Patients › Rehabilitation
Cubital Tunnel Release
Recovery after surgical decompression of the ulnar nerve at the elbow, covering both in-situ (simple) release and anterior transposition.
This protocol guides your recovery after surgical release of the ulnar nerve at the elbow (cubital tunnel release) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It explains what to expect, the precautions for the early weeks, and the exercises that keep the nerve gliding freely while everything settles. Bring this page or its PDF to your physiotherapist or hand therapist so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
Two different operations, two slightly different recoveries. The ulnar nerve can be freed in two main ways, and which one you had changes your early precautions:
- In-situ (simple) decompression: the nerve is freed where it lies, without moving it. This is the standard operation Dr Hirpara performs, and recovery is quick: gentle full movement of the elbow begins early. No rigid brace is used.
- Anterior (submuscular) transposition (the nerve lifted and re-routed to a more protected position in front of the elbow): done only in the less common situation where the nerve subluxes or dislocates over the bony bump (medial epicondyle) when the elbow bends. This needs a more careful early phase, avoiding end-range elbow bending and straightening for the first few weeks while the nerve and soft tissues settle in their new position. A simple sling may be worn for comfort only.
Follow the guidance below for the operation you had: in-situ in most cases, transposition where your nerve was unstable.
What to expect¶
For wound, swelling and scar management, see the practice's wound care guidance.
The aim of the surgery is to take the pressure off the ulnar nerve (the nerve that supplies feeling to your little and ring fingers and powers many of the small muscles of the hand). Once the pressure is relieved, the nerve begins to recover, but nerves heal slowly.
How quickly your symptoms improve depends a lot on how long the nerve was compressed and how irritated it had become before surgery. Tingling and pins-and-needles often ease first, sometimes within days or weeks. Numbness and hand strength take longer (frequently months) and the final result can continue to improve for up to a year or more after the operation. Where the nerve was very irritated for a long time before surgery, some numbness or weakness may not fully recover; the operation is then aimed at stopping things getting worse and giving the nerve its best chance.
Comparing the two operations, large reviews of the published trials have found that simple in-situ decompression and anterior transposition give similar overall results, with simple decompression tending to have fewer wound and soft-tissue complications [1][2]. The choice between them is made by your surgeon based on your nerve and your elbow.
Precautions and limitations¶
Light functional use of your hand for everyday tasks such as self-care, feeding, dressing, writing and typing is encouraged from the start, within comfort.
The early limits depend on which operation you had:
- After in-situ (simple) decompression (the usual operation): gentle full elbow, forearm, wrist and hand movement is encouraged early to keep the nerve gliding. No brace is used. Keep lifting, gripping and weight-bearing through the arm light for about the first six weeks, then build up gradually.
- After anterior transposition (only if your nerve was unstable): the elbow is protected for the first few weeks; avoid forcing it fully bent or fully straight, and avoid holding it bent for long periods, while the nerve settles in its new position. A simple sling may be worn for comfort only. Nerve glides start a little later than after a simple release (usually around two to three weeks). As with an in-situ release, keep lifting and resistance light for about the first six weeks, then build up gradually.
As a general guide, lifting and resistance strengthening are kept light until around six weeks, then built up gradually [3][4].
Leaning on the elbow (resting your elbow on a hard surface) puts pressure right over the nerve and should be avoided while it recovers.
Once your wound is healed, scar massage helps keep the skin and tissues supple over the nerve. The wound care page has more information on scar management.
These are the exercises from your handout, performed as described on each card. Start them as guided by Dr Hirpara and your therapist: the start date for the nerve glides, and any elbow range limit, depends on which operation you had.
Your exercises¶
Kieran Hirpara 4.0
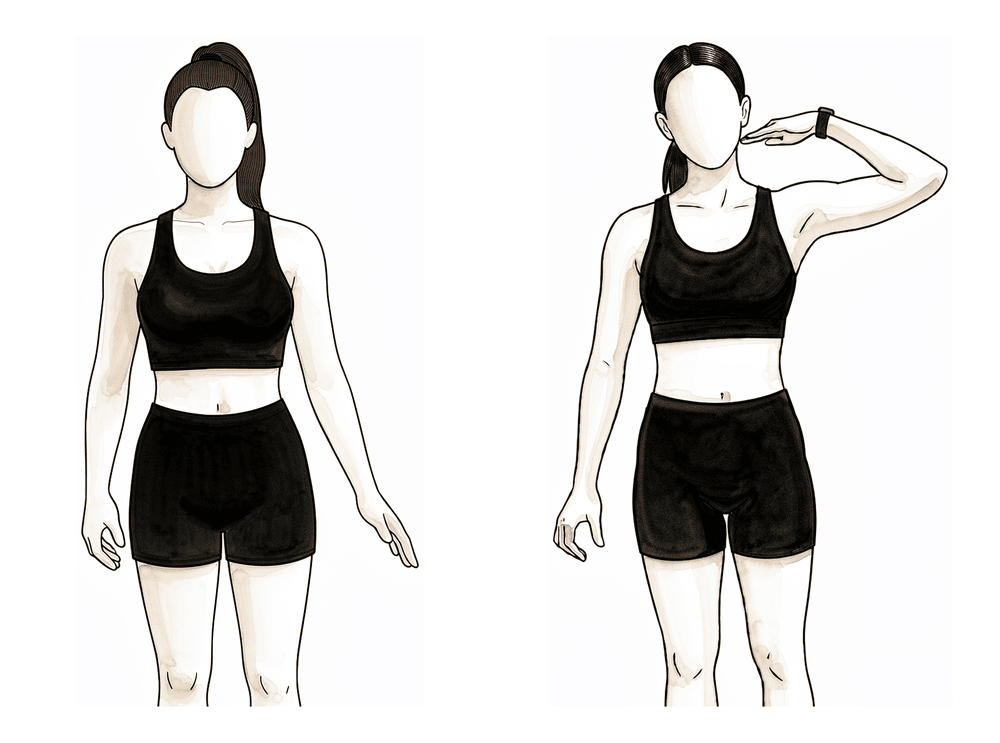
Ulnar nerve glides
These gentle movements keep the ulnar nerve sliding freely so it does not become stuck to the healing tissue. Move smoothly through each position only as far as is comfortable — a light pull or tingle is normal, but stop short of any sharp or strong pins-and-needles. Never force the stretch. Begin only when your surgeon or therapist tells you to (this is usually later if you have had a transposition — see the precautions below).
5 slow repetitions, 2–3 times daily

Kieran Hirpara 4.0
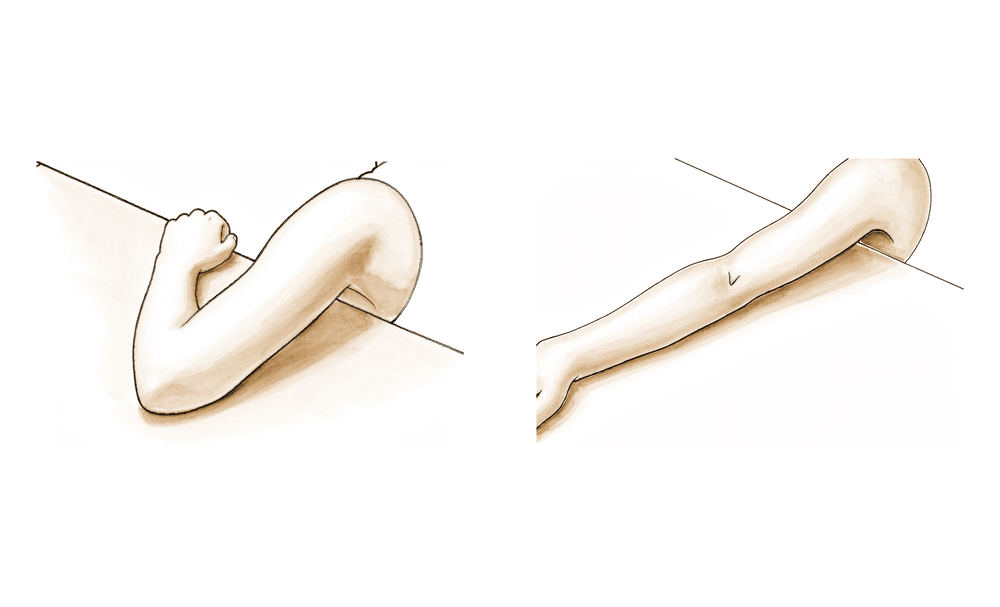
Elbow bends (flexion)
With your upper arm supported, gently bend your elbow to bring your hand towards your shoulder, then lower it again. Move within a comfortable range. If you have had a transposition, your surgeon may ask you to avoid bending the elbow all the way up for the first few weeks — follow the limit you have been given.
10 repetitions, 3–4 times daily, within your allowed range
Kieran Hirpara 4.0
Elbow straightening (extension)
From a bent position, gently straighten your elbow as far as is comfortable, then return. If you have had a transposition, avoid forcing the elbow fully straight in the early weeks if you have been asked to — settle for the comfortable range your surgeon has set.
10 repetitions, 3–4 times daily, within your allowed range
Kieran Hirpara 4.0
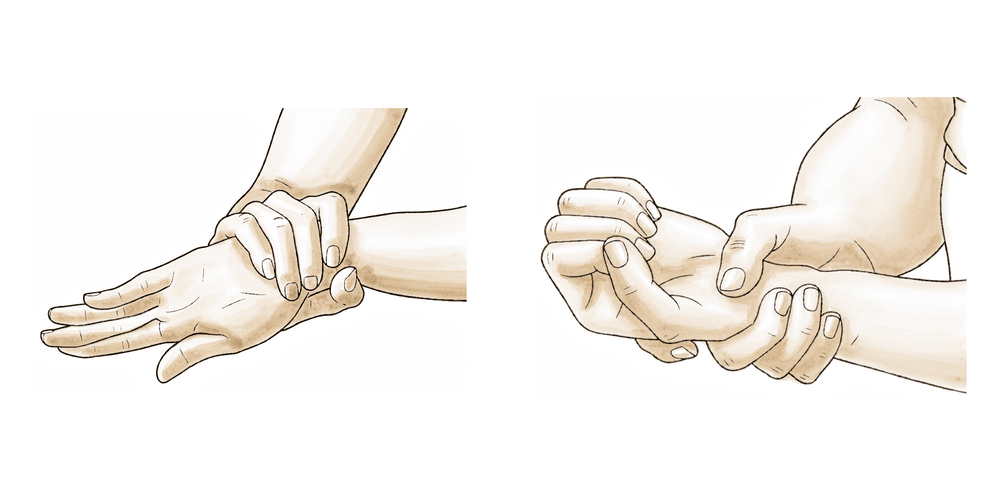
Forearm rotation
With your elbow tucked by your side and bent to a right angle, slowly turn your palm up towards the ceiling, then down towards the floor. Keep your elbow against your body throughout.
10 times each way, 3–4 times daily
Kieran Hirpara 4.0
Wrist and finger movement
Gently bend your wrist up and down, and open and close your fingers fully, making a loose fist and then spreading the fingers. This keeps the whole limb moving and helps reduce swelling and stiffness while the elbow settles.
10 of each, several times daily
Getting back to work and activity¶
Most people return to desk-based or light work within one to two weeks, while heavier, repetitive or manual roles usually take about four to eight weeks. You are ready for a particular task when your wound tolerates the contact and pressure it involves, and you can do it comfortably within the precautions above. If your work is heavy, involves leaning on the elbow, or uses vibrating tools, raise it at your post-operative review so a plan (including any modified duties) can be made.
Driving usually resumes around two to three weeks, once you are out of any sling and can control the vehicle and react in an emergency without pain. Return to sport and overhead activity is generally around six to twelve weeks.
Nerve recovery runs on a slower timeline of its own. Tingling often settles first, within days to weeks, while numbness and strength continue to improve over many months and can keep getting better for up to about a year. Where the nerve was very compressed for a long time, some numbness or weakness may not fully recover, and the operation then aims to stop things progressing.
After your protocol¶
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and hand therapy basics. The phased plan above is consistent with published evidence on decompression of the ulnar nerve at the elbow, and your ongoing recovery is guided individually by your physiotherapist or hand therapist according to how your nerve and elbow progress.
References
- Said J, Van Nest D, Foltz C, et al. Ulnar nerve in situ decompression versus transposition for idiopathic cubital tunnel syndrome: an updated meta-analysis. J Hand Microsurg. 2019;11(1):18–27.
- Macadam SA, Gandhi R, Bezuhly M, Lefaivre KA. Simple decompression versus anterior subcutaneous and submuscular transposition of the ulnar nerve for cubital tunnel syndrome: a meta-analysis. J Hand Surg Am. 2008;33(8):1314.e1–12.
- Caliandro P, La Torre G, Padua R, Giannini F, Padua L. Treatment for ulnar neuropathy at the elbow. Cochrane Database Syst Rev. 2016;11:CD006839.
- Andrews K, Rowland A, Pranjal A, Ebraheim N. Cubital tunnel syndrome: anatomy, clinical presentation, and management. J Orthop. 2018;15(3):832–836.
Evidence & references
Cubital Tunnel Release — Post-operative Rehabilitation (In-situ Decompression vs Anterior Transposition)¶
Topic scope: post-operative rehabilitation after surgical decompression of the ulnar nerve at the elbow. The single defining branch point is the operative technique: (A) in-situ (simple) decompression — an early-full-motion pathway; versus (B) anterior transposition (subcutaneous or submuscular) — a protected early phase that avoids end-range elbow flexion/extension for the first few weeks to protect the transposed nerve and its soft-tissue bed.
Defining principle of the rehab here: decompression relieves pressure on a nerve; it does not, by itself, create a load-bearing repair that needs months of protection. So the rehab is fundamentally an early-motion, nerve-glide pathway aimed at preventing perineural adhesion while the nerve recovers on its own (slow) biological timeline. The one variable that changes the early phase is whether the nerve was transposed — a transposed nerve sits in a new bed and end-range elbow excursion is restricted briefly to protect it, so nerve glides start later and elbow ROM is capped for a few weeks. Phase timings below are typical of published surgeon protocols and institutional consensus rather than trial-derived.
A. PROCEDURE CHOICE & OUTCOME EQUIVALENCE¶
- In-situ decompression and anterior transposition give equivalent clinical outcomes. Multiple meta-analyses of RCTs and comparative series find no significant difference in motor nerve conduction velocity or clinical outcome scores between simple decompression and transposition for idiopathic cubital tunnel syndrome. Strong (multiple SR/meta-analyses).
- Simple decompression carries a lower complication burden (wound, soft-tissue, devascularisation risk), and is often preferred where the nerve is stable and does not subluxate. Moderate–strong.
- Transposition is selected for nerve instability/subluxation, prior failed in-situ release, bony deformity, or a hostile cubital tunnel floor — surgeon's intra-operative judgement. Consensus.
- Endoscopic vs open in-situ decompression show comparable outcomes; choice does not change the rehab pathway (both early-motion). Moderate (SR).
B. POST-OPERATIVE REHABILITATION¶
Common principles (both pathways)¶
- Early digital, wrist and shoulder motion from day 1 to prevent stiffness and oedema.
- Ulnar nerve gliding to prevent perineural adhesion — timing differs by pathway (see below).
- No elbow leaning / direct pressure over the nerve during recovery.
- Wound: suture removal ~10–14 days; scar massage and desensitisation once healed.
- Nerve recovery is slow and graded: paraesthesia often improves first (days–weeks); numbness and intrinsic strength lag (months); final outcome continues to ~12 months. DASH, clinical findings and NCV improve postoperatively, with significant early gains by ~1 month in cohort data. Pre-operative severity/chronicity is the dominant predictor of incomplete recovery.
Phased timeline (typical of published surgeon protocols)¶
| Phase | In-situ (simple) decompression | Anterior transposition (SC / submuscular) |
|---|---|---|
| Week 0–2 | Soft dressing; early active full elbow ROM + digit/wrist/shoulder ROM; light ADLs | Splint/sling for comfort/protection (often elbow ~semi-flexed early); avoid end-range flexion AND extension, and avoid sustained/prolonged elbow flexion; digit/wrist/shoulder ROM |
| Week 2–6 | Progress to full unrestricted active ROM; scar massage + desensitisation once healed; nerve glides as tolerated | Suture out ~10–14d; gradually restore elbow ROM within set limits; scar/desensitisation; introduce nerve glides — typically deferred to this window |
| Week ~6+ | Strengthening / lifting built up as tolerated; return to full activity | Restrictions usually lifted ~6 wk; resistance strengthening from ~6 wk; build up gradually |
Dr Hirpara's practice parameters:
- Default operation = in-situ (simple) decompression; anterior submuscular transposition is reserved for a nerve that subluxates over the medial epicondyle. No rigid brace is used.
- Early elbow ROM: full active elbow motion from day 1 after in-situ decompression. After a transposition the elbow is protected from end-range flexion/extension for the first few weeks (a simple sling for comfort only — no rigid brace).
- Nerve glides: start early/as-tolerated after in-situ; start around 2–3 weeks after a transposition.
- Lifting: kept light (around ≤2 kg) for the first ~6 weeks, then resistance strengthening is built up gradually.
- Nerve recovery: paraesthesia settles first (days–weeks); numbness and intrinsic strength recover over months and can keep improving to ~12 months. Pre-operative severity/chronicity is the dominant predictor — long-standing severe compression may not fully recover, and surgery then aims to halt progression.
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Procedure equivalence is well supported (multiple meta-analyses); the complication-profile advantage of simple decompression drives the "in-situ first unless unstable" stance. Strong.
- The post-op rehab protocol itself is consensus/expert — drawn from surgeon patient-guidance protocols, not a rehab RCT. Phase timings are typical, not trial-derived. Weak/consensus.
- Nerve-glide evidence is stronger as a non-operative and adhesion-prevention measure than as a proven post-operative outcome-changer; biomechanical and clinical work supports gliding to reduce excursion-related symptoms. Moderate.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (SR / meta-analysis): clinical-outcome equivalence of in-situ decompression vs anterior transposition; lower complication rate with simple decompression.
- MODERATE (cohorts / SR): endoscopic vs open in-situ equivalence; post-op DASH/NCV improvement with early gains by ~1 month; nerve-gliding rationale.
- WEAK / CONSENSUS: the post-operative rehabilitation protocol (surgeon patient-guidance documents; no defining rehab RCT) — including the transposition early-ROM cap, nerve-glide start date, and the ~6-week lifting/strengthening threshold.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Open vs retractor-endoscopic in-situ decompression of the ulnar nerve in cubital tunnel syndrome. Neurosurgery. DOI: 10.1227/neu.0b013e3182846dbd
- Randomized, prospective study comparing ulnar neurolysis in situ with submuscular transposition. Neurosurgery. DOI: 10.1227/01.neu.0000194847.04143.a1
- Open versus endoscopic in situ decompression in cubital tunnel syndrome: a systematic review. Int J Surg. 2016. DOI: 10.1016/j.ijsu.2016.09.012
- Simple decompression vs. subcutaneous anterior transposition of the ulnar nerve (2025). J Hand Surg Glob Online / XRRT. DOI: 10.1016/j.xrrt.2025.100630
- Cubital tunnel syndrome: current concepts. Curr Rev Musculoskelet Med. 2020. DOI: 10.1007/s12178-020-09650-y
- Predictors of surgical revision after in situ decompression of the ulnar nerve. J Shoulder Elbow Surg. 2015. DOI: 10.1016/j.jse.2014.12.015
- Clinical outcomes of ulnar nerve gliding exercise in the nonoperative treatment of cubital tunnel syndrome. JSES Int. 2025. DOI: 10.1016/j.jseint.2025.02.001
- Biomechanical analysis of ulnar nerve gliding and elongation. Clin Shoulder Elbow. 2024. DOI: 10.5397/cise.2024.00934
- Postoperative improvement in DASH score, clinical findings and nerve conduction velocity in cubital tunnel syndrome. Sci Rep. 2016. DOI: 10.1038/srep27497
Comparative-effectiveness literature (URLs)¶
- Said J, et al. Ulnar nerve in situ decompression versus transposition for idiopathic cubital tunnel syndrome: an updated meta-analysis. J Hand Microsurg. 2019. https://pmc.ncbi.nlm.nih.gov/articles/PMC6431285/
- Macadam SA, et al. Simple decompression versus anterior subcutaneous and submuscular transposition of the ulnar nerve: a meta-analysis. J Hand Surg Am. 2008. https://pubmed.ncbi.nlm.nih.gov/18929194/
- Caliandro P, et al. Treatment for ulnar neuropathy at the elbow. Cochrane Database Syst Rev. 2016;CD006839. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD006839.pub4/full
- Andrews K, et al. Cubital tunnel syndrome: anatomy, clinical presentation, and management. J Orthop. 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC6082832/
Published rehab protocols (patient-guidance — basis for the phase structure)¶
- University of Virginia Orthopaedics — Cubital Tunnel Release, In-situ Rehabilitation Guidelines. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Cubital-tunnel-release-in-situ.pdf
- University of Virginia Orthopaedics — Cubital Tunnel Release, Anterior Subcutaneous Transposition. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Cubital-tunnel-release-anterior-subcutaneous-transposition.pdf
- AAOS OrthoInfo — Cubital Tunnel Release (patient recovery expectations). https://orthoinfo.aaos.org/en/treatment/cubital-tunnel-release/