Patients › Rehabilitation
Distal Biceps Tendon Repair
A protected early-motion recovery plan after surgical repair of a ruptured distal biceps tendon, allowing comfortable movement from day one while guarding the repair from resisted lifting until strength is rebuilt in stages.
This protocol guides your recovery after surgical repair of a ruptured distal biceps tendon with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your physiotherapist or hand therapist. Bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
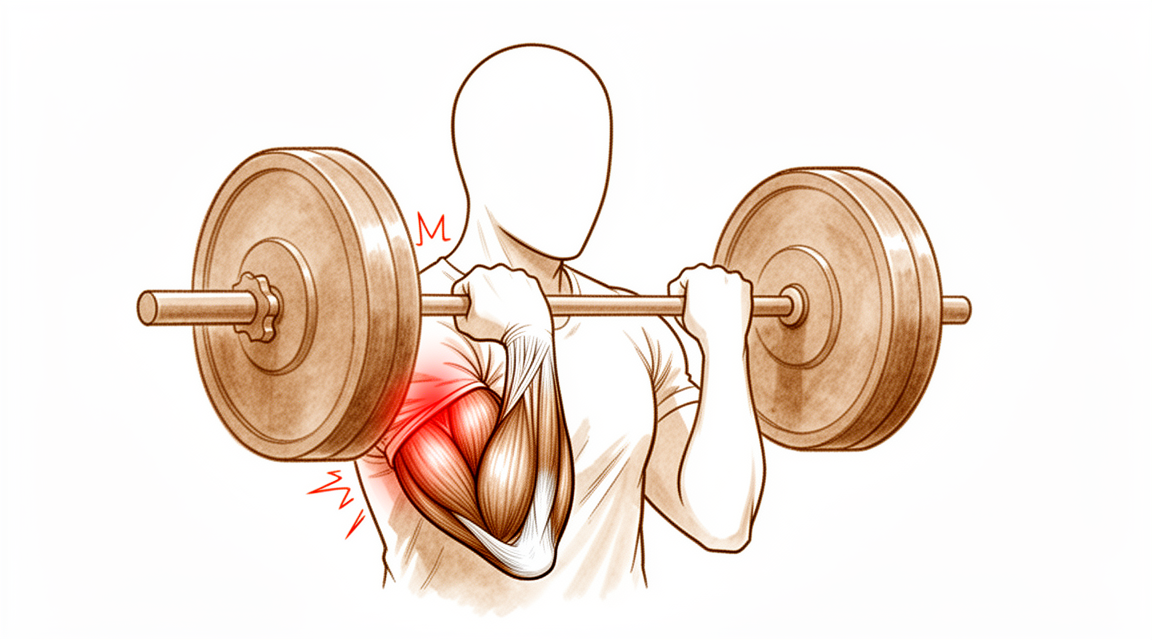
The distal biceps tendon is the cord that anchors your biceps muscle to the radius bone just below the front of the elbow. When it ruptures it is reattached to its bony footprint on the radius. Dr Hirpara repairs it using a cortical button, a small, strong fixation that holds the tendon firmly against the bone while it heals back on.
Because this is a strong repair, the recovery is built around comfortable early movement rather than rigid immobilisation. You will wear a simple sling for about 6 weeks (not a hinged elbow brace) and you are encouraged to move the elbow through its full comfortable range from day one, including straightening it out. Early movement keeps the elbow from going stiff, which is one of the main problems after this operation.
The strength of the repair is deliberately spent on allowing this early movement. It is not a licence to lift early. The tendon still has to knit biologically back onto the bone, and that healing is what protects you from re-rupture. For that reason, loading the arm (lifting, gripping hard and resisted strengthening) is held back until about 4 months, then introduced lightly and built up gradually. The sling is mainly for comfort and as a reminder not to use the arm heavily; it comes off for your exercises and for washing.
For wound, swelling and scar management, see the practice's wound care guidance.
Precautions and limitations¶
Do
- Move your elbow, forearm, wrist and hand through their full comfortable range from day one: bending, straightening and rotating the forearm.
- Take the sling off for your exercises and for hygiene; wear it for comfort and protection the rest of the time for about 6 weeks.
- Use the arm for very light everyday tasks (eating, light self-care) within comfort.
Do not
- Do not lift, carry, grip hard or do any resisted strengthening with the operated arm until you are cleared at about 4 months. This is the single most important precaution.
- Do not force a sudden, sharp straightening of the elbow against a load, and avoid forced or jerky movements.
- Do not stretch your shoulder back into hyperextension early, as this pulls on the healing wound at the front of the elbow.
Your exercises¶

Kieran Hirpara 4.0
Elbow bend and straighten (to comfort)
With your palm facing up, gently bend your elbow up towards your shoulder as far as is comfortable, then slowly straighten it back down as far as is comfortable. There is no limit on how far you move — let comfort be your guide and move smoothly. Keep your upper arm resting at your side.
10 times, 3–4 times a day
Kieran Hirpara 4.0
Assisted elbow bend
Let the operated arm relax completely, then use your other hand to gently bend the elbow up towards your shoulder. You are not pulling with the operated arm — the other hand does the work. This keeps the elbow supple in the early weeks.
10 times, 3–4 times a day
Kieran Hirpara 4.0
Elbow straightening (to comfort)
Slowly straighten your elbow down to a comfortable position and then bend it back up. Full straightening is allowed as comfort permits — there is no need to block or hold back the straightening direction. Move gently and avoid any sudden or forced movements.
10 times, 3–4 times a day
Kieran Hirpara 4.0
Forearm rotation (palm up / palm down)
Tuck your elbow into your side and bend it to about a right angle. Gently turn your palm up towards the ceiling, hold for a moment, then turn it down towards the floor. Keep the elbow tucked in so the movement comes from the forearm, not the shoulder.
10 times each direction, 3–4 times a day

Kieran Hirpara 4.0
Hand, wrist and grip movement
Keep your hand and fingers moving from the start. Open your hand wide, then make a gentle fist and release. Move your wrist up and down too. This keeps the hand supple and prevents stiffness and swelling while the elbow heals.
10–15 times, several times a day
Kieran Hirpara 4.0
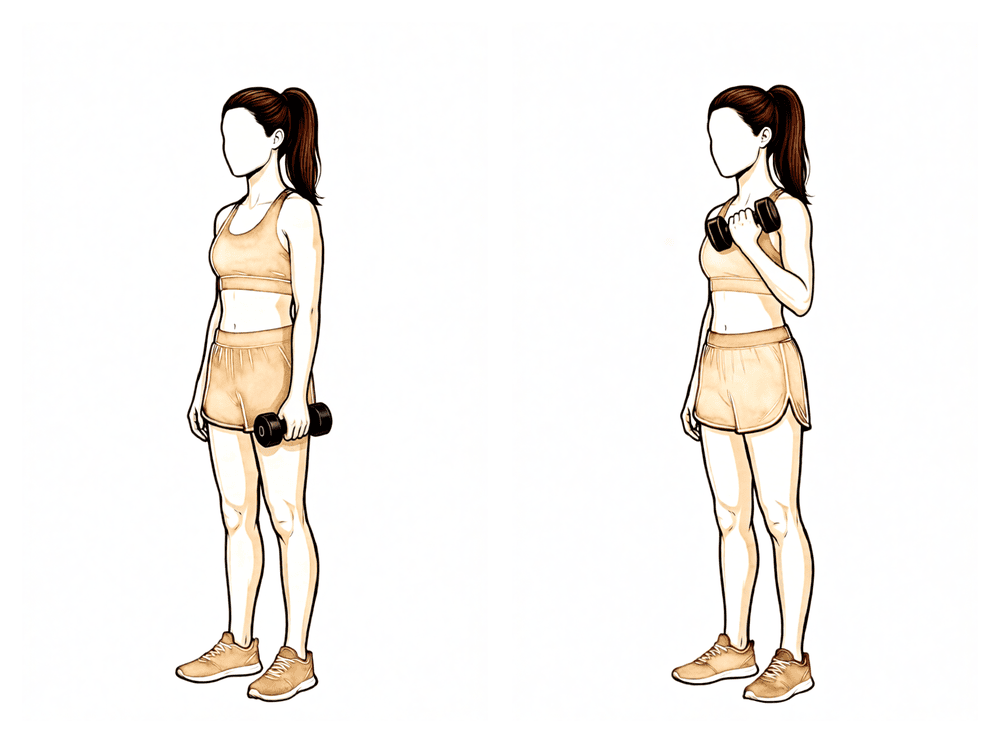
Resisted biceps curl (from about 4 months)
Begin ONLY once Dr Hirpara or your therapist has cleared you to start loading (from about 4 months). With your palm facing up, hold a light weight and slowly curl it up towards your shoulder, then lower under control. Start very light and add resistance gradually over the following weeks.
10–15 times, building up gradually once cleared
Kieran Hirpara 4.0
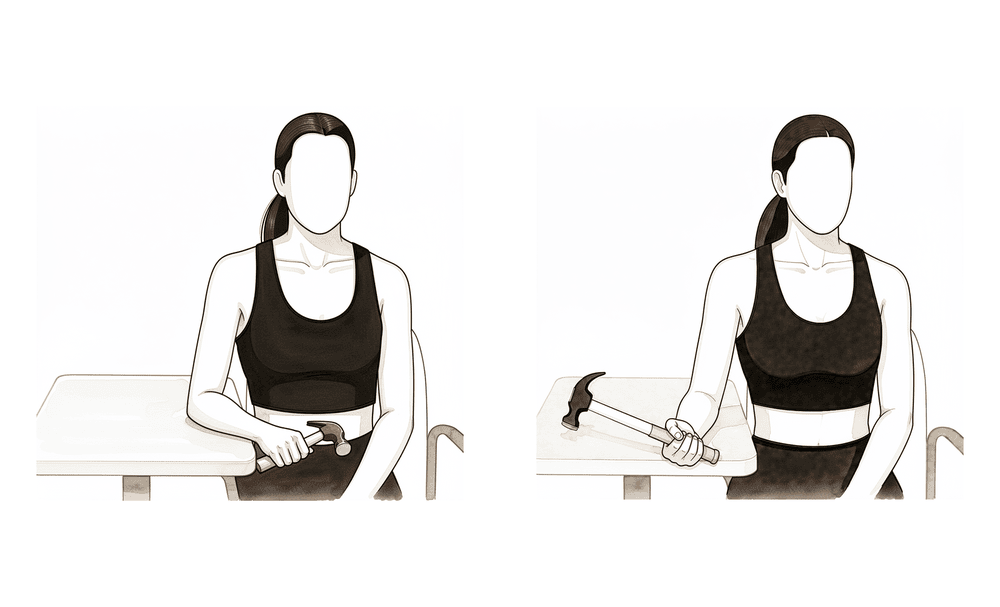
Resisted forearm rotation (from about 4 months)
Begin ONLY once you have been cleared to start loading (from about 4 months). With your elbow tucked in, turn your palm up against the light resistance of a band or a light weight held at one end, then return under control. This rebuilds the twisting (supination) strength the biceps provides. Start light and progress gradually.
10–15 times, building up gradually once cleared
These are the exercises from your handout for keeping your elbow, forearm and hand moving in the early weeks. Take the sling off to do them. Move only as far as is comfortable, and start them as guided by Dr Hirpara and your therapist. The two strengthening exercises are introduced later: only once you have been cleared to begin loading at around 4 months.
Your clinical protocol¶
The rest of this page is the clinical protocol for rehabilitation after a cortical-button distal biceps tendon repair. This section is to be provided to your physiotherapist or hand therapist, and each phase below opens with a plain-English explanation of what is happening.
The guiding principle is early comfortable motion with delayed loading: the cortical-button construct is strong enough to permit unrestricted movement from day one, so there is no hinged brace and no extension block. The construct's strength is used to prevent stiffness, not to justify early loading; resisted strengthening and lifting are deliberately deferred to protect tendon-to-bone healing and minimise re-rupture.
Phase I — Protected comfort motion (Week 0 → 6)¶
A simple sling is worn for comfort and as a reminder against heavy use; it is removed for exercises and hygiene. The aim is to maintain comfortable, near-full range of motion while protecting the repair from any load.
For your physiotherapist:
- Immobilisation: Simple sling for 6 weeks, off for exercises and hygiene. No hinged brace; no extension block.
- Range of motion: All motion as comfort allows from day 1: active and passive elbow flexion, extension and forearm rotation. No arc restriction and no extension block.
- Goals: Maintain comfortable full range of motion; protect the repair from load; keep the hand, wrist and shoulder mobile.
- Exercises: Active elbow flexion/extension to comfort; assisted (passive) elbow flexion; forearm pronation/supination active range with the elbow tucked at the side; hand, wrist and grip movement; scapular and shoulder range of motion. No resisted biceps or supination loading.
- Precautions: No lifting, gripping or resisted strengthening; avoid sudden forced eccentric extension against load; avoid shoulder hyperextension.
- Criteria to progress: Wound healed, comfortable near-full range of motion, out of the sling at 6 weeks.
Phase II — Full motion, unloaded (Week 6 → ~4 months)¶
The sling is discontinued. The arm is used freely for light everyday tasks, but without resisted loading or lifting: the tendon is still maturing onto bone, and this is the window where caution against load matters most even though motion is safe.
For your physiotherapist:
- Goals: Full symmetric pain-free range of motion; normal light functional use of the hand and arm.
- Range of motion / use: Full motion as comfort allows; everyday light use without resisted loading or lifting.
- Exercises: Continue range-of-motion work; hand, wrist and grip; scapular and shoulder conditioning. No resisted biceps or supination loading yet.
- Criteria to progress: Full painless range of motion; wound and repair settled → begin graded loading at about 4 months.
Phase III — Strengthening and graded loading (~4 → 6 months)¶
Loading begins. Light resisted strengthening for elbow flexion and forearm supination is introduced and progressed gradually towards functional, then job- or sport-specific demands.
For your physiotherapist:
- Goals: Rebuild flexion and supination strength; return to work and sport.
- Exercises: Start light resisted strengthening and lifting at about 4 months; progress gradually (isotonic curls and resisted supination → functional patterns → job- and sport-specific loading).
- Criteria to progress: Pain-free resisted flexion and supination; strength approaching the other side.
Getting back to work and activity¶
In the first 6 weeks, expect to use the arm only for light, comfortable everyday tasks with the sling on for protection. Light desk-based or one-handed duties are often possible early; heavier or two-handed manual work waits until loading has begun and built up.
The key milestones are:
- No lifting and no resisted loading in the early months: this is deliberate, to let the tendon heal onto the bone.
- Light lifting and strengthening from about 4 months, started gently and progressed week by week.
- Return to non-contact sport from about 4 months; unrestricted (contact) sport at about 6 months, once the criteria are met: full painless range of motion, strength at least 90–100% of the other side, and tolerance of the specific demands of your job or sport.
You must not drive while you are wearing the sling. Driving resumes once you are out of the sling and can comfortably and safely control the vehicle, as confirmed at your review. Always follow Dr Hirpara's specific advice, as timings can vary with the demands of your work and sport.
After your protocol¶
This protocol works alongside the practice's general recovery advice; see managing post-operative pain and wound care. The phased plan above is consistent with published evidence on rehabilitation after distal biceps tendon repair, and your ongoing recovery is guided individually by your physiotherapist or hand therapist according to how your elbow progresses.
Evidence & references
Distal Biceps Tendon Repair — Post-operative Rehabilitation (Evidence)¶
Topic scope: Post-operative rehabilitation after surgical repair of a ruptured distal biceps tendon reattached to the radial tuberosity with cortical-button fixation. The protocol here reflects Dr Hirpara's practice — a sling-only, early-comfort-motion approach with deliberately delayed loading — set against the published spectrum of distal-biceps rehabilitation protocols.
Defining principle: Cortical-button fixation is the strongest available construct, and biomechanical and clinical evidence show it tolerates immediate motion safely. Dr Hirpara's stance is to spend that strength on early movement, not early loading: a simple sling for 6 weeks (no hinged brace, no extension block) with all motion to comfort from day 1 including extension, but with resisted strengthening and lifting held back until ~4 months to protect tendon-to-bone healing and minimise re-rupture, and unrestricted activity / return to sport at ~6 months on criterion-based clearance. This sits at the protective end of loading while matching the most current thinking on early motion for stiffness prevention.
Where this protocol sits in the evidence¶
Published distal-biceps protocols span a wide range, from rigid hinged-brace extension-block schemes to immediate unrestricted motion. Dr Hirpara's plan diverges from the "traditional" template in two deliberate ways:
- Immobilisation: A simple sling for comfort, not a hinged ROM brace, and no extension block. Motion is unrestricted to comfort from day 1. The mainstream BWH/MGB protocols instead use a posterior splint at 90° for 5–7 days, then a hinged brace with a 45°→30° extension block opened ~10°/week to full extension by ~6 weeks (or ~3 weeks in the accelerated variant). Dr Hirpara's approach is at the early-motion end and is justified by the strength of the cortical-button construct.
- Loading: Resisted strengthening and lifting are deferred to ~4 months. This is more conservative than the published loading timelines (accelerated resisted work at week 6; standard/MGB at weeks 8–10–12; light weights weeks 12–14). Crucially, this conservatism is a choice made despite having the construct that would permit earlier loading.
The endpoint — unrestricted activity / return to sport at ~6 months, criterion-based — is the single most commonly cited endpoint across protocols and matches the mainstream consensus.
Key evidence and controversies¶
-
Early/immediate motion is safe with modern fixation. (Moderate) Biomechanical work supports immediate motion: Bisson et al (AJSM 2007) found aggressive rehabilitation safe after the modified 2-incision approach, and Rose et al (KSSTA 2010) showed single-incision EndoButton/FiberWire repairs survive 2,000 immediate-motion cycles. Several series report no increased re-rupture with immediate post-operative motion. This underpins the sling-only, motion-to-comfort approach.
-
Cortical-button strength enables early motion. (Moderate) Cortical-button (± interference screw) fixation has the highest load-to-failure of the available constructs (Olsen JSES 2014; Spang JSES 2006; Lang OTSR 2018 — comparable functional outcomes across constructs but higher load-to-failure for cortical button). Spencer/Edwin (HAND 2008) argued EndoButton fixation strength may allow earlier ROM. This fixation strength is the explicit rationale for permitting immediate movement.
-
Mobilisation timing may not change outcome. (Moderate) A retrospective comparison found no clinically significant difference in failure, complications, ROM or patient-reported outcomes for early versus delayed mobilisation after primary distal biceps repair. This undercuts the urgency of accelerating loading and supports a measured progression.
-
Conservative rehab may lower re-rupture. (Consensus / survey) Rosenthal/Ting/Sher (JSES 2023), a survey of fellowship-trained elbow surgeons, suggests more conservative post-operative rehab may be associated with lower re-rupture risk — a direct counterweight to the accelerated-loading trend and the rationale for deferring loading to ~4 months. Phelps et al (JSES Int 2025, Level IV systematic review) found no consensus on the optimal return-to-sport protocol, with protocols ranging from immobilisation to immediate motion.
-
Tendon elongation in the mid window. (Moderate) Marshall et al (OJSM 2016, radiostereometric) showed the repaired tendon elongates mostly at 4–8 weeks post-op with minimal change at 8–16 weeks — a biomechanical argument for caution against aggressive loading in that mid window even when motion itself is safe.
-
Incision and complications. (Moderate) Grewal et al RCT (JHS 2010): no overall functional difference single vs double incision (flexion strength slightly greater with two-incision, more minor complications with single-incision). Amarasooriya systematic review (AJSM 2020): synostosis occurred only with double incision; fixation technique did not significantly affect re-rupture. Incision choice mainly drives complication-avoidance precautions, not the ROM timeline. Re-rupture rates overall are low (0–5.6%; Garon & Greenberg 2016).
Phased rehabilitation timeline (this protocol)¶
| Phase | Window | Sling / brace | ROM / use | Strengthening / loading | Criteria to progress |
|---|---|---|---|---|---|
| I — Protected comfort motion | Week 0 → 6 | Simple sling 6 wk, off for exercises/hygiene. No hinged brace, no extension block | All motion to comfort from day 1 — active + passive flexion, extension and forearm rotation. No arc restriction | None. No resisted biceps/supination loading; hand/wrist/grip and scapular/shoulder ROM maintained | Wound healed; comfortable near-full ROM; out of sling at 6 wk |
| II — Full motion, unloaded | Week 6 → ~4 mo | Sling off | Full symmetric pain-free ROM; light everyday use | None yet — light functional use without resisted loading or lifting | Full painless ROM; wound/repair settled → begin loading ~4 mo |
| III — Strengthening & graded loading | ~4 → 6 mo | — | Full ROM maintained | Start LIGHT resisted strengthening / lifting at ~4 mo; progress gradually (isotonic curls + resisted supination → functional → job/sport-specific) | Pain-free resisted flexion/supination; strength approaching the other side |
| Return to activity | ~6 mo | — | Unrestricted | Unrestricted activity / return to sport, criterion-based | Full painless ROM; strength ≥90–100% of the other side; tolerance of job/sport-specific demands |
One-line summary: simple sling 6 weeks with all motion to comfort from day 1 (no brace, no extension block) → full unloaded motion to ~4 months → light resisted loading from ~4 months → unrestricted activity / sport at ~6 months, criterion-based.
Evidence strength flags¶
- MODERATE (biomechanical + cohort): safety of immediate/early motion with cortical-button fixation (Bisson 2007; Rose 2010; Olsen 2014; Spang 2006; Lang 2018); no clinically significant difference early vs delayed mobilisation; low overall re-rupture rates.
- MODERATE (biomechanical): tendon elongation concentrated 4–8 weeks (Marshall 2016) — supports caution on mid-window loading.
- CONSENSUS / survey-level: more conservative rehab may lower re-rupture (Rosenthal 2023); no consensus on optimal return-to-sport protocol (Phelps 2025, Level IV). The specific phase timings of this protocol are expert/consensus-derived, not trial-derived.
Overall evidence strength: Moderate. Phased timelines rest on consistent institutional protocol consensus reinforced by biomechanical studies and retrospective cohorts; few prospective RCTs of the rehabilitation progression itself, and no consensus on the optimal return-to-sport protocol.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Grewal R, Athwal GS, MacDermid JC, et al. Single vs. double incision technique for the repair of distal biceps tendon ruptures: a randomized clinical trial. J Hand Surg Am. 2010.
- Amarasooriya M, Bain GI, Roper T, et al. Complications after distal biceps tendon repair: a systematic review. Am J Sports Med. 2020.
- Keener JD. Controversies in the surgical treatment of distal biceps tendon ruptures: single versus double-incision repairs. J Shoulder Elbow Surg. 2011;20(2):S113–S125.
- Dunphy TR, Hudson J, Batech M, et al. Surgical treatment of distal biceps tendon ruptures: an analysis of complications in 784 surgical repairs. Am J Sports Med. 2017;45(13):3020–3029.
- Bisson LJ, Gurske-de Perio J, Weber AE, et al. Is it safe to perform aggressive rehabilitation after distal biceps tendon repair using the modified 2-incision approach? A biomechanical study. Am J Sports Med. 2007.
- Rose DM, Archibald JD, Sutter EG, et al. Biomechanical analysis suggests early rehabilitation is possible after single-incision EndoButton distal biceps repair with FiberWire. Knee Surg Sports Traumatol Arthrosc. 2010;19(6).
- Marshall NE, Keller RA, Okoroha K, et al. Radiostereometric evaluation of tendon elongation after distal biceps repair. Orthop J Sports Med. 2016.
- Phelps BM, Birnbrich A, Singer W, et al. Postoperative rehabilitation and return to sport criteria following distal biceps tendon rupture surgery. JSES Int. 2025. (Level IV systematic review: no consensus on optimal RTS rehabilitation.)
- Rosenthal R, Ting RS, Sher D. Management of distal biceps tendon ruptures: a survey of fellowship-trained subspecialist elbow surgeons. J Shoulder Elbow Surg. 2023;32(10).
- Olsen JR, Shields E, Williams RB, et al. A comparison of cortical button with interference screw versus suture anchor techniques for distal biceps brachii tendon repairs. J Shoulder Elbow Surg. 2014;23(11):1607–1611.
- Spang JT, Weinhold PS, Karas SG. A biomechanical comparison of EndoButton versus suture anchor repair of distal biceps tendon injuries. J Shoulder Elbow Surg. 2006.
- Lang NW, Bukaty A, Sturz GD, et al. Treatment of primary total distal biceps tendon rupture using cortical button, transosseous fixation and suture anchor: a single center experience. Orthop Traumatol Surg Res. 2018.
- Edwin ES (Spencer EE Jr), Tisdale A, Kostka K, Ivy RE. Is therapy necessary after distal biceps tendon repair? HAND. 2008;3(4).
- Rubinger L, Solow M, Johal H, et al. Return to work following a distal biceps repair: a systematic review of the literature. J Shoulder Elbow Surg. 2020;29(5):1002–1009.
- Ford SE, Andersen JS, Macknet DM, et al. Major complications after distal biceps tendon repairs: retrospective cohort analysis of 970 cases. J Shoulder Elbow Surg. 2018;27(10):1898–1906.
- Cuzzolin M, Secco D, Guerra E, et al. Operative versus nonoperative management for distal biceps brachii tendon lesions: a systematic review and meta-analysis. Orthop J Sports Med. 2021.
- Garon MT, Greenberg JA. Complications of distal biceps repair. Orthop Clin North Am. 2016. (Re-rupture 0–5.6%.)
Published rehabilitation protocols (web)¶
- Brigham & Women's Hospital — Distal Biceps Tendon Repair Rehabilitation Protocol (standard). https://www.brighamandwomens.org/assets/BWH/patients-and-families/pdfs/elbow---distal-biceps-repair-protocol.pdf
- Brigham & Women's Hospital — Distal Biceps Tendon Repair Accelerated Protocol. https://www.brighamandwomens.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/elbow-accelerated-distal-biceps-repair-protocol-bwh.pdf
- Mass General Brigham Sports Medicine — Rehabilitation Protocol for Distal Biceps Tendon Repair (rev. 10/2021). https://www.massgeneral.org/assets/mgh/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-distal-biceps-repair.pdf