Patients › Rehabilitation
Calcific Tendinitis
Recovery after arthroscopic excision of a calcific deposit, from early movement to full activity.

This protocol covers the rehabilitation after arthroscopic excision of a calcific deposit with Dr Kieran Hirpara at Mater Private Hospital Rockhampton: keyhole surgery to remove the calcium deposit from the rotator cuff tendon, sometimes combined with a subacromial decompression to make more room for the tendon. Bring this page or its PDF to your first physiotherapy visit so your rehabilitation stays coordinated. Your rehabilitation is progressed individually by your physiotherapist through the phases below, depending on how your shoulder progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
If removing the deposit required a rotator cuff repair (the deposit sometimes leaves a defect in the tendon that needs to be stitched closed), your recovery follows rotator cuff repair rules instead, and the rotator cuff repair protocol takes priority over this page. Dr Hirpara will tell you after the operation if this applies to you.
What to expect¶
Both pathways are early-movement pathways. Unless the rotator cuff needed a repair, nothing has been stitched that needs months of protection; the aim of treatment is to remove the source of pain, and the aim of rehabilitation is to settle the post-treatment flare, keep the shoulder moving so it does not stiffen, and then rebuild strength.
- After arthroscopic excision a sling is provided for comfort only. It is worn briefly, typically days and rarely beyond two weeks, and should be left off as much as possible. You do not need to sleep in it. Recovery to full, unrestricted activity typically takes around three months.
Do not drive for at least six weeks after any shoulder operation, even once the sling is gone; your surgeon will clear you to drive, typically at the six-week review.
With either treatment, the shoulder can take time to settle completely. Discomfort often improves in stages rather than all at once, and after surgery it can take several months (occasionally up to nine) for the pre-treatment symptoms to fade fully. Steady improvement, not instant comfort, is the expected pattern.
This is keyhole day surgery through several small incisions. The calcific deposit is located within the rotator cuff tendon and removed, and a subacromial decompression is often performed at the same time to give the tendon more room. The dressings are waterproof — you can shower over them from day 1 — and stay on until your wounds are checked at your first post-operative appointment about a week to ten days after surgery.
Phase I — Early movement (weeks 0–2)¶
Kieran Hirpara 4.0
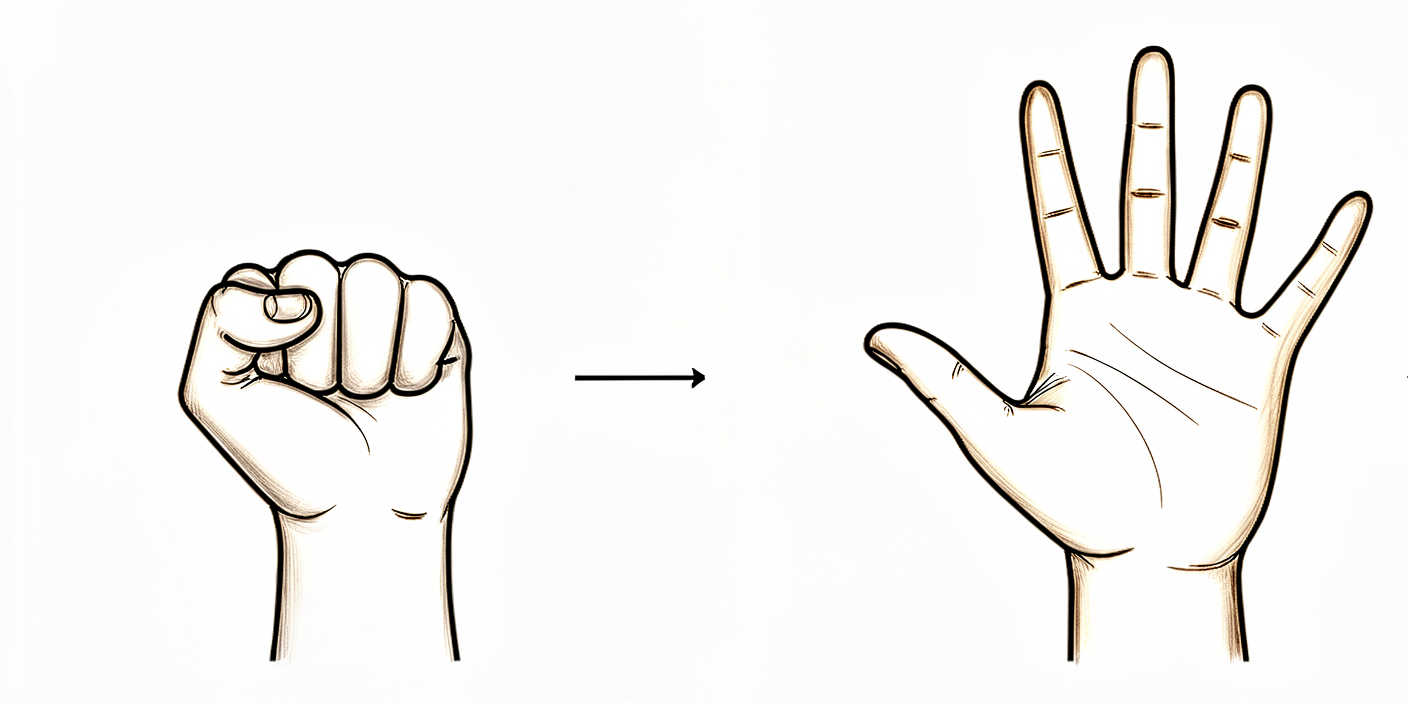
Open and close hand
Keep your hand and fingers moving by opening and closing them, or by squeezing a soft ball. Start this straight away to keep the hand and arm working while the shoulder settles.
10 times, three times a day
Kieran Hirpara 4.0
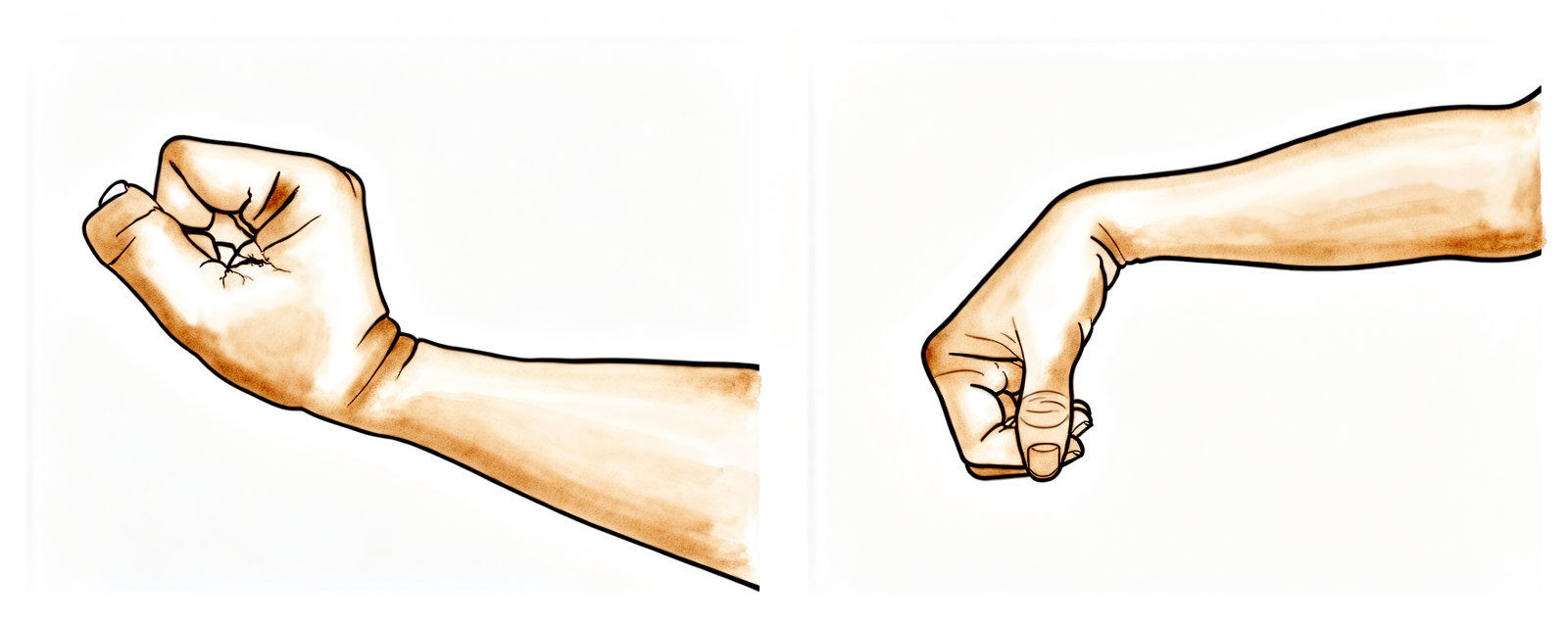
Wrist movement
Keep your wrist moving by bending it forwards, backwards and side to side. Do this with the arm out of the sling.
10 times, three times a day

Kieran Hirpara 4.0
Elbow bends
With the upper arm resting by your side, bend the elbow as far as it comfortably goes, then straighten it fully. Only the elbow moves — keep the shoulder relaxed.
10 times, three times a day
Kieran Hirpara 4.0
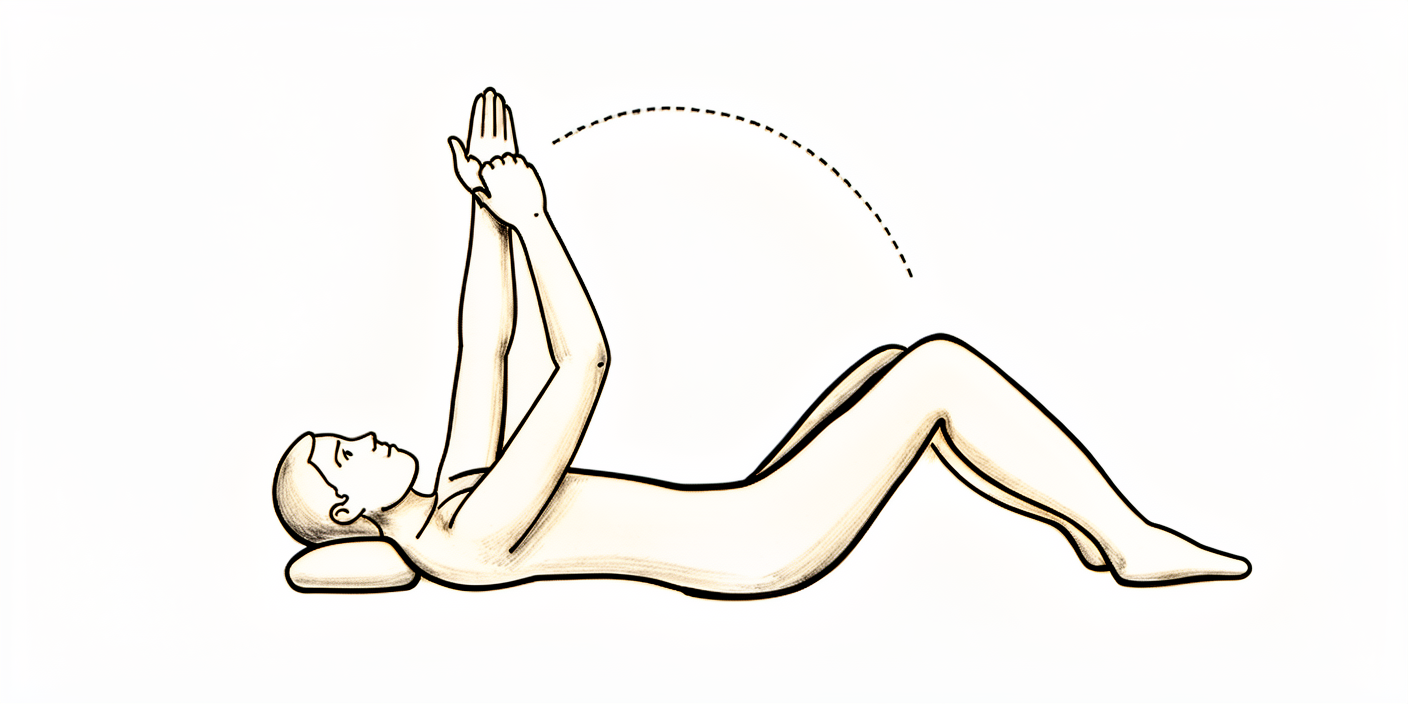
Assisted overhead stretch (lying)
Lie on your back and use your good arm to help lift the operated arm up above shoulder height as a gentle stretch, then lower it back down with the good arm still helping. It will be uncomfortable at first — that is expected — and it is the key exercise for stopping the shoulder stiffening.
10 repetitions, three times a day
You will wake from surgery with your arm in a sling, but the sling is for comfort only: try to do without it as much as you can, and most people are out of it within days. You can use the arm without restriction below shoulder height from the start. Lifting the arm above shoulder height is allowed and safe, although it will be uncomfortable at first; several times a day, use your good arm to help lift the operated arm above shoulder height as a gentle stretch, so the shoulder does not stiffen. Avoid carrying anything heavier than about two kilograms with the operated arm in these first weeks, as this will be painful. Start your exercises as soon as possible, aiming for ten repetitions of each, three times a day. Take pain relief before your exercises, and use ice for comfort. Do not drive: driving resumes only after your surgeon clears you, typically at the six-week review.
For your physiotherapist:
Goals
- Settle post-operative pain and swelling
- Early restoration of range of motion: the priority is preventing stiffness, to which calcific tendinitis patients are prone
- Normal use of the arm below shoulder height
Management
- Sling for comfort only; wean as quickly as comfort allows, typically within days
- Unrestricted active use of the arm below shoulder height from day one
- Active elevation above shoulder height as tolerated
- Passive and active-assisted elevation above shoulder height several times daily (using the other arm) to prevent stiffness
- Home exercise program ten repetitions each, three times daily
- Analgesia before exercises; cryotherapy for pain relief as needed
Precautions
- No carrying or lifting beyond approximately two kilograms with the operated arm
- No driving for six weeks (this applies to any shoulder operation)
Criteria to progress
- Wound review satisfactory at the first post-operative appointment
- Out of the sling and using the arm comfortably below shoulder height
Phase II — Regaining your range (weeks 2–8)¶

Kieran Hirpara 4.0
Supported abduction
Cradle the operated forearm with your other arm and lift both out to the side, letting the good arm do most of the work, then lower with control. Progress the range as comfort allows — stretching to firm discomfort is acceptable; forced, severely painful stretching is not.
As guided by your physiotherapist
Kieran Hirpara 4.0
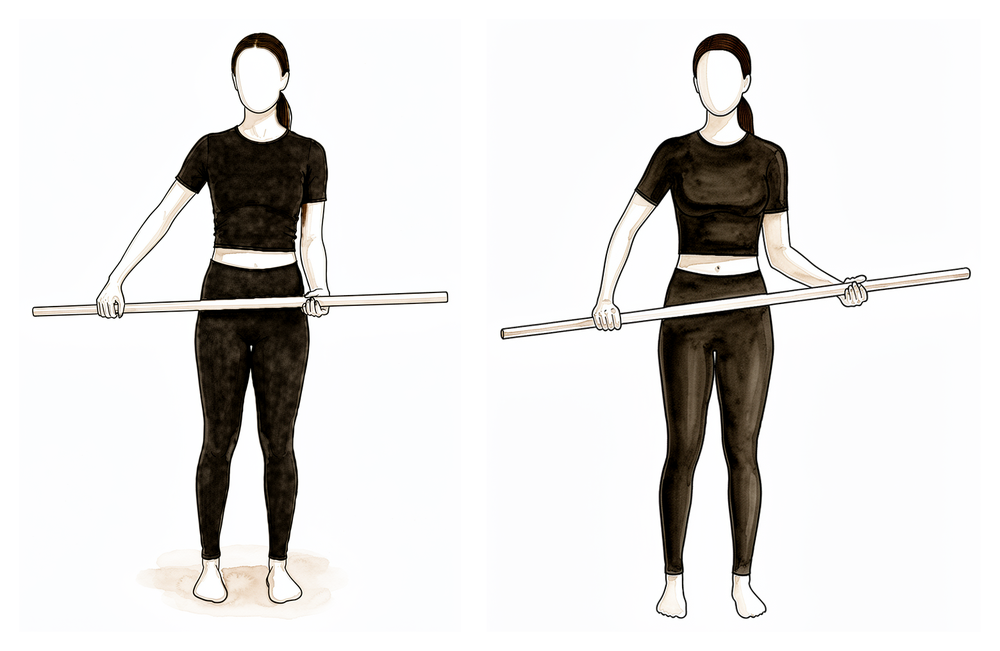
Assisted external rotation with a stick
Lie on your back with the elbow tucked by your side and bent to a right angle. Hold a stick in both hands and use your good arm to turn the operated hand outwards, rotating the shoulder. Restoring this outward rotation is one of the goals of this phase, so keep working it gently a little further each week.
10 times, three times a day
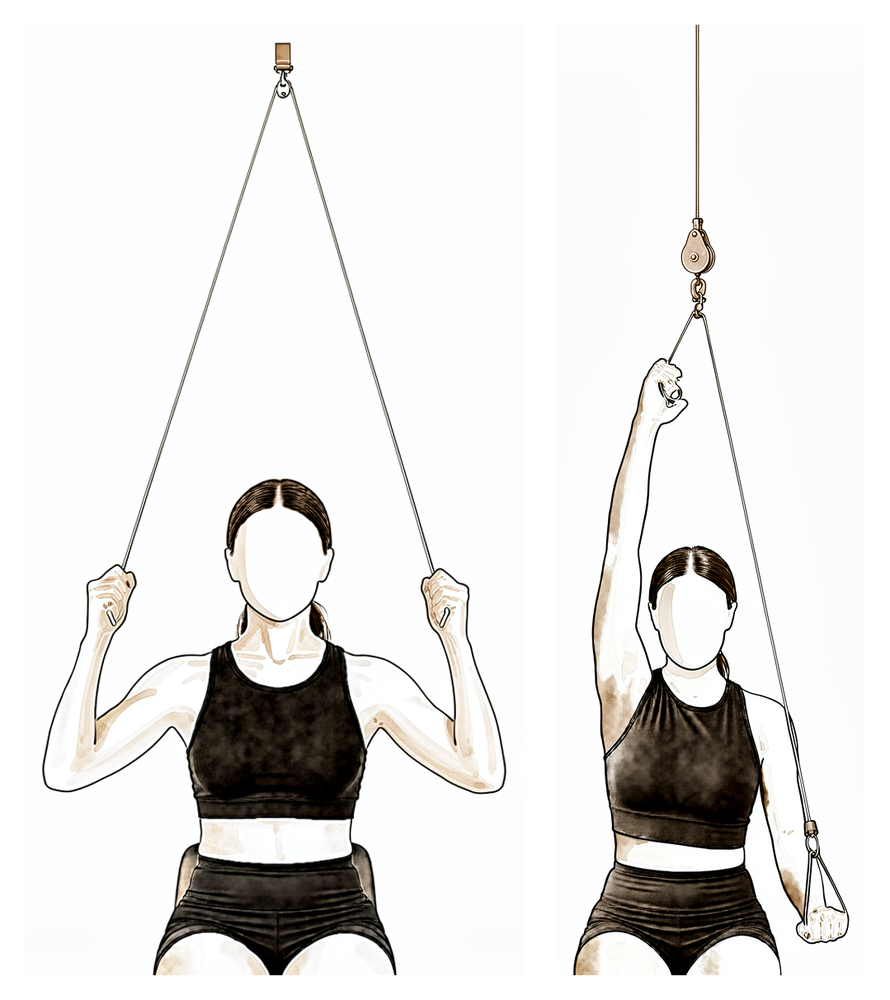
Kieran Hirpara 4.0
Over-door pulley
Sit under an over-door pulley with a handle in each hand. Pull down with your good arm to raise the operated arm overhead as far as it comfortably goes, then lower slowly. Work into a gentle stretch, not sharp pain.
10 times, three to four times a day
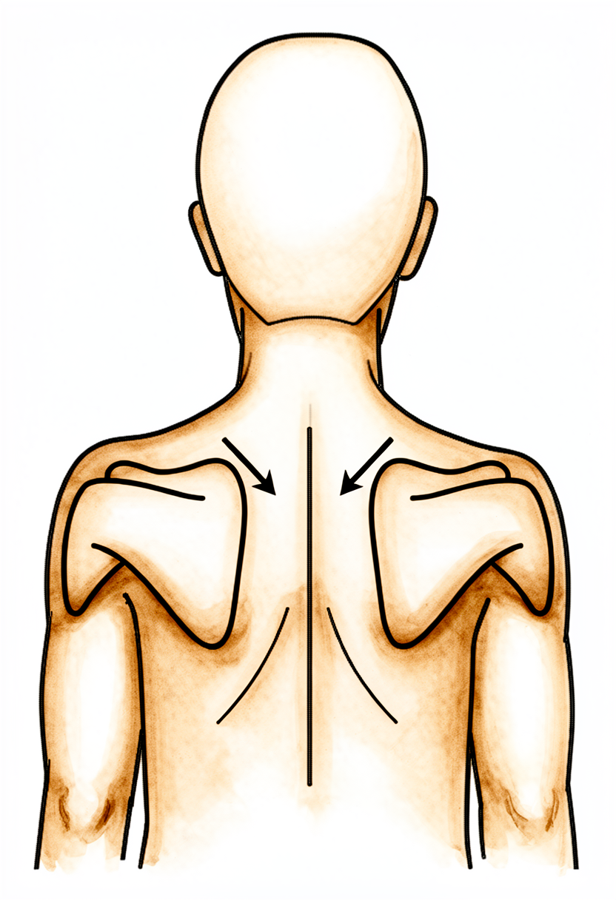
Kieran Hirpara 4.0
Scapular setting
Sitting or standing tall, gently draw your shoulder blades back together and down, away from your ears. Hold for a few seconds, then relax. Continue this alongside your stretches to keep the shoulder blade moving well as your range returns.
As guided by your physiotherapist
You will be reviewed in the rooms at about two to three weeks, where your wound and your passive range of motion are checked. The work of this phase is range: progress your forward elevation stretches and add movements out to the side, with physiotherapy guiding the progression. The typical aims are to lift the arm actively to horizontal by six weeks, with the assisted (passive) range (forward, out to the side and in rotation) back to normal by six weeks. Driving resumes from six weeks, once your surgeon has cleared you and you can perform an emergency stop safely.
For your physiotherapist:
Goals
- Active forward flexion and abduction to horizontal by six weeks
- Passive flexion, abduction and external rotation to normal by six weeks
- Independence with daily activities
Management
- Progress passive and active-assisted forward flexion; introduce and progress abduction
- Progress to active range of motion in all planes as comfort allows
- Continue scapular setting and postural work
- Continue analgesia before sessions, and heat or ice around stretching as preferred
Precautions
- Keep lifting light while range is restored; progression remains symptom-guided
- Stretching to firm discomfort is acceptable; forced, severely painful stretching is not
Criteria to progress
- Passive range of motion at or near normal
- Active elevation to horizontal or better, with pain settling
Phase III — Strengthening and return to full activity (weeks 8–16)¶
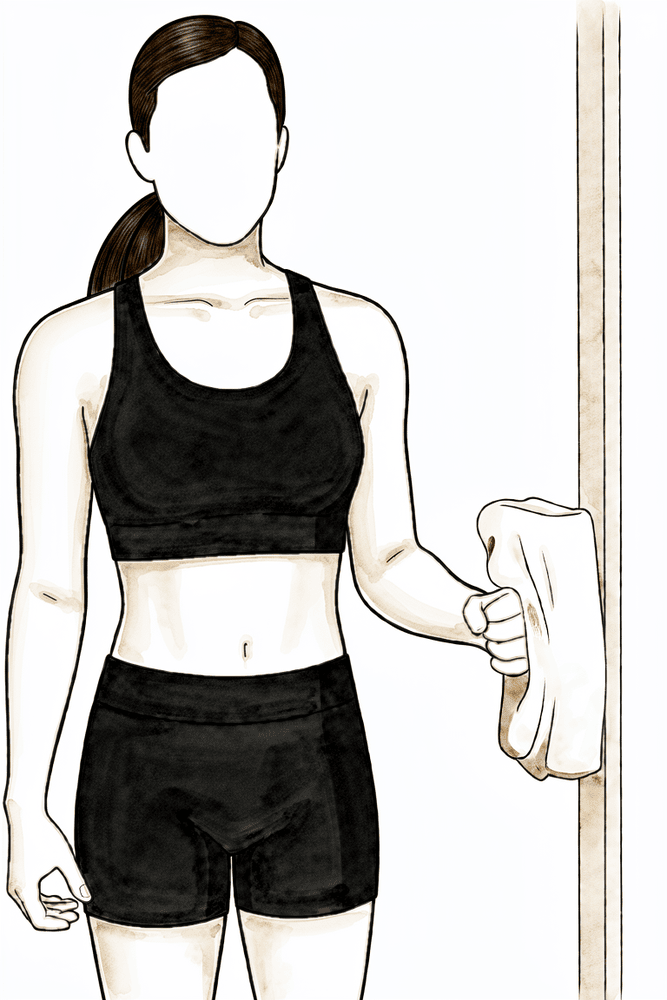
Kieran Hirpara 4.0
Isometric external rotation
Stand with your elbow tucked at your side and bent to a right angle, the back of your hand against a wall or doorframe. Gently press outwards into it without letting the arm move, hold a few seconds, then relax. This builds the rotator cuff with no movement — the starting point for strengthening from about eight weeks.
Hold a few seconds, several times; as guided by your physiotherapist
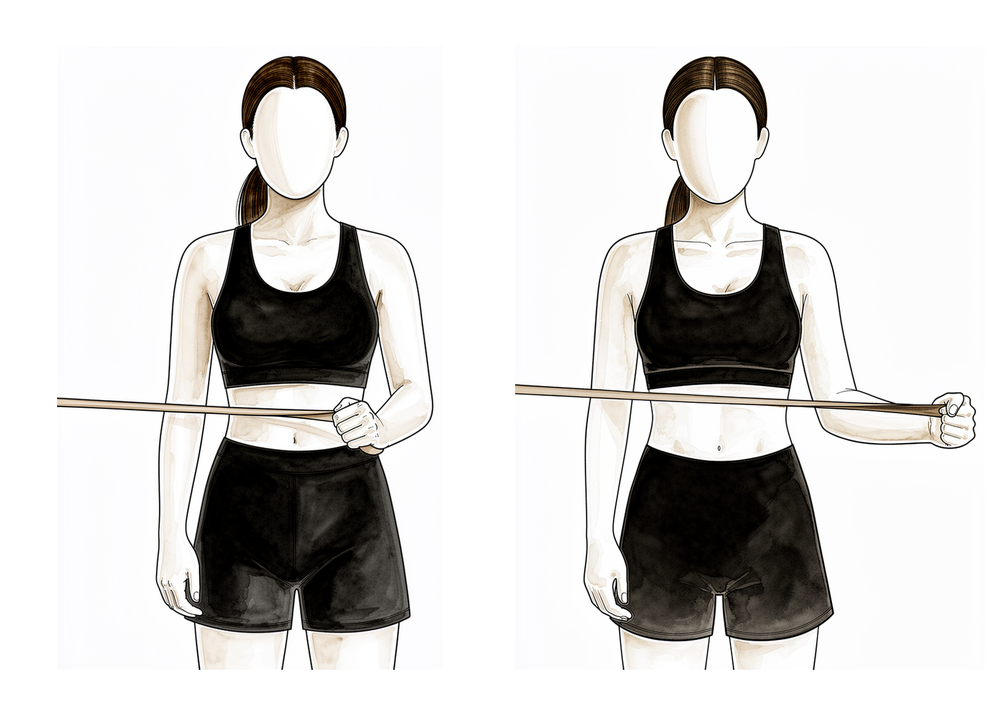
Kieran Hirpara 4.0
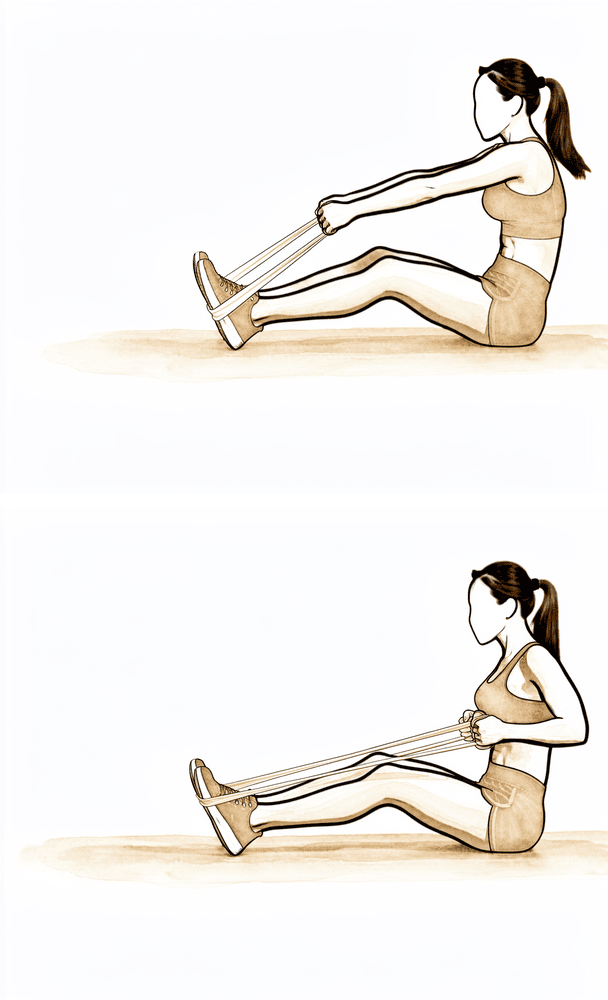
Band external rotation
Stand with your elbow tucked into your side and bent to a right angle, holding an elastic band anchored at waist height. Keeping the elbow at your side, rotate the forearm outwards against the band, then return slowly. Progresses on from the isometric work as your strength builds.
2 to 3 sets of 10 to 15, low resistance
Kieran Hirpara 4.0
Low row
Hold a band anchored in front of you at waist height. Keeping the arm fairly straight, pull it back and down towards your hip, squeezing the shoulder blade down and back, then return slowly. Builds the shoulder-blade muscles that support the cuff.
2 to 3 sets of 10 to 15
Kieran Hirpara 4.0
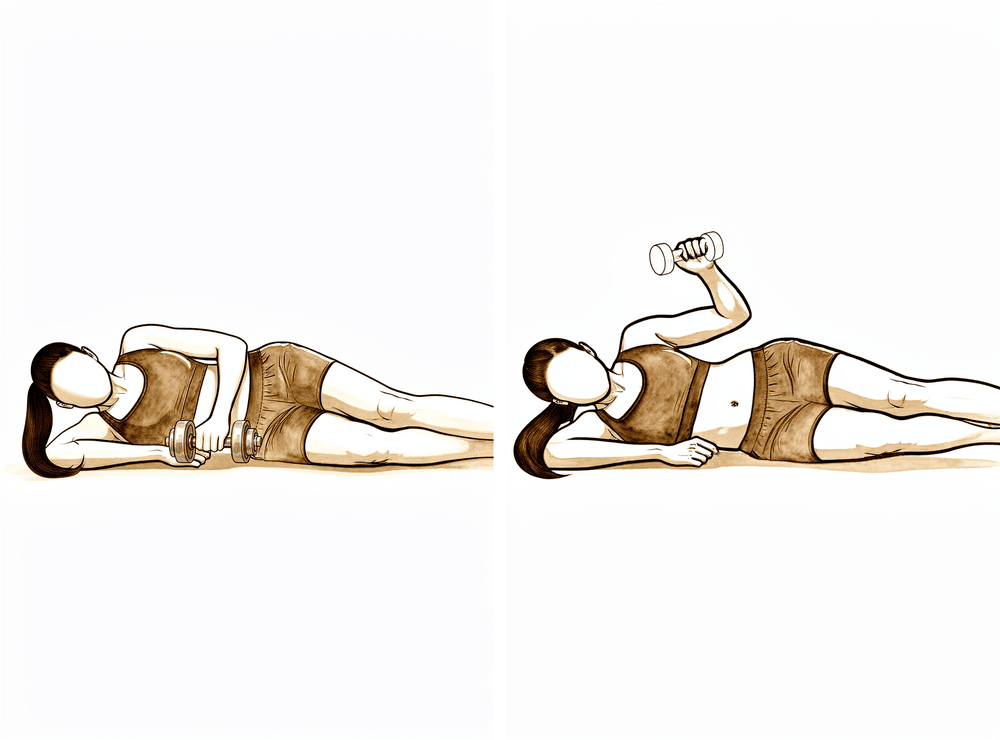
Side-lying external rotation with weight
Lie on your non-operated side with the top elbow bent to a right angle and tucked against your body. Holding a light weight, rotate the forearm up towards the ceiling, then lower slowly. Part of the rotator cuff strengthening from about eight weeks — keep mobility work going alongside it.
Low load, higher repetitions
You will usually be reviewed again at about eight weeks. With your range restored, rehabilitation turns to strengthening the rotator cuff, typically under your physiotherapist's supervision, and to using the arm freely above shoulder height. The aim is full active forward elevation and abduction by about twelve weeks. Recovery from removal of the deposit alone typically takes about three months, after which there are no restrictions; if the rotator cuff needed a repair, recovery is longer (typically around five months) and follows the rotator cuff repair protocol instead. Do not be concerned if some ache persists beyond this point: after this operation it can take up to nine months for the pre-operative symptoms to settle completely, with the trend steadily in the right direction.
For your physiotherapist:
Goals
- Full active forward flexion and abduction by approximately twelve weeks
- Graduated restoration of rotator cuff and scapular strength and endurance
- Return to full, unrestricted activity by approximately three months
Management
- Progressive rotator cuff strengthening from eight weeks: isometrics progressing to elastic-band and light-weight work, low load and higher repetitions
- Progress active use of the arm above shoulder height
- Advance gym-, work- and sport-specific loading as tolerated through weeks twelve to sixteen
Precautions
- Strengthening should not come at the cost of range; continue mobility work throughout
- Build heavy and overhead loading gradually; a flare of pain means easing back a step
Criteria to progress
- Full active range of motion with strength returning and symptoms continuing to settle
- Discharge from routine follow-up when progressing well, typically from around eight to sixteen weeks
After your protocol¶
The phases above are adapted from published patient guidance and rehabilitation protocols for this procedure: The London Shoulder Partnership's calcific deposit excision rehabilitation protocol, patient guidance from ShoulderDoc (UK) on surgery for calcific tendinitis, and Dr Kevin Ko's patient guide to arthroscopic excision. The week ranges are typical rather than fixed, and your ongoing rehabilitation is guided individually by your physiotherapist, working with the practice, based on how your shoulder recovers. This page works alongside the practice's general recovery advice: see managing post-operative pain and wound care. For the condition itself and how these treatments work, see calcific tendinitis. The evidence behind this protocol (natural history, barbotage, and the surgical-excision literature) is summarised in the evidence section, available as a PDF from the top of this page.
Evidence & references
Calcific Tendinitis of the Rotator Cuff — Staged Management & Post-operative Rehabilitation (Arthroscopic Excision)¶
Topic scope: (A) the natural history and stepped non-operative management of rotator-cuff calcific tendinitis (rest/analgesia → barbotage ± subacromial steroid → ESWT), and (B) post-operative rehabilitation after arthroscopic excision of the calcific deposit (± subacromial decompression; the cuff-repair pathway defers to the rotator-cuff-repair protocol).
Defining principle of the surgical rehab here: arthroscopic excision removes the source of pain and does not, by itself, create a construct that needs months of protection — provided the rotator cuff is left intact. So (like a debridement/decompression, and unlike a cuff repair) the rehab is an early-movement pathway: short sling for comfort only, unrestricted use below shoulder height from day one, assisted elevation to prevent stiffness, strengthening from ~8 weeks. The single branch point is whether removing the deposit left a tendon defect that needed repair — if so, the recovery converts to the slower, protected rotator-cuff-repair pathway.
A. NATURAL HISTORY & NON-OPERATIVE MANAGEMENT¶
Natural history (self-limiting in most)¶
Rotator-cuff calcific tendinitis is self-limiting in the majority: after a variable quiescent period the deposit enters a resorptive phase (peripheral vascularisation + phagocytosis), and spontaneous resorption occurs in roughly two-thirds of cases within 1–2 years [Uhthoff & Loehr; Chianca 2018 review]. This underpins a non-operative-first approach and explains why post-operative residual calcium that "dissolves spontaneously" does not harm the outcome.
Stepped non-operative interventions¶
- Analgesia / activity modification / physiotherapy — first line; many settle as the deposit resorbs. Consensus.
- Ultrasound-guided barbotage (needling + lavage), usually + subacromial corticosteroid — the best-supported interventional option. A systematic review of 908 patients and subsequent meta-analyses favour barbotage for medium-term pain/function; barbotage + subacromial steroid improves Constant–Murley score and reduces deposit size vs steroid alone. Notably, clinical improvement is NOT dependent on how much calcium is aspirated — perforating the deposit to trigger resorption is the active mechanism. Moderate–strong (SR/RCT).
- Extracorporeal shock-wave therapy (ESWT) — reduces deposit size and pain; broadly comparable to barbotage in several comparisons. Moderate (RCT).
B. POST-OPERATIVE REHABILITATION (arthroscopic excision ± subacromial decompression)¶
Surgery is reserved for deposits recalcitrant to adequate non-operative care. The operation locates and removes the deposit from within the cuff tendon, often with a subacromial decompression for room. Key surgical-outcome facts that shape the rehab:
- Preserving cuff integrity while removing as much deposit as possible gives good-to-excellent results in ~90% and avoids iatrogenic tendon defects [arthroscopic excision series].
- Complete vs near-complete removal gives equivalent outcomes — residual calcium resorbs spontaneously afterwards; the surgeon need not chase every fleck at the cost of the tendon.
- Arthroscopic decompression WITHOUT cuff repair is a validated strategy with good outcomes where the residual defect is not repaired [Bone & Joint 2023].
- Symptom settling is gradual — significant pain relief and ROM gains are the norm, but the pre-operative symptoms can take up to ~9 months to fade fully; recovery to unrestricted activity after excision alone is ~3 months.
Phased post-op timeline (no cuff repair)¶
| Phase | Window | Sling | ROM / use | Strengthening | Notes |
|---|---|---|---|---|---|
| I — Early movement | Week 0–2 | Comfort only, days (rarely > 2 wk), off ASAP | Unrestricted use below shoulder height from day 1; assisted elevation above shoulder height several × daily to prevent stiffness | — | Settle post-op flare; calcific patients are stiffness-prone → motion is the priority. ≤ ~2 kg, no driving while in sling |
| II — Regaining range | Week 2–8 | Off | Progress active elevation; restore full passive + active ROM | Begin gentle as pain allows | Most regain comfortable range through this window |
| III — Strengthening / return | Week 8–16 | Off | Full active elevation goal by ~12 wk | Cuff + scapular strengthening from ~8 wk, isometric → band/light weight; advance work/sport loading wk 12–16 | Full unrestricted activity ~3 months; discharge ~8–16 wk |
Branch point — if a rotator cuff repair was required: recovery converts to the protected rotator-cuff-repair pathway (sling ~6 wk, ROM restrictions, strengthening deferred), typically ~5 months total. The surgeon confirms post-operatively which pathway applies.
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Surgery is a last resort — given high spontaneous-resorption rates and effective barbotage/ESWT, excision is reserved for genuinely recalcitrant cases. Strong rationale.
- How much to remove / whether to repair the defect. Equivalent outcomes for complete vs partial removal, and viable decompression-without-repair, mean the surgeon balances deposit clearance against tendon integrity intra-operatively — which in turn decides the rehab pathway. Moderate.
- The post-op rehab protocol itself is consensus/expert, drawn from surgeon patient-guidance protocols rather than a rehab RCT — phase timings are typical, not trial-derived.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- MODERATE–STRONG (SR / RCT): barbotage ± steroid for non-operative calcific tendinitis (908-patient SR; barbotage + steroid > steroid alone); ESWT efficacy.
- MODERATE (cohorts): arthroscopic excision outcomes (~90% good-excellent; equivalence of complete vs partial removal; decompression without repair, Bone & Joint 2023); spontaneous resorption ~2/3 within 1–2 years.
- WEAK / CONSENSUS: the post-operative rehabilitation protocol (surgeon patient-guidance documents; no defining rehab RCT).
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles) — adjacent rotator-cuff evidence¶
- Predictors of failure of non-operative treatment of chronic symptomatic rotator-cuff disease (2013 Neer Award). J Shoulder Elbow Surg. 2016. DOI: 10.1016/j.jse.2016.04.030
- Arthroscopic rotator cuff repair: scientific rationale, surgical technique, early clinical results. J Shoulder Elbow Surg. 2010. DOI: 10.1016/j.jse.2009.12.012
- Early versus delayed rehabilitation after arthroscopic rotator cuff repair. Knee Surg Sports Traumatol Arthrosc. 2024. DOI: 10.1002/ksa.12129
- Speed of recovery after arthroscopic rotator cuff repair. J Shoulder Elbow Surg. 2017. DOI: 10.1016/j.jse.2016.11.002
- (The corpus is thin on calcific-tendinitis-specific rehab; the evidence base below is the calcific literature + published surgeon protocols.)
Calcific tendinitis literature (URLs)¶
- Ultrasound-guided barbotage for calcific tendonitis of the shoulder: a systematic review including 908 patients (DARE). https://www.ncbi.nlm.nih.gov/books/NBK241935/
- Determining the efficacy of barbotage for pain relief in calcific tendinitis. JSES Int / ScienceDirect. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC11401591/
- Needling and lavage in rotator-cuff calcific tendinitis: ultrasound-guided technique. PMC. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10805427/
- Calcific tendinitis of the rotator cuff: a review (natural history, phases, resorption). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC3749672/
- Recovery pattern after arthroscopic treatment for calcific tendinitis of the shoulder. Orthop Traumatol Surg Res. 2020. https://www.sciencedirect.com/science/article/pii/S1877056820301043
- Arthroscopic decompression of calcific tendinitis without cuff repair. Bone Joint J. 2023. https://boneandjoint.org.uk/Article/10.1302/0301-620X.105B6.BJJ-2022-1137.R1
- Arthroscopic treatment of calcific tendonitis (preserve cuff, ~90% good-excellent; residuals resorb). PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4044535/
Published rehab protocols (patient-guidance — basis for the phase structure)¶
- The London Shoulder Partnership — Calcific Deposit Excision Rehabilitation. http://thelondonshoulderpartnership.co.uk/shoulder/shoulder-rehabilitation/calcific-deposit-excision-rehabilitation/
- Ko K. Arthroscopic Excision of Calcific Tendonitis — What Can I Expect? (OPA Orthopedics). https://www.kevinkomd.com/pdf/calcific-tendonitis.pdf
- Funk L. Surgery for Calcific Tendinitis. ShoulderDoc. https://shoulderdoc.co.uk/pages/surgery-for-calcific-tendinitis