Patients › Rehabilitation
Stiff Elbow Release (Arthrolysis)
An early, aggressive movement recovery plan after an operation to free up a stiff elbow — the surgeon regains the bend and straightening on the table, and the whole job of rehabilitation is to keep that range, starting from day one with no sling and no protection phase.
This protocol guides your recovery after an operation to free up a stiff elbow (a release, or arthrolysis) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your physiotherapist or hand therapist; bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
A stiff elbow after a previous injury or operation happens because the lining (capsule) of the joint thickens and tightens, and sometimes extra bone forms, so the elbow can no longer bend and straighten through its full arc. During the release operation, done either with keyhole (arthroscopic) surgery or through an open incision, the surgeon removes that tight capsule (and any extra bone or trapped scar) so the elbow moves freely again on the operating table.
The single most important thing to understand is that this recovery is the opposite of a repair operation. There is nothing that has been stitched or fixed that needs weeks of rest to heal. Instead, the surgeon establishes a near-full range of movement during the operation, and the whole job of your rehabilitation is to keep that movement, because the elbow's natural tendency after surgery is to stiffen up again. That is why there is no sling and no protection phase: you start moving the elbow on the first day, and you move it firmly and often. The enemy here is re-stiffening, not tissue failing.
For wound, swelling and scar management, see the practice's wound care guidance. Swelling and pain are the main things that hold movement back in the early days, so controlling them with elevation, ice and your pain relief is an important part of keeping your range.
Most of your improvement happens between about 6 weeks and 3 months, and the elbow usually reaches its best, settled range at around 4 months. To hold and even add to your range, a splinting program is used at night and rest times and is continued for at least 3 months.
Precautions and limitations¶
- Do start moving the elbow on day one, and keep moving it little and often throughout the day: this is the core of your recovery.
- Do push gently into the end of each stretch; unlike a repair, there is no construct to protect, so reaching the range is the goal.
- Do keep on top of swelling and pain with elevation, ice and your prescribed pain relief: they are what limit your movement, not the surgery itself.
- Do take any anti-inflammatory medication (such as indomethacin) exactly as prescribed if Dr Hirpara has started it to discourage extra bone forming.
- Do wear your night/rest splint as directed, for at least 3 months, to hold and build on the range you gain.
- Do not rest the elbow or "take it easy" to let it settle: that is how the stiffness comes back.
- Do not be alarmed by pins and needles or tingling into the little and ring fingers; the nerve on the inside of the elbow (the ulnar nerve) can become more sensitive as your bend improves, so let Dr Hirpara or your therapist know so it can be reviewed.
Your exercises¶

Kieran Hirpara 4.0
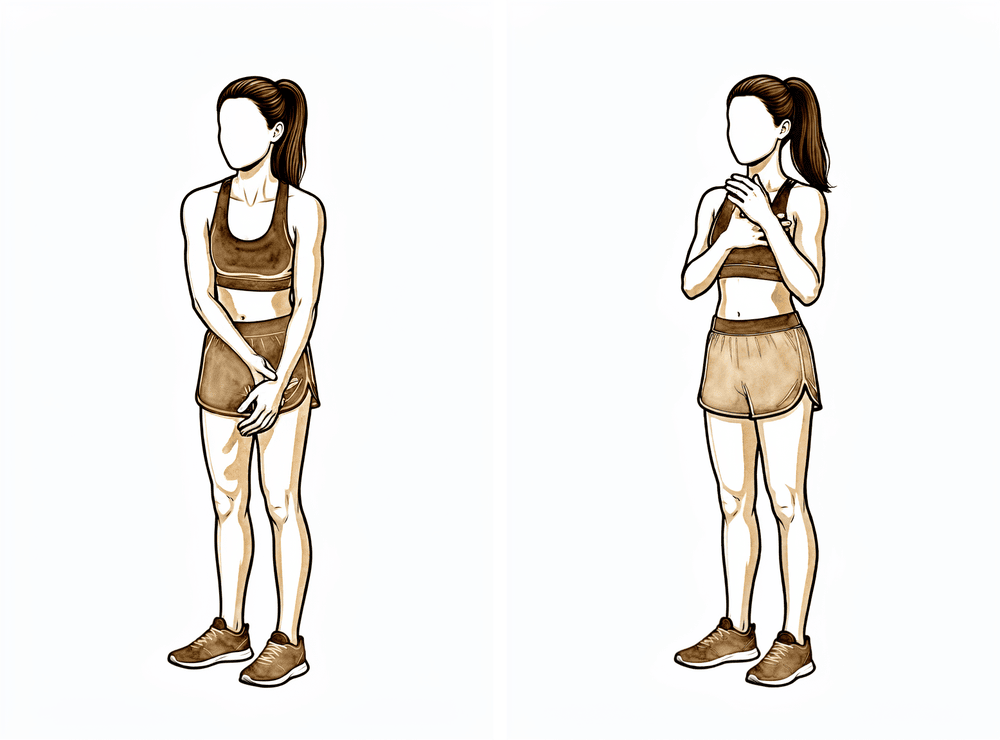
Active elbow bends (bending and straightening)
Using your own muscles, bend the elbow up as far as it will go towards your shoulder, then straighten it out as far as you can. Push gently into each end of the movement and try to reach the same range the surgeon achieved during your operation. This is the single most important exercise — the elbow re-stiffens quickly, so it is done little and often through the day.
10–15 times each direction, every 1–2 hours while awake
Kieran Hirpara 4.0
Assisted (passive) elbow bend
With the operated arm completely relaxed, use your other hand to gently push the elbow further into a bend than it will go on its own, holding at the end where you feel a firm stretch. There is no repair to protect, so you are encouraged to push gently into the stretch — hold it, breathe, and let the elbow ease a little further. Stop short of sharp pain.
Hold each stretch 20–30 seconds, 3–5 times, several times a day
Kieran Hirpara 4.0
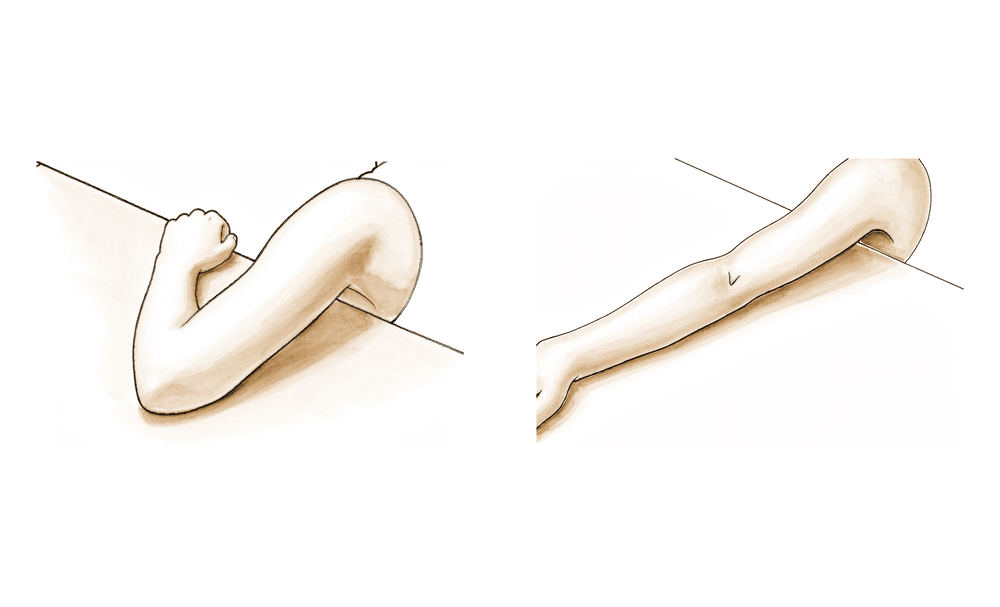
Active elbow straightening (extension)
Work on getting the elbow as straight as you can — straightening (extension) is the movement most commonly lost, so it gets extra attention. Rest the back of your upper arm on a firm surface and let gravity, then gentle help from your other hand, ease the elbow towards fully straight. Hold at the end of the stretch.
Hold 20–30 seconds, 5 times, several times a day
Kieran Hirpara 4.0
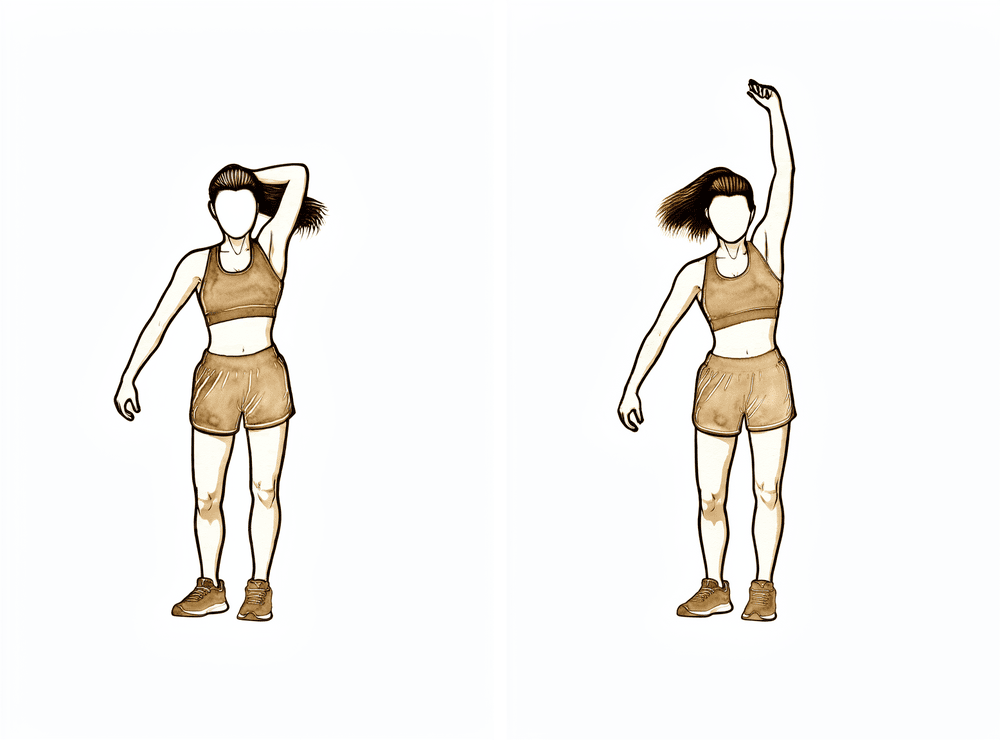
Overhead triceps stretch (end-range straightening)
Raise the operated arm overhead and gently use your other hand to push the elbow towards fully straight, stretching the back of the upper arm. This is a strong end-range stretch into straightening — hold it steady rather than bouncing.
Hold 20–30 seconds, 3–5 times, a few times a day
Kieran Hirpara 4.0
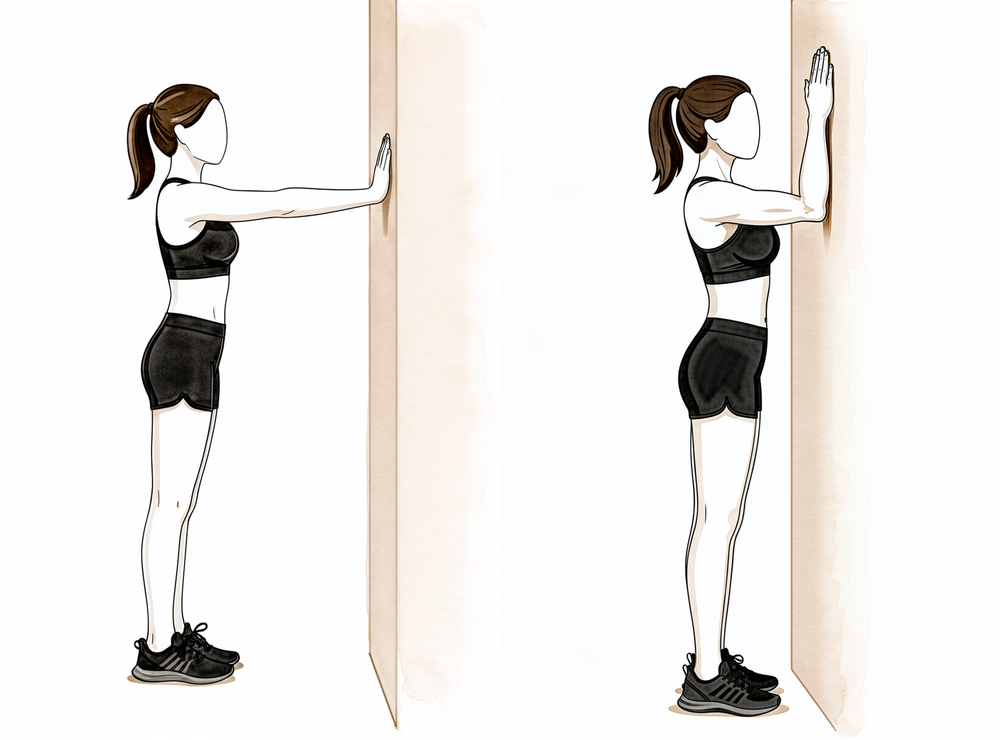
Wall walk into a bend (end-range flexion)
Face a wall and walk your fingers up it, letting the elbow bend further as your hand climbs. Walk up until you feel a firm stretch deep in the elbow, hold, then walk a little higher. This helps recover the last part of the bend.
Hold 20–30 seconds at the top, 5 times, a few times a day
Kieran Hirpara 4.0
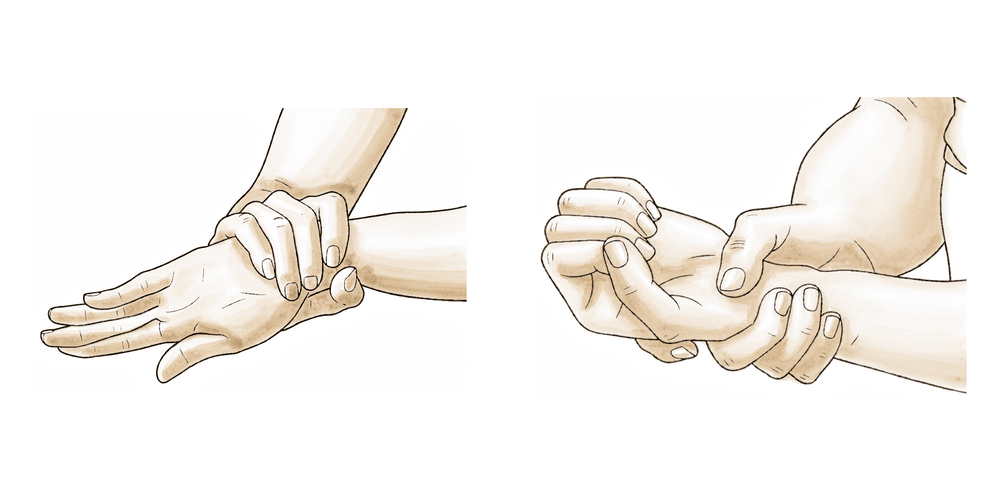
Forearm rotation (palm up / palm down)
With your elbow tucked at your side and bent to about 90°, turn your palm up towards the ceiling, then down towards the floor, going as far as you can each way. A release operation often frees rotation as well as bending, so keep this moving fully alongside your bend and straighten work. You may use your other hand to gently push a little further at each end.
10–15 times each direction, several times a day

Kieran Hirpara 4.0
Triceps muscle-set (gentle hold)
An early activation exercise. With the arm supported, gently tighten the muscle on the BACK of your upper arm (the triceps) as though to straighten the elbow, helping to hold and reinforce the straightening you have gained. Keep it gentle and as guided by your physiotherapist.
Hold ~5 seconds, 5–10 times, as guided
Kieran Hirpara 4.0
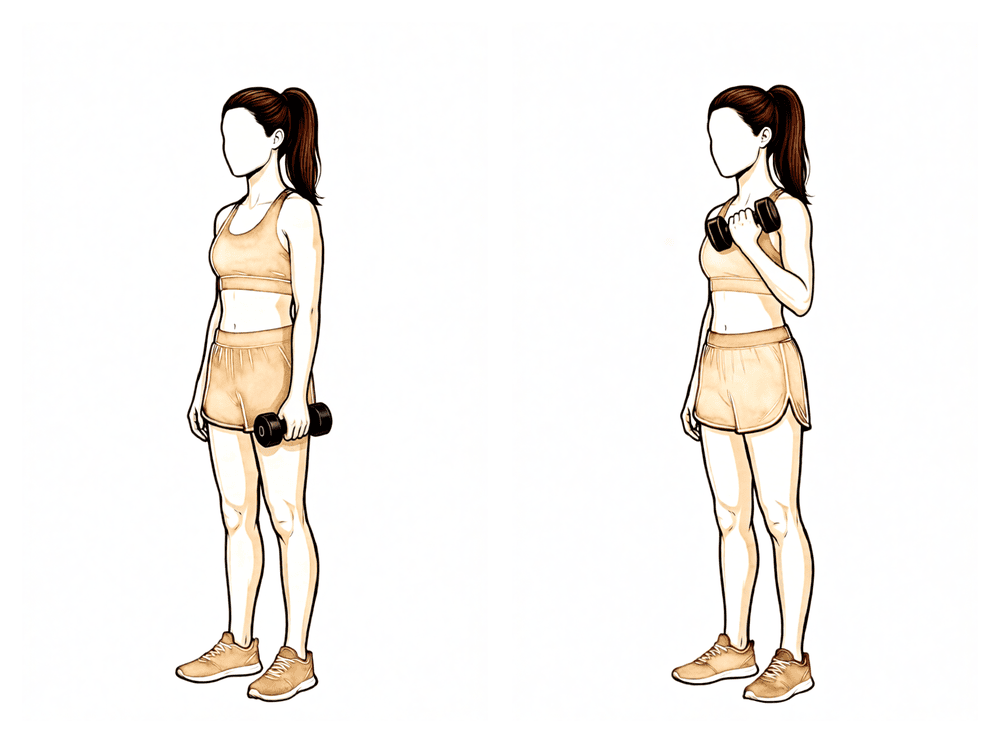
Biceps curl (later strengthening)
A LATER exercise — strengthening starts only once your movement is stable, usually from around 6 weeks. With your palm up, curl a light weight towards your shoulder, then lower it slowly under control. Build the weight up gradually as guided by your physiotherapist.
As guided by your physiotherapist (from about week 6)
These are the exercises from your handout for regaining and holding the movement of your elbow and forearm. Start them as guided by Dr Hirpara and your therapist; in this protocol they begin straight away. They are done firmly and often, because the range you keep is the range you use through these exercises every day.
Your clinical protocol¶
The rest of this page is the clinical protocol for rehabilitation after surgical release (arthrolysis) of a stiff elbow. This section is to be provided to your physiotherapist or hand therapist, and each phase below opens with a plain-English explanation of what is happening. The overriding principle is that the surgeon establishes a near-full arc on the table; rehabilitation's job is to not lose it. There is no fixation to protect and therefore no protection phase: pain and oedema control are the rate-limiters, not tissue healing.
Day 0 to 2 after your operation¶
In the first day or two the elbow is rested briefly, the arm is kept elevated, and swelling is controlled with ice and compression. The elbow is often supported in a fully straight (extension) position, because straightening is the movement most commonly lost and the one to bias towards. If extra bone formation is a concern (for example after removal of extra bone, or a high-energy original injury), Dr Hirpara may start an anti-inflammatory medication now to discourage it.
For your physiotherapist:
Prior to treatment, check the patient's imaging, operation report and past medical history (PMHx), and liaise with the treating surgeon regarding the intra-operative arc achieved, any ulnar nerve procedure, and whether heterotopic ossification (HO) prophylaxis has been started.
Position and oedema
- Brief immobilisation in full extension in a padded splint; arm elevated; cryotherapy/compression for oedema
- Drains typically removed POD1
HO prophylaxis (if indicated)
- Indomethacin (e.g. 25 mg TID, or 75–100 mg/day) for 3–6 weeks where indicated, especially after HO excision or high-energy trauma; ± single-dose perioperative radiotherapy in selected high-risk cases (surgeon's decision)
Day 1 onward — immediate aggressive range of motion¶
This is the core of the protocol. The splint comes off on the first day after surgery and firm, frequent movement begins: active-assisted and passive bending, straightening and forearm rotation, aiming to recover the full range the surgeon achieved on the table. There is no range ceiling: the goal is the full intra-operative arc.
For your physiotherapist:
ROM ceiling
- None. Recover the full intra-operative arc. Splint off POD1.
Exercises
- Active-assisted and passive ROM in flexion, extension, pronation and supination; bias the stretch toward the tightest direction (usually extension)
- Optional CPM: if used, start in-hospital POD1–2 at full available range (commonly cited 0–145° with a bolster behind the elbow) and continue at home to ~4 weeks, in addition to PT. CPM is an adjunct only and has not been shown superior to supervised PT; use is at the surgeon's discretion.
- Cadence: daily supervised PT in the first post-operative week, then 2–3×/week for ~6 weeks
Criteria to progress
- Maintaining the on-table arc; oedema and pain controlled
Weeks 2 to 6 — hold the arc and introduce splinting¶
Movement continues firmly. To hold and build on the range, a splinting program is added at night and rest times: a low-load, prolonged stretch held at the end of range, alternating between bend and straighten.
For your physiotherapist:
Exercises and splinting
- Continue aggressive active / active-assisted / passive ROM
- Add static-progressive (or dynamic / serial-static / turnbuckle) splinting for low-load prolonged end-range stretch: a night/rest program alternating flexion and extension. Static-progressive (inelastic, patient-adjusted incremental torque) is the favoured modality for elbow flexion contractures.
- Oedema and scar management
Criteria to progress
- Arc maintained or exceeded; ready for loading by ~week 6
Weeks 6 to 12 — strengthening and continued splinting¶
Once movement is stable, usually around 6 weeks, strengthening begins with progressive resistive exercise as tolerated. The splinting program continues.
For your physiotherapist:
Exercises and splinting
- Begin progressive resistive strengthening once motion is stable (typically ~6 weeks)
- Continue splinting for at least ~3 months post-operatively for optimal final ROM
Around 16 weeks — plateau¶
Published series report patients reach their maximum arc of motion at a mean of about 16 weeks, with most recovery occurring between 6 weeks and 3 months. This expectation should be set pre-operatively. Final maintained gains in the bend/straighten and rotation arcs are typically held long term (around 15-month follow-up in large cohorts).
For your physiotherapist:
- Maximum arc reached at a mean of ~16 weeks; counsel that no pre-operative range threshold reliably predicts the recovery trajectory; apply the same ~16-week timeline to all patients
Getting back to work and activity¶
Because there is no fixation to protect, getting back to everyday activity is paced by your comfort, swelling and the range you are holding rather than by waiting for something to heal. Light use of the arm for daily tasks is encouraged from the start; in fact, using the elbow normally through the day is part of the treatment.
Strengthening, and with it heavier and more demanding tasks, starts from about 6 weeks once your movement is stable, and is built up gradually as your strength and range allow. Most people reach their settled range and function by around 4 months, and the gains achieved are typically held long term. Return to driving, work duties and sport depends on regaining enough movement, strength and control for the specific task; discuss the timing for your situation with Dr Hirpara and your therapist, as it varies with your job and the extent of your surgery. The most important message is to keep up your movement and night/rest splinting program throughout, as that is what protects the range you have worked to regain.
After your protocol¶
This protocol works alongside the practice's general recovery advice: see managing post-operative pain and wound care. For a related elbow recovery where the joint lining is released, see capsular release. The phased plan above is consistent with published evidence on rehabilitation after elbow contracture release, and your ongoing recovery is guided individually by your physiotherapist or hand therapist according to how your elbow progresses.
Evidence & references
Stiff Elbow — Arthrolysis / Capsular Release (Open or Arthroscopic) — Rehabilitation Evidence¶
Topic scope: rehabilitation after surgical release of the post-traumatic / post-surgical stiff elbow — open or arthroscopic arthrolysis, anterior + posterior capsulectomy, ± heterotopic ossification (HO) excision, ± ulnar nerve decompression. The focus here is the post-operative rehabilitation philosophy and timeline, not the indications for or technique of the release itself.
Defining principle: the surgeon establishes a near-full arc of motion on the operating table; rehabilitation's single job is to not lose it. There is no fixation to protect, so — unlike a fracture fixation or a tendon repair — there is no protection phase. Motion starts essentially Day 1 (or even in-hospital CPM from Day 1–2), pushed firmly and often. Pain and oedema control are the rate-limiters, not tissue healing. This is the opposite philosophy to olecranon ORIF or a distal biceps repair. Dr Hirpara's stance: no sling and no immobilisation phase; immediate aggressive active-assisted and passive ROM from POD1; static-progressive (or dynamic) night/rest splinting continued for at least 3 months; HO prophylaxis where indicated; and a frank pre-operative conversation that the elbow reaches its plateau at a mean of ~16 weeks.
Consensus phased timeline (week windows)¶
| Phase | Window | Immobilisation / "ceiling" | Movement & adjuncts | Strengthening | Criteria to progress |
|---|---|---|---|---|---|
| Immediate | Day 0–2 | Brief splint in full extension; arm elevated, cryotherapy/compression | HO prophylaxis decision made now (see below); drains out POD1 | — | Splint off POD1 |
| Immediate aggressive ROM (core) | Day 1 onward | No ROM ceiling — recover the full intra-operative arc | Active-assisted + passive flexion / extension / pronation / supination; bias toward tightest direction (usually extension). Optional CPM 0–145° with bolster, in-hospital POD1–2, home to ~4 wk. Daily PT first week → 2–3×/wk for ~6 wk | — | On-table arc maintained; oedema/pain controlled |
| Hold the arc + splinting | Weeks 2–6 | None | Continue aggressive A/AAROM/PROM. Add static-progressive (or dynamic / serial-static / turnbuckle) splinting — low-load prolonged end-range stretch, night/rest, alternating flexion/extension | — | Arc maintained or exceeded; ready for loading ~wk 6 |
| Strengthening + continued splinting | Weeks 6–12 | None | Continue splinting | Progressive resistive strengthening once motion stable (~wk 6); continue splinting ≥3 months | Stable, strengthening motion |
| Plateau | ~16 weeks (≈4 months) | None | — | Maintain gains; long-term hold | Maximum arc reached; most recovery occurred 6 wk–3 mo |
Evidence summary by theme¶
Immediate aggressive motion — the agreed principle (Strong consensus)¶
Large, consistent retrospective case series and review articles agree that the elbow re-stiffens without immediate motion, and that rehabilitation exists to hold the intra-operative arc. Motion begins POD1; the splint (when used) is removed POD1 and active-assisted + passive ROM is started in all planes, biased toward the tightest direction (usually extension). This is strong consensus across the literature.
Which specific rehab protocol is best (Moderate — genuine equipoise)¶
The best specific rehab protocol is genuinely unknown. No completed RCT shows superiority of CPM vs PT vs delayed PT — the SET-Study (Stiff Elbow Trial) was designed precisely because this question is unresolved, with three real-world arms (in-hospital CPM + early PT / in-hospital early PT / outpatient PT from POD7–10). CPM is cited in protocols (home use to ~4 weeks) and one arthroscopic- release series reports very good 3-year outcomes with a 4-week CPM rail plus PT, but CPM has never been shown superior to supervised PT alone. So: strong consensus on aggressive early motion; weak/equipoise evidence on which adjunct.
Splinting modality (Moderate — no clear winner)¶
Static-progressive, dynamic, serial-static and turnbuckle splinting all deliver low-load prolonged end-range stretch. The Lindenhovius RCT found no difference between dynamic orthoses and static-progressive splinting (similar DASH). Static-progressive (inelastic, patient-adjusted incremental torque) is the favoured modality for elbow flexion contractures. Reviews recommend the splinting program run for at least ~3 months post-operatively for optimal final ROM. Bracing alone can rival surgery for non-osseous stiffness with far lower neurovascular risk.
HO prophylaxis (Consensus — extrapolated evidence)¶
Indomethacin (commonly 25 mg TID, or 75–100 mg/day, for 3–6 weeks) ± single-dose perioperative radiotherapy is widely used after release, especially with HO excision or high-energy trauma. Most HO-prophylaxis RCT evidence is extrapolated from acetabular/hip surgery, not elbow-specific. Recurrent HO / arthrofibrosis responds to repeat excision + release.
Recovery trajectory and plateau (Moderate — cohort data)¶
Published series report patients reach their maximum arc of motion at a mean of ~16 weeks, with most recovery occurring between 6 weeks and 3 months, and maintained gains at ~15-month follow-up in large cohorts. Growth-mixture modelling found no pre-operative ROM threshold or factor reliably predicted the recovery trajectory — so all patients are counselled on the same ~16-week timeline pre-operatively.
Ulnar nerve (Consensus)¶
As flexion improves post-release, the ulnar nerve sees increased stress — there should be a low threshold for review, and for concomitant ulnar nerve decompression/transposition at the time of surgery. Tobacco use predicts poorer outcomes and higher complication rates after open arthrolysis.
Evidence strength flags (summary)¶
- STRONG (consensus across case series/reviews): immediate aggressive active-assisted + passive motion from POD1 to hold the intra-operative arc — no protection phase.
- MODERATE (RCT/cohort, equipoise): which adjunct is best — CPM vs PT vs delayed PT (SET-Study, no completed superiority data); splinting modality (Lindenhovius RCT: no difference dynamic vs static-progressive); ~16-week plateau and maintained gains (growth-mixture-modelling and large open-release cohorts).
- CONSENSUS / EXTRAPOLATED: HO prophylaxis (indomethacin ± single-dose RT; most evidence extrapolated from acetabular/hip surgery); ≥3-month splinting program duration.
Overall topic flag: MODERATE — strong consensus on the principle (aggressive early motion + adjunct splinting + HO prophylaxis), weak/equipoise evidence on the specific adjunct.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Sun Z, Wang W, Fan C. Tobacco use predicts poorer clinical outcomes and higher post-operative complication rates after open elbow arthrolysis. Arch Orthop Trauma Surg. 2019.
- Open elbow release for post-traumatic stiffness — growth-mixture-modelling cohort: maximum arc of motion at a mean of ~16 weeks, most recovery between 6 weeks and 3 months.
- 103-patient open capsular release series — significant, maintained flexion/extension and supination/pronation arc gains at a mean of 15 months.
- Papatheodorou LK, Sotereanos DG (University of Pittsburgh) — elbow contracture release techniques review.
- Lindenhovius et al. RCT — no difference between dynamic orthoses and static-progressive splinting (cited within a retrieved review).
- Retrieved technique text: indomethacin 25 mg TID for ~6 weeks for HO prophylaxis; CPM continued at home up to 4 weeks, full range 0–145° with a bolster behind the elbow.
- Northwestern series — HO excision + contracture release: ROM gains and complications.
- Arthroscopic release + 4-week CPM rail series — very good ROM, function and quality of life at a mean of 3 years.
Published protocols / reviews (URLs)¶
- Papadopoulos et al. Elbow contracture release. Annals of Joint (PT from POD1; flexion bias the first 2 weeks then full ROM over 2–3 months; dynamic / static-progressive splinting ≥3 months; CPM optional). https://aoj.amegroups.org/article/view/6083/html
- SET-Study (Stiff Elbow Trial) protocol — CPM vs PT vs delayed PT RCT; documents that the best rehab protocol is unknown. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5700741/
- Analysis of Long-Term Outcomes Following Surgical Contracture Release of the Elbow — immediate splint in full extension, splint off POD1, AAROM started POD1, OT/PT-guided self-directed program, no CPM. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8152451/