distant bone graft. [48] (10.1016/j.jhsa.2012.11.010)
- [Case_report] Both trigger wrist and avascular necrosis of the capitate are rare disorders. [49] (10.1186/s12891-018-2010-1)
- [L4] The procedure can provoke severe malalignment and midcarpal instability, leading to an intercarpal arthrodesis with an outcome potentially worse than STT fusion. [50] (10.1177/1753193408098903)
- [L5] The procedure aims to alleviate pain and improve range of motion in patients with isolated radiolunate or radioscapholunate arthritis who have failed non-surgical treatment. [51] (10.1016/j.jhsa.2022.04.002)
- [L4] Pyrocarbon interposition arthroplasty is an alternative to total wrist arthrodesis when marked degenerative changes exist at the radiolunate joint, capitate head or both, and increases operative options for challenging clinical scenarios. [52] (10.1177/1753193417714400)
- [L5] Although both simulated fusion types decreased ROM compared with the intact wrist, the principal direction of wrist motion along the path of DTM was not significantly altered by simulated RCF or PCF. [53] (10.1016/j.jhsa.2017.10.017)
- [L4] The case highlights the importance of locking screws in improving the longevity of total wrist arthroplasty by imitating external or internal fixation for bridging large bony defects, allowing the carpal component to remain stable despite complete asymptomatic avascular bone necrosis around the capitate peg. [55] (10.1016/j.jhsg.2024.01.002)
- [L4] The LFT and MFT demonstrate similar congruity to the proximal capitate in the sagittal and coronal planes of the wrist. [56] (10.1016/j.jhsa.2022.04.015)
- [L4] This novel dynamic CT scan of the wrist is a user-friendly way of measuring the scapholunate distance, which is minimal in the normal wrist below 40 years of age. [57] (10.1177/1558944717726372)
- [L4] Delayed diagnosis and late reconstructive surgery were associated with no improvement in radiolunate angle. [58] (10.1016/j.jhsa.2021.04.024)
- [L5] The fusion model confirmed the dart-thrower's hypothesis as wrist motion was primarily preserved from radial-extension toward ulnar-flexion. [59] (10.1016/j.jhsa.2007.12.013)
- [L5] Results suggest that midcarpal stabilisation and scaphoid and triquetrum excision retains most wrist motion. [60] (10.1177/1753193408094923)
- [L4] This procedure preserves motion, yields acceptable functional outcome, and reduces pain. [61] (10.1016/j.arthro.2018.10.134)
- [L2] A scaphoid fracture was by far the most common injury, but it is not clear whether diagnosis of subtle injuries only demonstrated on MRI improves outcomes. [62] (10.1016/j.jhsa.2012.09.034)
- [L5] Measurements in the middle of the scapholunate joint in neutral and 30° of ulnar deviation under fluoroscopic imaging best capture all stages of ligamentous disruptions. [63] (10.1177/1558944717729219)
- [L4] Plain radiographs, CT, 3D-CT, and MRI are suboptimal modalities to assess capitate type. [64] (10.1007/s11552-015-9743-1)
- [L4] Four-corner bone wrist arthrodesis by dorsal rectangular plating achieves an acceptable preservation of range of motion with good pain relief, an excellent consolidation rate and minimal complications. [66] (10.1177/1753193409105684)
- [L4] It provided adequate pain relief and improved the range of wrist motion and grip strength during short-term follow-up. [67] (10.1016/j.jhsa.2015.09.010)
- [L5] While some procedures yield good, predictable outcomes, others are infrequently used due to unpredictable results and high complication rates. [68] (10.1016/j.jhsa.2013.09.014)
- [L3] Wrist fusion rates and average costs are higher in the 4CF group without a significant difference in readmission rates. [70] (10.1016/j.jhsa.2019.12.010)
- [L3] Conversion rates to total wrist arthrodesis are significantly higher with PWA (19.2%) than with PRC (4.9%) and have a greater associated direct cost. [71] (10.1016/j.jhsa.2017.07.032)
- [L4] Based on the high complication rate following FCA with a nonlocking plate, the authors no longer use this implant and recommend fixation with a locking screw plate. [74] (10.1016/j.jhsa.2017.10.036)
References¶
[1] How Much Scaphoid Can be Safely Resected? A Biomechanical Analysis of the Effects of Distal Scaphoid Resection. HAND. 2020. DOI: 10.1177/1558944720966717 [2] Vascularized Bone Graft to the Lunate Combined with Shortening of the Capitate and Radius for Treatment of Advanced Kienböck Disease After a Follow-Up for More Than 10 Years. Journal of Hand Surgery Global Online. 2020. DOI: 10.1016/j.jhsg.2019.09.012 [3] The use of a pyrocarbon capitate resurfacing implant in chronic wrist disorders. Journal of Hand Surgery (European Volume). 2013. DOI: 10.1177/1753193413501730 [4] Midcarpal instability. Journal of Hand Surgery (European Volume). 2015. DOI: 10.1177/1753193415617756 [5] Resilience of SLAC 4-Corner Fusion: Long-Term Follow-Up. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2014.06.118 [6] The Outcome of Scaphoid Excision and Four-Corner Arthrodesis for Advanced Carpal Collapse at a Minimum of Ten Years. The Journal of Hand Surgery. 2010. DOI: 10.1016/j.jhsa.2010.01.025 [7] Reduction and Association of the Scaphoid and Lunate Procedure: Short-Term Clinical and Radiographic Outcomes. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2014.07.014 [8] Ten-Year Minimum Follow-Up of 4-Corner Fusion for SLAC and SNAC Wrist. HAND. 2016. DOI: 10.1177/1558944716681949 [9] Pyrocarbon Interposition Arthroplasty for Proximal Capitate Avascular Necrosis. HAND. 2014. DOI: 10.1007/s11552-014-9698-7 [10] 2007 IFSSH Committee Report of Wrist Biomechanics Committee: Biomechanics of the So-Called Dart-Throwing Motion of the Wrist. The Journal of Hand Surgery. 2007. DOI: 10.1016/j.jhsa.2007.08.014 [11] Radioscapholunate Arthrodesis With Compression Screws and Local Autograft. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.01.026 [12] Three-dimensional analysis of the proximal articulating surfaces of the lunate and capitate. Journal of Hand Surgery (European Volume). 2013. DOI: 10.1177/1753193413488303 [13] A new plate for partial wrist fusions: results in midcarpal arthrodesis. Journal of Hand Surgery (European Volume). 2011. DOI: 10.1177/1753193410395357 [14] Radiocarpal fusion and midcarpal resection interposition arthroplasty: long-term results in severely destroyed rheumatoid wrists. BMC Musculoskeletal Disorders. 2018. DOI: 10.1186/s12891-018-2172-x [15] A Case of Implant Failure in Partial Wrist Fusion Applying Magnesium-Based Headless Bone Screws. Case Reports in Orthopedics. 2016. DOI: 10.1155/2016/7049130 [16] Surgical Treatments for Scapholunate Advanced Collapse Wrist: Kinematics and Functional Performance. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2015.04.035 [17] Interfragmentary Motion in Patients With Scaphoid Nonunion. The Journal of Hand Surgery. 2008. DOI: 10.1016/j.jhsa.2008.03.008 [18] Dart-Splint: An innovative orthosis that can be integrated into a scapho-lunate and palmar midcarpal instability re-education protocol. Journal of Hand Therapy. 2015. DOI: 10.1016/j.jht.2015.01.007 [19] Scaphocapitate Arthrodesis for Kienböck Disease. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2014.12.013 [20] Long-Term Outcomes After Distal Scaphoid Fractures: A 10-Year Follow-Up. The Journal of Hand Surgery. 2017. DOI: 10.1016/j.jhsa.2017.06.016 [21] Parallel K-Wire Placement Leads to Fusion and Midcarpal Settling in Scaphoid Excision Four-Corner Fusion. HAND. 2021. DOI: 10.1177/15589447211057302 [22] Scaphoid Excision with Four-Corner Fusion: A Biomechanical Study. HAND. 2007. DOI: 10.1007/s11552-007-9048-0 [23] “Off-Label” Use of Orthopedic Implants in the Wrist. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.10.050 [24] Arthroscopic Resection of the Proximal Capitate With Tendon Interposition for Isolated Capitolunate Osteoarthritis: A Retrospective Series of Six Cases. The Journal of Hand Surgery. 2026. DOI: 10.1016/j.jhsa.2025.06.004 [25] Avascular necrosis of the capitate: report of six cases and review of the literature. Journal of Hand Surgery (European Volume). 2014. DOI: 10.1177/1753193414524876 [27] Volar Capitate Dislocation: A Case Report. HAND. 2013. DOI: 10.1007/s11552-013-9545-2 [29] Elongation of the Dorsal Carpal Ligaments: A Computational Study of In Vivo Carpal Kinematics. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.04.025 [30] Force in the Scapholunate Interosseous Ligament During Active Wrist Motion. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2015.04.007 [31] Radiocarpal and midcarpal kinematics in scapholunate instability: a four-dimensional CT study in vivo. Journal of Hand Surgery (European Volume). 2024. DOI: 10.1177/17531934241242676 [32] Scapholunate and lunotriquetral joint dynamic stabilizers and their role in wrist neuromuscular control and proprioception. Journal of Hand Therapy. 2024. DOI: 10.1016/j.jht.2023.09.011 [33] Carpal Kinematics and Kinetics. The Journal of Hand Surgery. 2016. DOI: 10.1016/j.jhsa.2016.07.105 [34] In Vivo Kinematics of the Scaphoid, Lunate, Capitate, and Third Metacarpal in Extreme Wrist Flexion and Extension. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.10.035 [35] Imaging in carpal instability. Journal of Hand Surgery (European Volume). 2015. DOI: 10.1177/1753193415610515 [38] Impact of scapholunate dissociation on human wrist kinematics. Journal of Hand Surgery (European Volume). 2015. DOI: 10.1177/1753193415600669 [39] Imaging Recognition of Morphological Variants at the Midcarpal Joint. The Journal of Hand Surgery. 2009. DOI: 10.1016/j.jhsa.2009.03.002 [40] International Federation of Societies for Surgery of the Hand 2013 Committee's Report on Wrist Dart-Throwing Motion. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2014.02.035 [41] Changes in Contact Site of the Radiocarpal Joint and Lengths of the Carpal Ligaments in Forearm Rotation: An In Vivo Study. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.01.021 [42] Reconstruction of Both Volar and Dorsal Limbs of the Scapholunate Interosseous Ligament. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2013.05.026 [43] Ulnar-sided Wrist Pain: Evaluation and Treatment of Triangular Fibrocartilage Complex Tears, Ulnocarpal Impaction Syndrome, and Lunotriquetral Ligament Tears. The Journal of Hand Surgery. 2012. DOI: 10.1016/j.jhsa.2012.04.036 [44] Influence of forearm rotation on the kinetic stabilizing efficiency of the muscles that control the scapholunate joint. Clinical application in proprioceptive and neuromuscular rehabilitation programs. Journal of Hand Therapy. 2024. DOI: 10.1016/j.jht.2023.09.012 [45] Carpal Kinematics After Proximal Row Carpectomy. The Journal of Hand Surgery. 2007. DOI: 10.1016/j.jhsa.2006.10.014 [46] Complex Carpal Dissociation With Open, Complete, and Divergent Trapezium, Capitate, and Hamate Dislocation: A Case Report. The Journal of Hand Surgery. 2007. DOI: 10.1016/j.jhsa.2007.07.025 [47] Exercise-based intervention as a nonsurgical treatment for patients with carpal instability: A case series. Journal of Hand Therapy. 2024. DOI: 10.1016/j.jht.2023.08.010 [48] Modified AO Arthrodesis of the Wrist (With Proximal Row Carpectomy). The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.11.010 [49] Trigger wrist caused by avascular necrosis of the capitate: a case report. BMC Musculoskeletal Disorders. 2018. DOI: 10.1186/s12891-018-2010-1 [50] Midcarpal instability after excision arthroplasty for scapho-trapezial-trapezoid (STT) arthritis. Journal of Hand Surgery (European Volume). 2009. DOI: 10.1177/1753193408098903 [51] Radiocarpal Fusion: Indications, Technique, and Modifications. The Journal of Hand Surgery. 2022. DOI: 10.1016/j.jhsa.2022.04.002 [52] Vascular anatomy of the capitate determined by micro-computed tomography angiography. Journal of Hand Surgery (European Volume). 2017. DOI: 10.1177/1753193417714400 [53] Relative Contributions of the Midcarpal and Radiocarpal Joints to Dart-Thrower’s Motion at the Wrist. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2017.10.017 [55] The Crucial Role of Locking Screws in Total Wrist Arthroplasty: Should We Always Revise or Not?. Journal of Hand Surgery Global Online. 2024. DOI: 10.1016/j.jhsg.2024.01.002 [56] Lateral Femoral Trochlea Flap Reconstruction of the Proximal Capitate: An Assessment of Congruity and Description of Technique. The Journal of Hand Surgery. 2023. DOI: 10.1016/j.jhsa.2022.04.015 [57] Dynamic CT Scan of the Normal Scapholunate Joint in a Clenched Fist and Radial and Ulnar Deviation. HAND. 2017. DOI: 10.1177/1558944717726372 [58] Traumatic Nondissociative Carpal Instability: A Case Series. The Journal of Hand Surgery. 2022. DOI: 10.1016/j.jhsa.2021.04.024 [59] Simulated Radioscapholunate Fusion Alters Carpal Kinematics While Preserving Dart-Thrower's Motion. The Journal of Hand Surgery. 2008. DOI: 10.1016/j.jhsa.2007.12.013 [60] Effect of scaphoid and triquetrum excision after limited stabilisation on cadaver wrist movement. Journal of Hand Surgery (European Volume). 2009. DOI: 10.1177/1753193408094923 [61] Arthroscopic Interposition Tendon Arthroplasty for Stage 2 Scapholunate Advanced Collapse. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2018.10.134 [62] The Benefit of Magnetic Resonance Imaging for Patients With Posttraumatic Radial Wrist Tenderness. The Journal of Hand Surgery. 2013. DOI: 10.1016/j.jhsa.2012.09.034 [63] The Optimal Location to Measure Scapholunate Diastasis on Screening Radiographs. HAND. 2017. DOI: 10.1177/1558944717729219 [64] Common Radiographic Imaging Modalities Fail to Accurately Predict Capitate Morphology. HAND. 2015. DOI: 10.1007/s11552-015-9743-1 [66] Four-corner bone arthrodesis with dorsal rectangular plate: series and personal technique. Journal of Hand Surgery (European Volume). 2009. DOI: 10.1177/1753193409105684 [67] Arthroscopic Partial Capitate Resection for Type Ia Avascular Necrosis: A Short-Term Outcome Analysis. The Journal of Hand Surgery. 2015. DOI: 10.1016/j.jhsa.2015.09.010 [68] Intercarpal Arthrodeses. The Journal of Hand Surgery. 2014. DOI: 10.1016/j.jhsa.2013.09.014 [70] Proximal Row Carpectomy Versus 4-Corner Fusion: Incidence, Conversion to Fusion, and Cost. The Journal of Hand Surgery. 2020. DOI: 10.1016/j.jhsa.2019.12.010 [71] A Comparative Analysis of Resource Utilization Between Proximal Row Carpectomy and Partial Wrist Fusion: A Population Study. The Journal of Hand Surgery. 2017. DOI: 10.1016/j.jhsa.2017.07.032 [74] Treatment Outcomes of 4-Corner Arthrodesis for Patients With Advanced Carpal Collapse: An Average of 4 Years’ Follow-Up Comparing 2 Different Plate Types. The Journal of Hand Surgery. 2018. DOI: 10.1016/j.jhsa.2017.10.036