What you're feeling¶
You may notice pain in the back of your shoulder or deep in the shoulder blade area. This pain often feels like a dull ache that can become sharp with movement. In many cases, you might also feel sudden weakness when trying to lift your arm or rotate it. These two symptoms—pain and weakness—are the most common ways this condition shows up, especially if you are active.
The pain often flares up after you have been using your arm for a while. You might feel it more strongly at night, which can make it hard to sleep. Sleeping on the affected side is usually uncomfortable or painful. You may also notice stiffness when you first wake up in the morning. The discomfort tends to worsen with activities that require your arm to be raised or moved across your body.
Daily tasks can become difficult because of this pain and weakness. You might struggle to reach behind your back to fasten a bra or tuck in a shirt. Reaching for items on a high shelf can feel unstable or painful. Even simple movements, like putting on a coat or washing your hair, may require extra effort or cause a spike in pain. If you try to push through the discomfort, the pain often lingers longer into the evening.
In some cases, you might not feel significant pain at all. Instead, the main issue is a loss of strength. You might find that your arm feels heavy or that you cannot lift it as high as you used to. This weakness can happen even if the tendons in your shoulder are still intact. The nerve signals that tell your muscles to work are being interrupted, leading to this specific type of fatigue and power loss.
If you experience these symptoms, your surgeon will look for signs of nerve irritation. They may check for tenderness at specific points on your shoulder blade or test your muscle strength. Understanding whether your primary issue is pain or weakness helps guide the next steps in your care.
What's actually happening¶
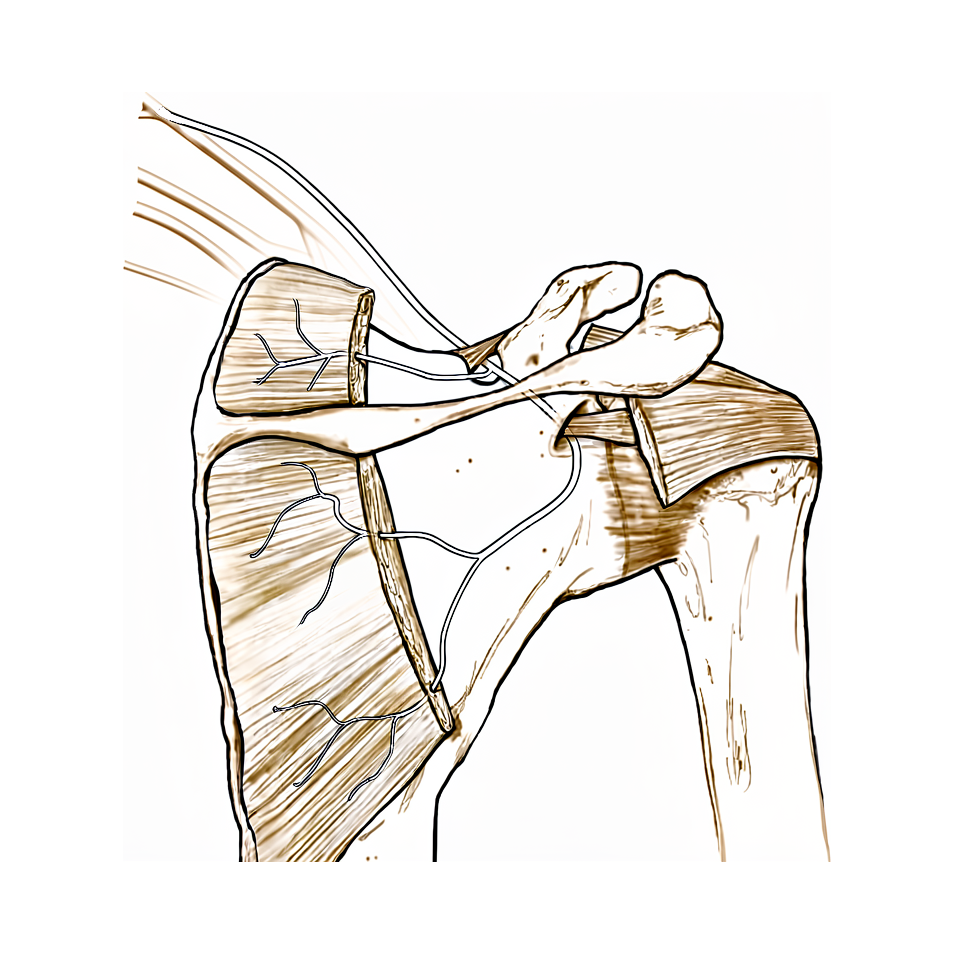
Your suprascapular nerve is a cable that sends signals from your neck to your shoulder muscles. It passes through two narrow tunnels in your shoulder blade. These tunnels are formed by bones and tough bands of tissue called ligaments. Sometimes, these tunnels are naturally narrow. Other times, extra tissue or bone changes can squeeze the nerve. This pressure stops the nerve from working properly.
When the nerve is compressed, it cannot tell your shoulder muscles to move or feel pain correctly. You might notice weakness in your arm or a deep ache in your shoulder. In some cases, the muscle itself changes. It may lose its healthy tissue and become replaced by fat. This happens even if the tendons that attach to your bone are still intact. The nerve injury weakens the structure that holds your rotator cuff in place.
There are several reasons this squeezing happens. A large collection of blood (hematoma) or a benign fatty growth (lipoma) can press on the nerve. In some people, the shape of their shoulder blade makes the nerve more likely to get trapped. This can also occur after shoulder surgery. For example, if a screw used to secure a joint replacement is placed too high, it can hit the nerve. Even before surgery, an existing nerve injury does not always cause new problems during a joint replacement.
We often see this condition in active people who report either pain or weakness as their main complaint. If there is no clear object pressing on the nerve, we usually start with non-surgical care. This includes rest, anti-inflammatory medicines, and physical therapy. If the nerve is clearly trapped by a physical barrier, or if your symptoms get worse, we may recommend a procedure to free the nerve. This involves cutting the tight band of tissue to give the nerve more space.
What we can do about it¶
At Mater Private Hospital Rockhampton, Dr Kieran Hirpara approaches suprascapular neuropathy by matching treatment to the cause of your nerve compression. We start with the least invasive options and move to surgery only if needed. Your journey begins with a clear diagnosis based on your history, examination, and imaging. This helps us avoid missed issues and unnecessary repeat procedures.
For most cases without a clear structural block, we begin with non-operative care. You will likely try activity modification to avoid movements that irritate the nerve. Physical therapy is a core part of this phase. It aims to strengthen the muscles around your shoulder and improve movement patterns. We typically give this approach time to work before considering other steps. If a cyst or fluid collection is pressing on the nerve, we may monitor it closely. In some cases, these cysts resolve on their own, allowing your nerve function to return without surgery.
If pain persists, we discuss medical management to help you stay active. This often includes nonsteroidal anti-inflammatory drugs to reduce swelling and pain around the nerve. We may also consider injections. Cortisone injections can calm inflammation and provide temporary relief. Hyaluronic acid or platelet-rich plasma (PRP) injections are other options we may discuss to support joint health. These treatments aim to manage symptoms while your body heals or while you continue with physiotherapy. The effect of these injections varies, but they can provide a window of comfort to engage in rehabilitation.
Surgery is considered when conservative care does not provide enough improvement, or if you have progressive weakness or severe pain. We also recommend surgery sooner for structural problems, such as a specific ligament compressing the nerve, where waiting may not help. Arthroscopic release is a common surgical option. This minimally invasive procedure involves making small incisions to relieve pressure on the suprascapular nerve. We may release the transverse scapular ligament or the spinoglenoid ligament, depending on where the compression is located. This decompression aims to restore normal shoulder function and relieve pain. For athletes, this approach often allows a return to sport. If you also have a rotator cuff tear, we discuss whether nerve release adds benefit to the repair. In many cases, repairing the cuff alone is sufficient, and adding nerve release does not significantly change the outcome. We make this decision together, based on your specific anatomy and goals.
What to expect¶
Your outlook depends on whether a clear cause for the nerve pressure can be found. If you have a well-defined lesion pressing on the suprascapular nerve, your surgeon will likely recommend surgery. This procedure, called decompression, frees the nerve from tight bands or ligaments. In cases without major shoulder joint damage, this approach leads to good functional outcomes with significant improvements from before to after surgery. You can expect relief of pain and a return of normal shoulder function. Full recovery of shoulder function is possible, even in complex cases like those caused by bleeding into the shoulder blade area.
If no clear mechanical compression is found, your surgeon will typically advise non-operative treatment first. This initial path involves physical therapy, anti-inflammatory medications, and changing your daily activities to reduce strain. This conservative approach is the standard starting point for isolated nerve issues.
You should know that the relationship between nerve issues and rotator cuff tears is complex. Sometimes, nerve injury can lead to fatty infiltration and muscle wasting in the shoulder muscles, even if the tendons themselves are intact. This pattern differs from the damage seen in chronic tendon tears alone. If you have a large or massive rotator cuff tear, adding nerve decompression to the repair does not necessarily produce better outcomes than repairing the cuff alone. Your surgeon will weigh these factors carefully to avoid unnecessary procedures.
Recovery is a gradual process. While specific timelines vary, significant improvements are noted as you progress through your treatment plan. In young, active patients, the main complaints are usually pain or weakness. Addressing these effectively often restores your ability to use your shoulder normally. However, if the condition is left untreated or if the underlying cause is not properly identified, symptoms may persist or lead to further muscle changes. A thorough evaluation helps ensure that all issues in your shoulder are treated at the same time, reducing the need for future operations.
When to see someone¶
See your GP if you have shoulder pain or weakness that does not improve with rest. Suprascapular neuropathy often causes distinct pain or weakness in young, active people. Ask for a specialist review if symptoms interfere with sleep or work. Sudden worsening, locking, or a feeling of instability also warrant prompt attention. While the link to rotator cuff issues is unclear, nerve entrapment at the shoulder notch can cause muscle wasting. Initial treatment is usually non-surgical, involving physical therapy and anti-inflammatory drugs. However, if there is clear nerve compression or progressive weakness, surgery may be needed. A thorough check helps avoid missed problems and the need for further operations.