Patients › Rehabilitation
Latarjet Procedure
Rehabilitation protocol after the Latarjet coracoid bone-block transfer for anterior shoulder instability — union-gated loading and subscapularis/graft precautions.

This protocol guides your recovery after a Latarjet procedure with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It pairs a plain-English explanation of each stage with a structured programme you can share with your physiotherapist; bring this page or its PDF to your first appointment so your rehabilitation stays coordinated. Your physiotherapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
A Latarjet is a bone-block operation for a shoulder that keeps dislocating at the front. Because it uses solid bone fixed with screws (rather than only stitched-up soft tissue), the repair is sturdy early, and your recovery is generally faster than for a soft-tissue stabilisation (a Bankart repair). On average, people return to sport at around 20 weeks, compared with roughly 32 weeks after a Bankart.
But "faster" does not mean "anything goes". The pace of your recovery is set by one thing above all: the transferred bone healing onto your shoulder socket. This bony join (called union) usually takes about 6 to 8 weeks. Until your surgeon confirms it has united, loading the shoulder is held back, no matter how good the arm feels. The Latarjet also has two extra structures to protect that a Bankart does not, which is why some of the early restrictions below are specific to this operation.
The procedure¶
In a Latarjet, a small piece of bone called the coracoid (a bony bump at the front of your shoulder blade) is moved across and fixed with screws to the front rim of your shoulder socket, where bone has been lost. This adds bone where it was missing and creates a "sling" effect at the front of the shoulder that helps stop it dislocating.
To move that bone into place, the surgeon has to pass it through the subscapularis (a muscle at the front of the shoulder), which is split, or partly detached and then repaired. Two things therefore need protecting while they heal:
- the bone block and its screws, which must knit onto your socket (union, about 6–8 weeks); and
- the subscapularis muscle at the front, which is repaired around the transferred bone.
Some people are left with a small permanent loss of outward-rotation range (turning the hand outward) of roughly 7–8 degrees. This is expected and is not a complication; for most people it makes no difference to daily life.
Wearing your sling¶
You will wear a simple shoulder sling, not an abduction-pillow or wedge sling. Dr Hirpara uses a simple sling for stabilisation surgery, because the bone fixation is sturdy and protection comes mainly from keeping the arm in a safe position, not from the sling's shape.
- Wear the sling for about 3 weeks for daytime support and comfort (it is weaned off from about week 3). The bony Latarjet needs a shorter time in a sling than a soft-tissue repair.
- You do not sleep in the sling. Sleep with it off; keep your arm in a safe position while you are asleep: do not let it fall out to the side and turned outwards (the position the operation is protecting against). Lying with the arm supported on a pillow across your body or by your side is comfortable and safe.
- Take it off for showering and for your exercises (once you have been shown how). Whenever the sling is off, keep your arm relaxed and by your side.
- Use ice if the shoulder is swollen or sore, especially after exercise.
Watch your posture while you are using the sling: keep your ears, shoulders and hips in line and avoid slumping.
Key precautions — do NOT¶
These protect the bone block, its screws, and the front muscle while they heal.
- Do NOT force the arm into outward rotation (turning the hand outward) early. In the first 2 weeks, outward rotation is kept to about 25 degrees in a supported position, and only opened up gradually after that, always within the range your surgeon sets.
- Do NOT push the arm backwards behind your body (shoulder extension), and avoid the combined position of the arm turned outward and stretched backwards. This pulls on the tendon attached to the transferred bone.
- Do NOT do resisted inward-rotation strengthening early (pressing the hand hard inwards across the body against resistance). This works the healing front muscle (subscapularis) and is held back until your surgeon agrees.
- Do NOT bear weight through the arm or hand, push up from a chair with the arm, or lift, push or pull anything heavy until your surgeon confirms the bone has united (about 6–8 weeks). The bony join, not the calendar, decides when heavier loading can begin.
- Do NOT do heavy chest or overhead gym work early: no pec flys, wide-grip bench press, military (overhead) press, behind-the-neck lat pulldowns or triceps dips until late in your recovery.
- Avoid any sudden jerk, grab or fall onto the arm.
Phase I — Immediate protection (weeks 0–2)¶
Kieran Hirpara 4.0
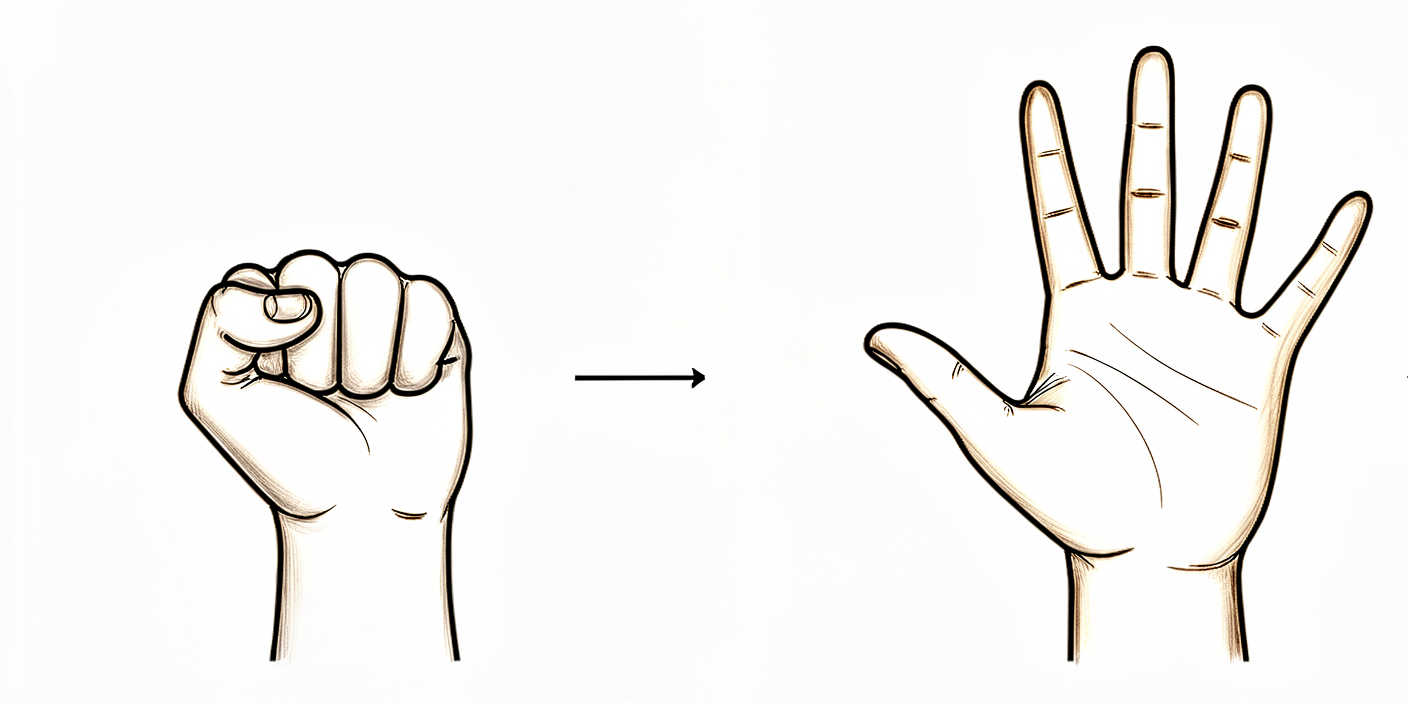
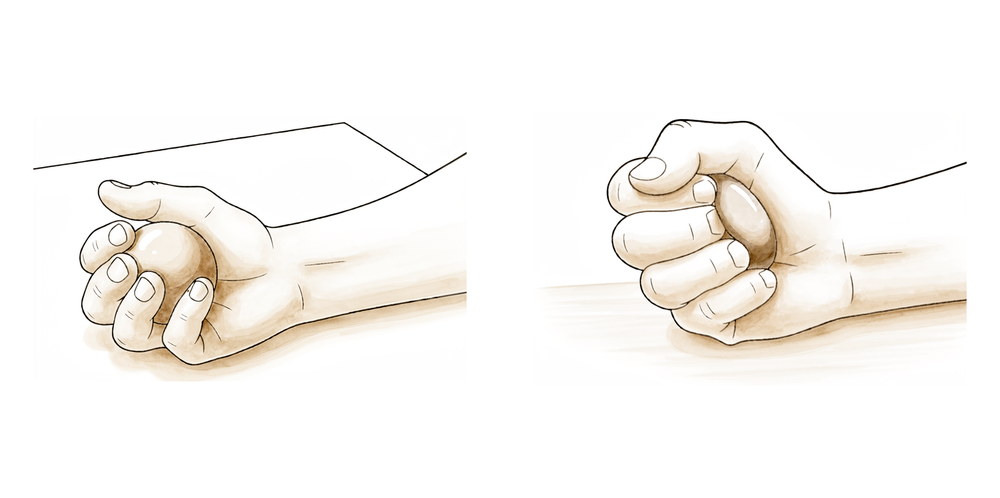
Open and close hand
Make a tight fist with your hand, then open it fully. This keeps your hand moving and helps prevent stiffness and swelling.
10 times per hour
Kieran Hirpara 4.0
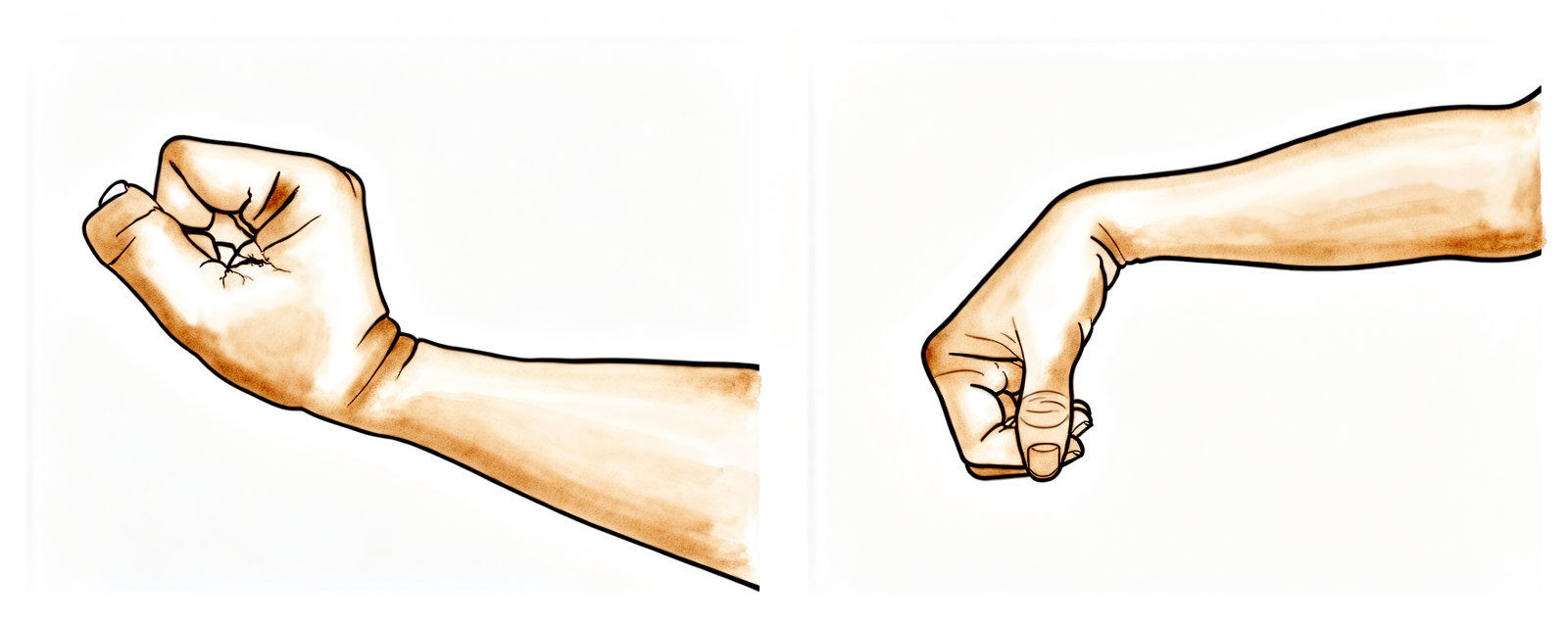
Active wrist bends
Gently bend your wrist forwards, then back, as far as is comfortable.
10–15 times per hour

Kieran Hirpara 4.0
Active elbow bends
With your palm facing up, gently bend your elbow as far as you can, then straighten your arm again. Keep your upper arm tucked at your side. Do NOT let the arm swing backwards behind your body.
10–15 times, 2–3 times a day
Kieran Hirpara 4.0
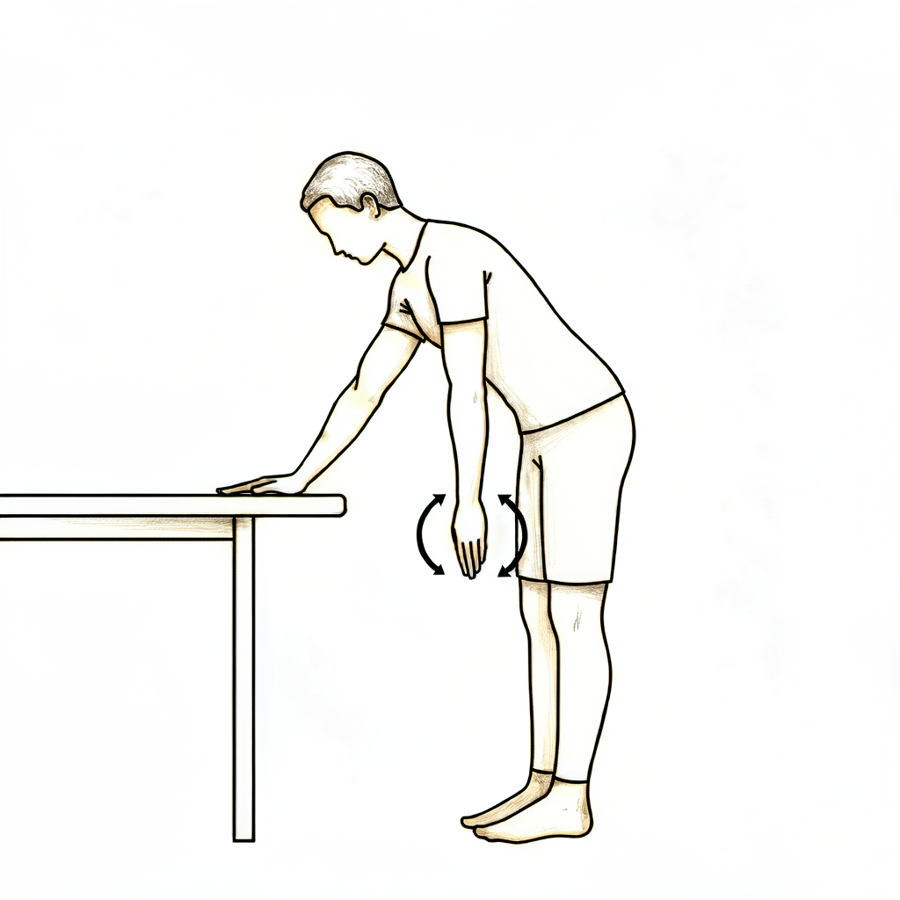
Pendulum swings
Lean forwards and let your operated arm hang down, completely relaxed. Make small circles — clockwise, then the other way — by rocking your body, NOT by using your shoulder muscles. Keep the circle small (under about 20 cm). Your operated arm stays relaxed throughout — you are not lifting it. Do NOT let the arm drift backwards behind your body.
10 in each direction, 2–3 times a day
Kieran Hirpara 4.0
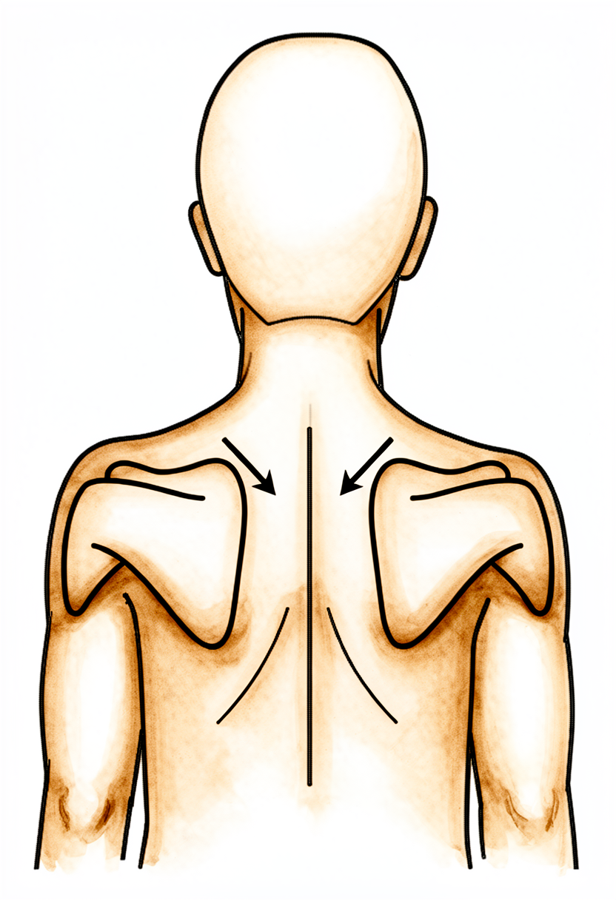
Shoulder-blade setting
Gently squeeze your shoulder blades downwards and together, hold, then relax. This is a light muscle-activation drill — your arm does not move.
Hold 5 seconds, 5 times, 2–3 times a day
Kieran Hirpara 4.0
Ball squeeze
Hold a soft ball or rolled-up sock in your hand and squeeze gently, then relax. This keeps the hand and forearm active while the shoulder rests.
10 times, 2–3 times a day
The first two weeks are about protecting the freshly transferred bone block and the repaired front muscle while the swelling settles. You wear the simple sling in the day, sleep out of it (keeping the arm in a safe position), and do gentle drills that keep your hand, wrist and elbow moving without stressing the shoulder. The shoulder itself is moved only gently and passively; you do not lift the arm under its own power yet.
- Sling: simple sling for daytime support and comfort; sleep OUT of the sling with the arm in a safe position; off for exercises and hygiene.
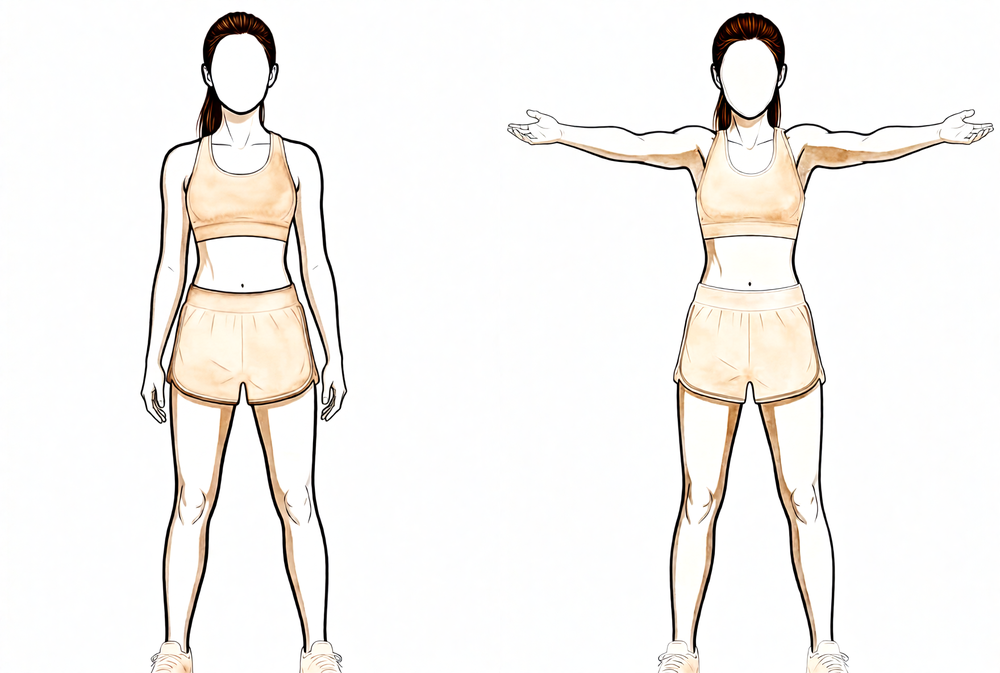
- Movement allowed: gentle assisted and passive movement only; no lifting the arm under your own shoulder power. Forward elevation and reaching out to the side to comfort; outward rotation kept to about 25 degrees in a supported position; do not push the arm backwards behind the body.
- Exercises: shoulder-blade setting; ball squeeze; gentle hand, wrist and elbow movement; pendulum swings (arm relaxed, not drifting backwards).
Ready for the next phase when: your pain is settling and controlled with simple pain relief; your wound has healed with no signs of a problem; you are comfortable out of the sling; and your gentle movement stays within the safe range your surgeon has set.
Phase II — Restoring movement (weeks 3–9)¶
Kieran Hirpara 4.0
Full-can lift to shoulder height
From about week 6, once you are moving the arm under your own power. Raise your arm forwards and slightly out to the side with your THUMB POINTING UP — the "full can" position — only up to about shoulder height (90°) at first, then lower with control. Use no weight or a very light weight (about 1–1.5 kg) and many repetitions.
As guided by your physiotherapist
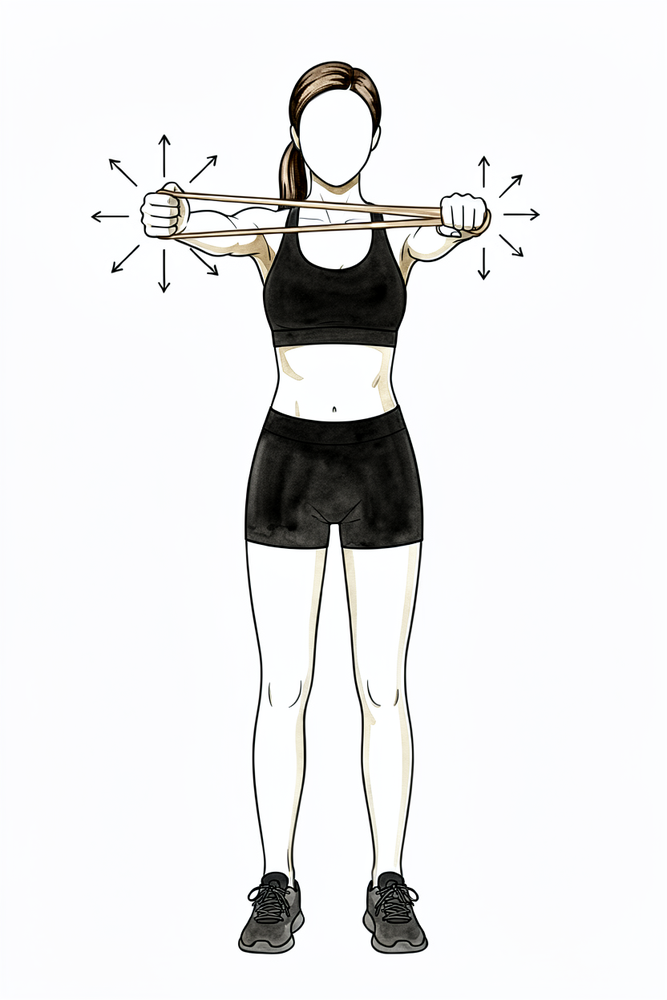
Kieran Hirpara 4.0
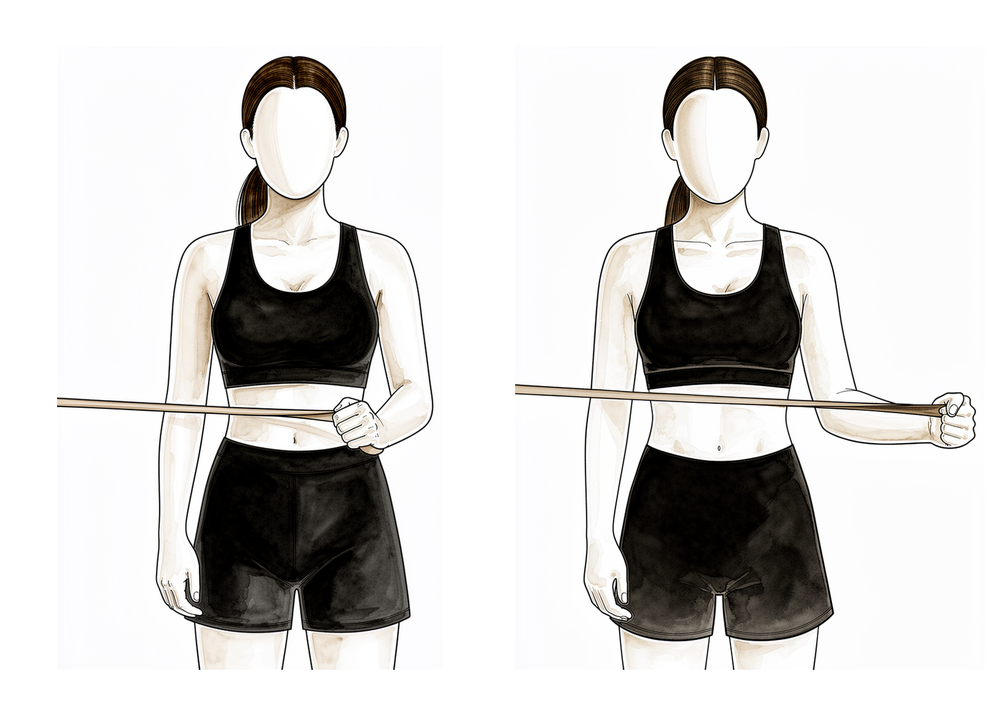
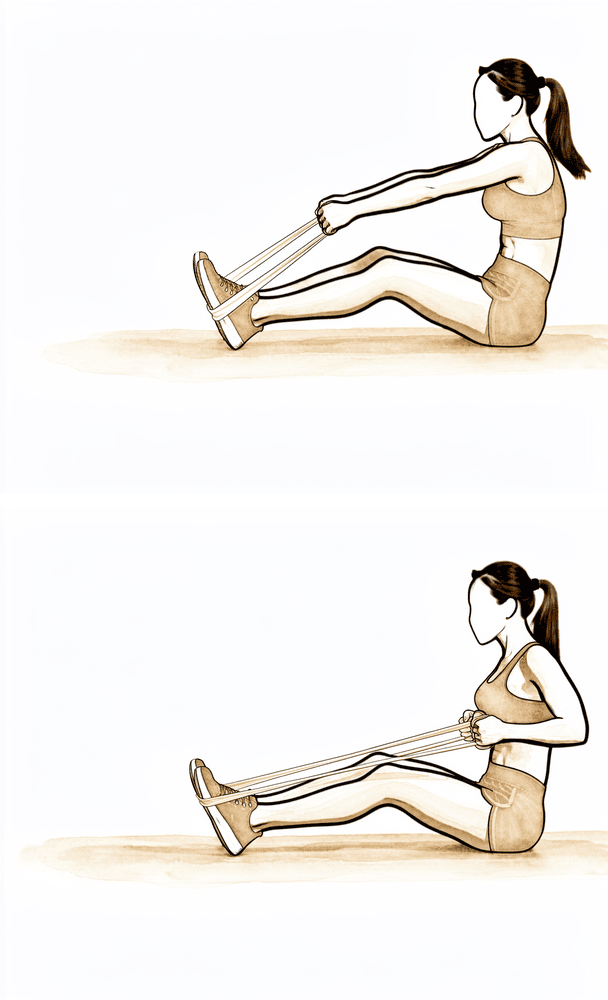
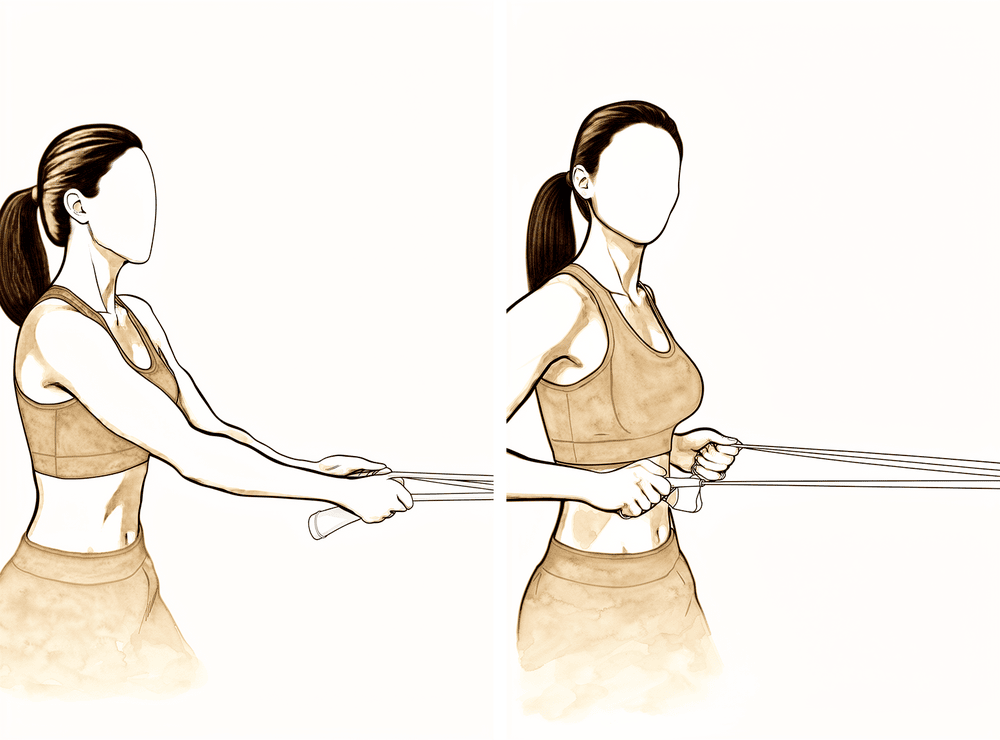
External rotation at the side (band)
From about week 6, within the outward-rotation range your surgeon has set. Tuck your elbow at your side with a rolled towel between your elbow and your body, and your elbow bent to 90°. Rotate the forearm gently outwards against a light band, then return with control. Stay inside your safe range and never force it. Use a light band and many repetitions, not heavy resistance.
As guided by your physiotherapist
Kieran Hirpara 4.0
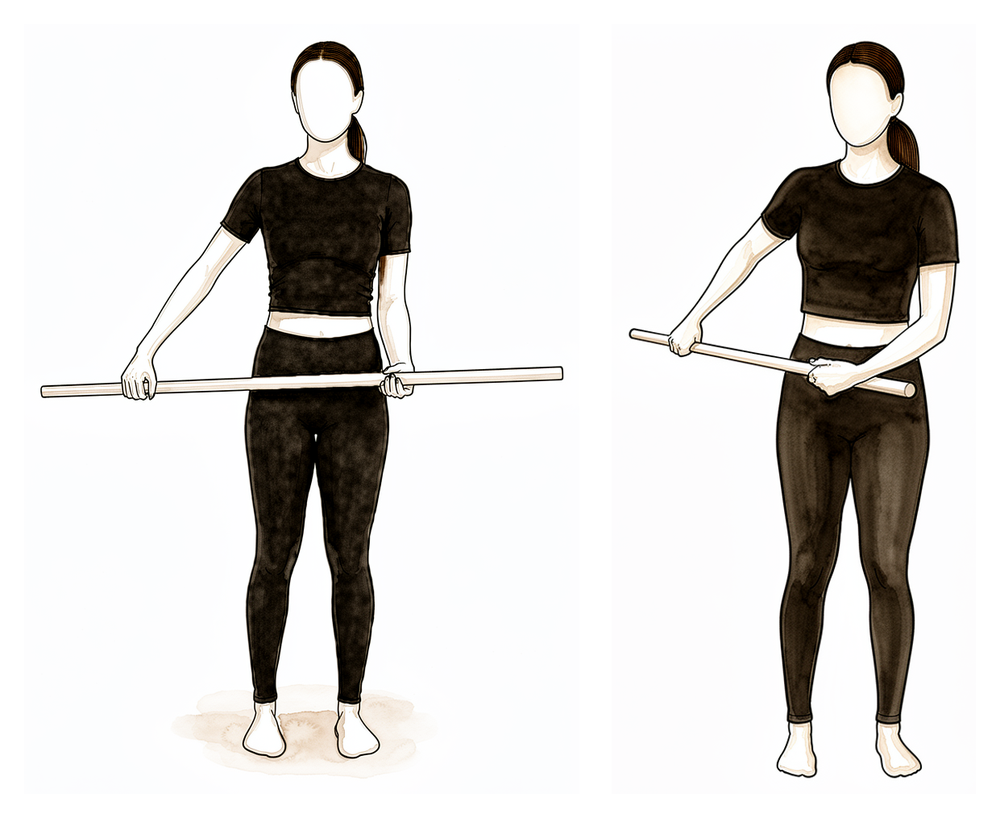
Internal rotation with a stick
From about week 6, gently and only as guided. Keep your elbow tucked at your side and use a stick in your good hand to rotate the operated forearm gently inwards across your stomach, then return. This is gentle movement only — do NOT push hard or add resistance early, as the front of your shoulder (the subscapularis muscle) is still healing.
As guided by your physiotherapist
Kieran Hirpara 4.0
Low row (shoulder-blade setting)
From about week 6. With your hand on a fixed surface beside you, press down and back to draw the shoulder blade down and in, holding briefly. This steadies the shoulder blade.
As guided by your physiotherapist
Kieran Hirpara 4.0
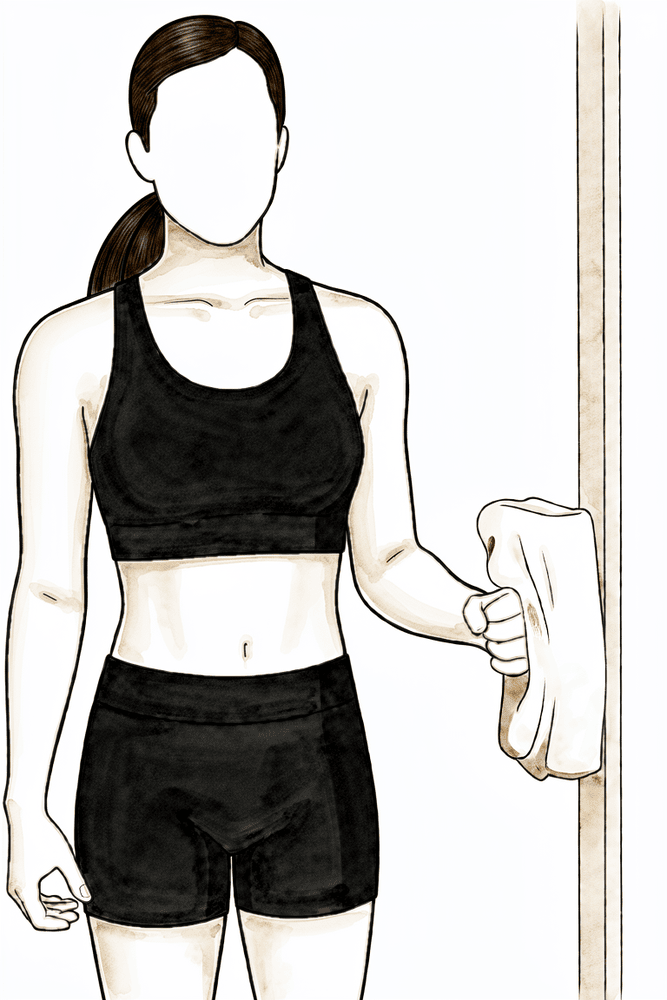
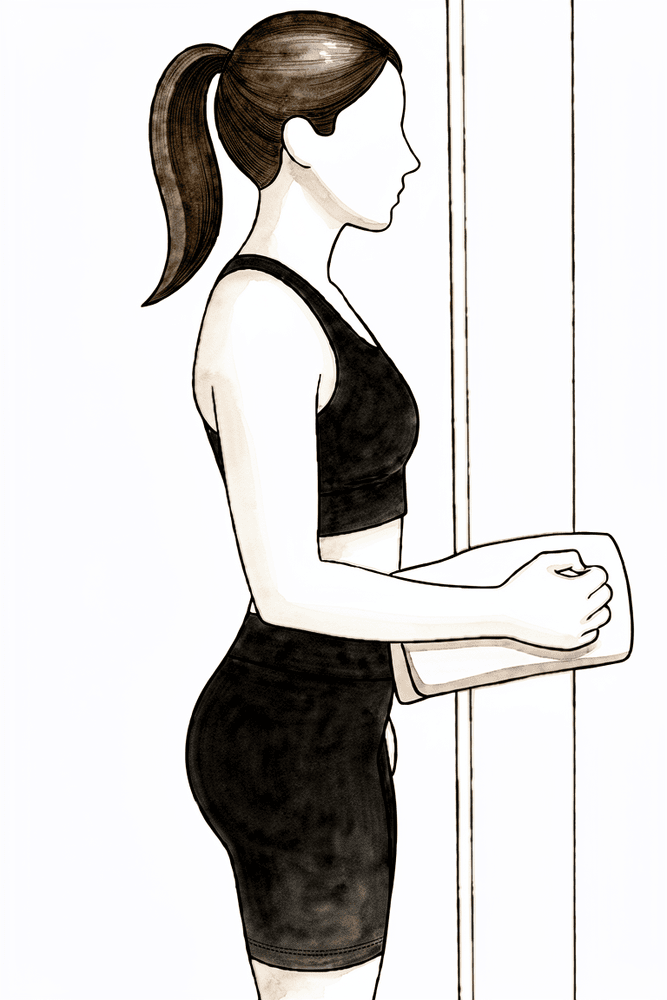
Isometric external rotation
From about week 6, if your physiotherapist agrees and only within your safe range. Stand with your elbow tucked at your side and bent to 90°, the back of your hand near a wall or door frame. Press the back of your hand gently outwards into the surface WITHOUT letting the arm move — a gentle effort, about a quarter of your strength, with no pain. Hold, then relax.
Hold ~5 seconds, gentle (~25% effort), as guided by your physiotherapist
Kieran Hirpara 4.0
Isometric internal rotation
Held back until later (usually after the graft has united and your surgeon agrees), because pressing inwards works the healing front muscle (subscapularis). When cleared, stand with your elbow tucked at your side, palm against a wall, and press the palm gently inwards WITHOUT letting the arm move — about a quarter effort, no pain. Hold, then relax.
Hold ~5 seconds, gentle (~25% effort), as guided by your physiotherapist
Kieran Hirpara 4.0
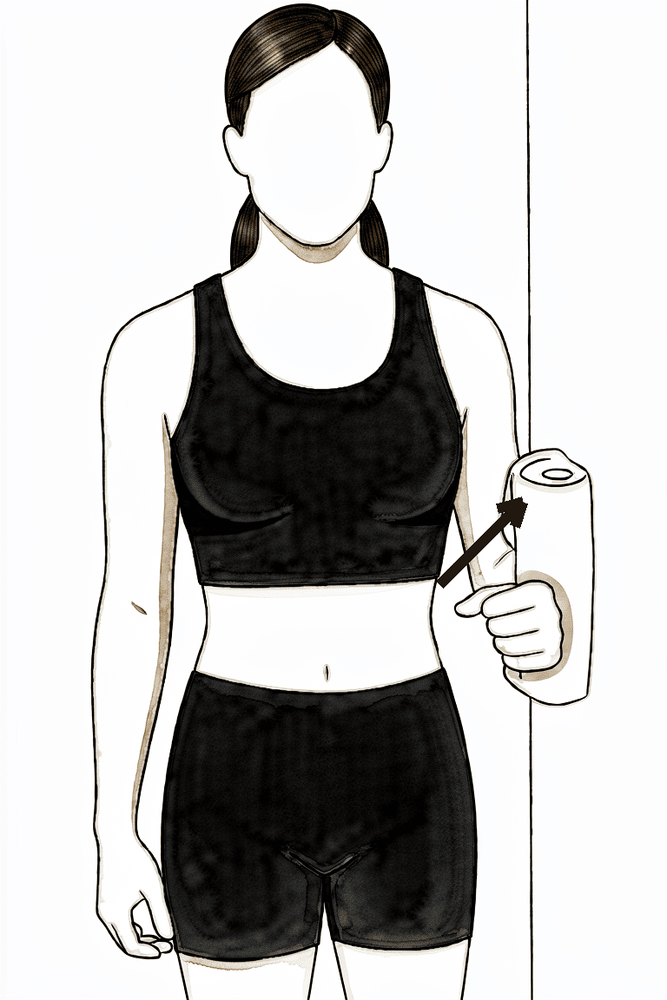
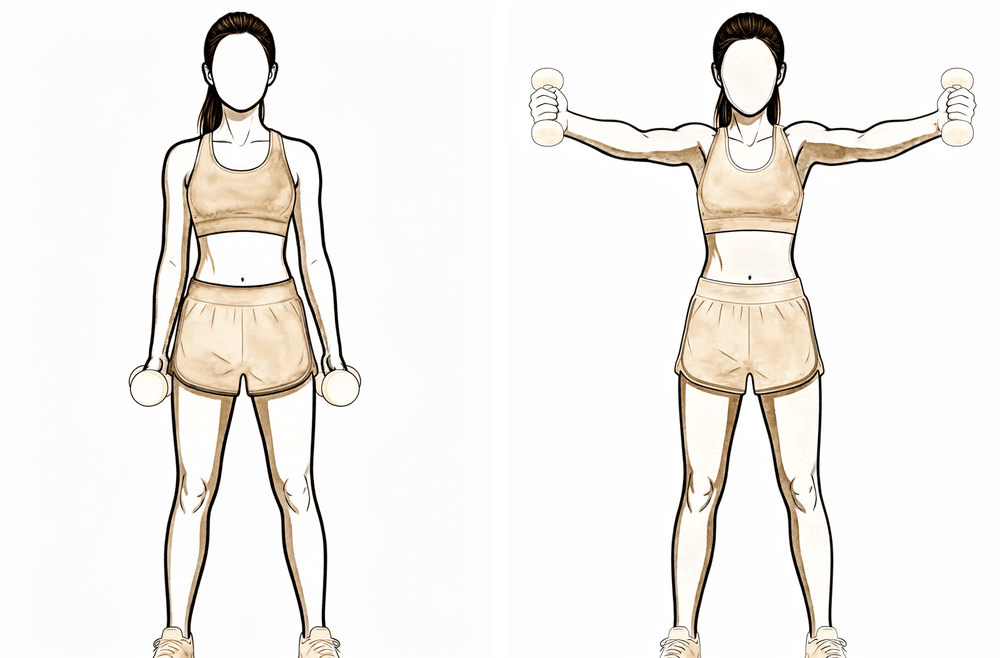
Isometric abduction
From about week 6, if your physiotherapist agrees. Stand side-on with the outside of your upper arm near a wall, elbow at your side. Press the arm gently outwards into the wall WITHOUT letting it move — about a quarter effort, no pain. Hold, then relax.
Hold ~5 seconds, gentle (~25% effort), as guided by your physiotherapist
Now the focus is movement, not strength. The sling is weaned off from about week 3. You progress from assisted movement to moving the arm under your own power, and outward rotation is gradually opened up; early on to about 45 degrees in a supported position, then further to tolerance from about week 6, always within your surgeon's limits. Light press-and-hold (isometric) drills are added, keeping inward-rotation effort gentle to protect the front muscle. Loading still waits; the bone block is only just uniting through this phase.
- Sling: weaned off from week 3.
- Movement allowed: assisted movement building to movement under your own power by about week 6 (towards roughly 90–110° of elevation). Outward rotation opened up gradually; early about 45 degrees in support, later to tolerance, within the range your surgeon sets. Inward rotation gently to about 45 degrees.
- Exercises: full-can lift to shoulder height; gentle outward-rotation band work over a towel roll; gentle inward rotation with a stick (no force); low row; gentle press-and-hold isometrics for outward rotation and abduction from about week 6 (inward-rotation isometrics held back until later). Your physiotherapist may also add gentle rhythmic stabilisation (hold-steady drills where they push lightly on your arm and you resist) to retrain control; this is hands-on work with no diagram.
Ready for the next phase when: your surgeon has confirmed (usually on review around 6–8 weeks) that the bone block has united; you can move the arm under your own power with good control; your assisted and passive movement is full or nearly full and comfortable; and gentle isometrics cause no pain flare afterwards. Strengthening does not begin until union is confirmed: this is gated by the bone healing, confirmed by your surgeon, not by the calendar.
Phase III — Strengthening (weeks 10–15)¶
Kieran Hirpara 4.0
Full-can lift with a light weight
From about week 10, once your surgeon has confirmed the bone block has united. The full-can lift as before, now building height and adding a light weight gradually. Keep the THUMB UP. Stop if the shoulder is painful or swells afterwards.
As guided by your physiotherapist
Kieran Hirpara 4.0
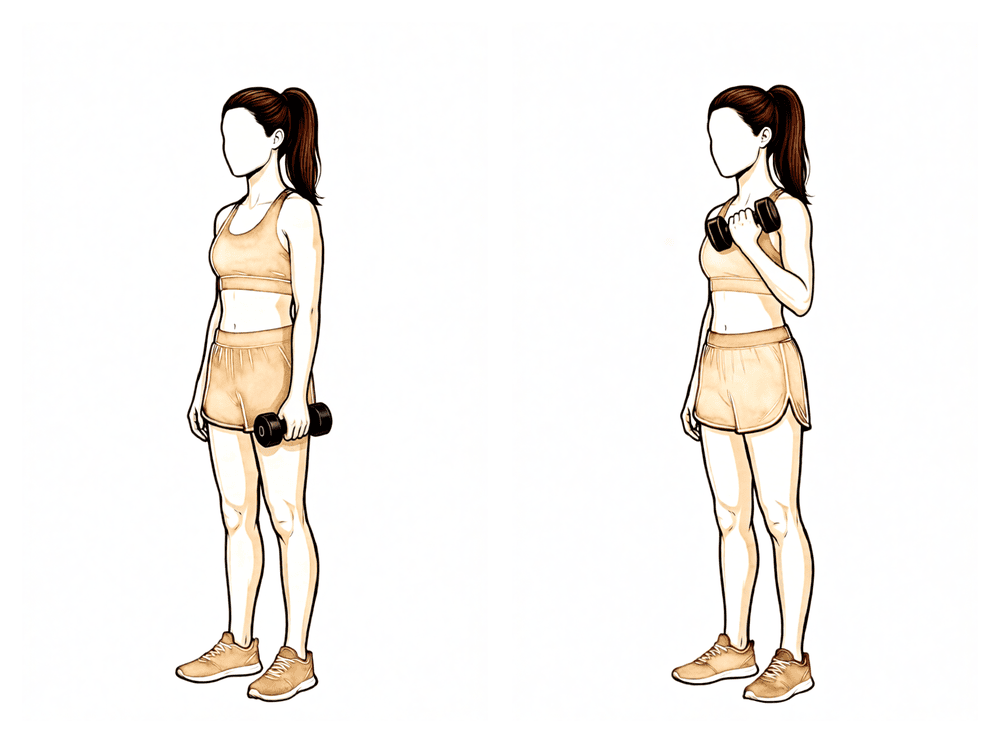
Light biceps curls
From about week 10, once union is confirmed. With your upper arm tucked at your side, bend your elbow to curl a light weight, then lower with control. Build the weight gradually. The biceps tendon attaches close to the bone block, so start light and progress slowly.
As guided by your physiotherapist
Kieran Hirpara 4.0
Internal rotation up the back, with a stick (option 1)
From about week 12, once your surgeon and physiotherapist are happy the front muscle (subscapularis) has healed. Hold a stick behind your back and use your good hand to draw the operated hand gently up your back, then lower with control. Keep it comfortable and within your physiotherapist's limits.
As guided by your physiotherapist

Kieran Hirpara 4.0
Internal rotation with a light weight, side-lying (option 2)
An alternative to the stick version, with the same timing (from about week 12, once the front muscle has healed). Lie on your operated side with the elbow tucked at your waist and bent to 90°; rotate the forearm so the hand lifts a light weight towards your tummy, then lower with control. Your physiotherapist will pick whichever version suits you — both build the same inward-rotation strength.
As guided by your physiotherapist
Kieran Hirpara 4.0
Resistance-band row
From about week 10, once union is confirmed. With a band anchored in front of you, pull the handles towards you, drawing your elbows back and squeezing your shoulder blades together, then return with control. Light band, high repetitions; stop if the shoulder becomes painful.
As guided by your physiotherapist
Kieran Hirpara 4.0
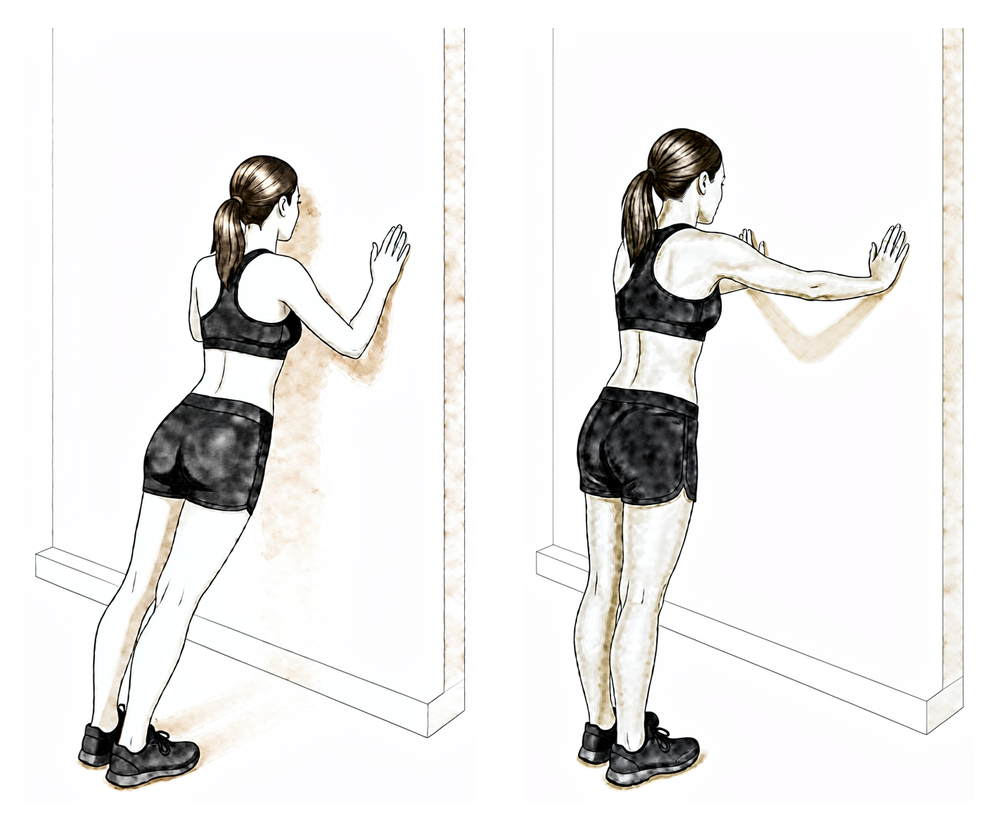
Push-up-plus (wall)
From about week 10, once union is confirmed. Start against a wall (not the floor). Do a slow push-up; at the top, push a little further so your shoulder blades spread apart and your upper back rounds slightly. Keep your elbows from going further back than your shoulders. This works the front muscle (subscapularis) — keep it light and pain-free.
As guided by your physiotherapist
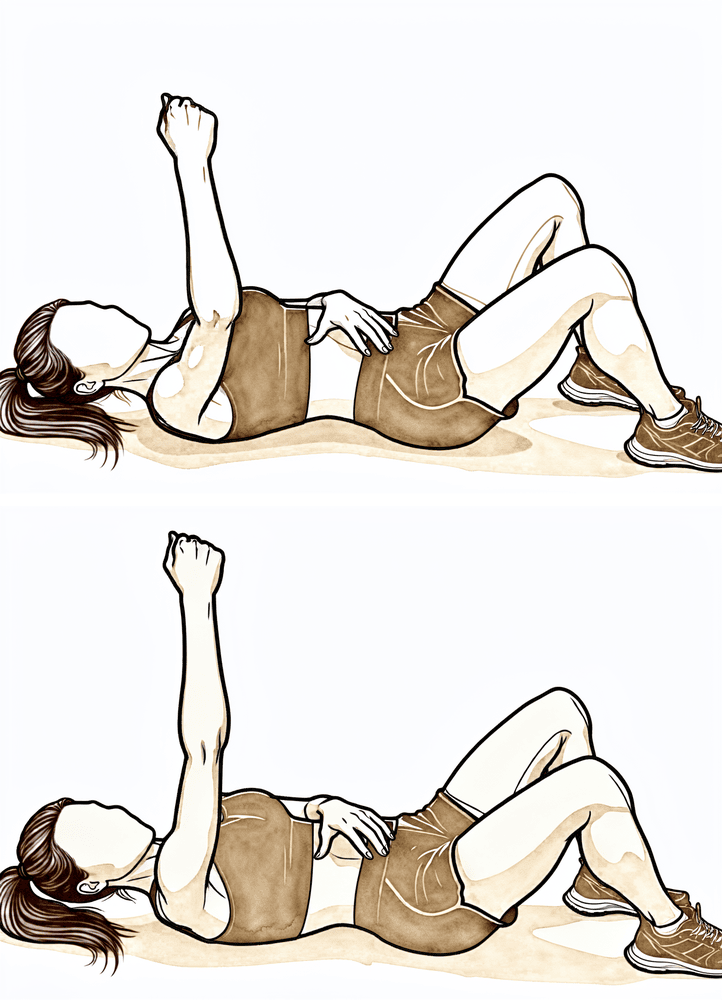
Kieran Hirpara 4.0
Forward punch (supine)
From about week 10, once union is confirmed. Lie on your back, arm pointing up towards the ceiling, holding a light weight or none. Reach the hand a little further up towards the ceiling so the shoulder blade lifts off the bed, then lower with control. A gentle subscapularis drill — keep it light.
As guided by your physiotherapist
Kieran Hirpara 4.0
Rhythmic stabilisation
With your arm supported in front of you at about shoulder height, have your physiotherapist (or your good hand) apply small, gentle pushes from different directions while you hold the arm still and steady — do not let it move. This trains the shoulder's stabilising muscles to react. Keep all the efforts gentle.
As guided by your physiotherapist
Once your surgeon has confirmed the bone has united, you can start to load the shoulder. Strengthening uses light bands and light weights to begin with: high repetitions and low loads, building gradually. The golden rule is one direction at a time: you only strengthen in a direction once you have comfortable, near-full movement in it. Inward-rotation and front-muscle (subscapularis) strengthening is still introduced carefully and later, as that muscle was repaired during your operation.
- Sling: none; near-full, comfortable movement expected before loading a direction.
- Exercises: full-can lift with a light, increasing weight; light biceps curls; resistance-band rows; wall push-up-plus and supine forward punch for the front muscle; internal rotation up the back with a stick (gentle, from about week 12 once the front muscle has healed). Build loads gradually and stop if the shoulder is painful or swells.
Ready for the next phase when: you have full, pain-free movement under your own power with good shoulder-blade control; no pain or swelling after strengthening sessions; comfortable resisted lifting below shoulder height; and your outward-rotation strength is building towards the other side.
Phase IV — Overhead and return to sport (weeks 16–20)¶
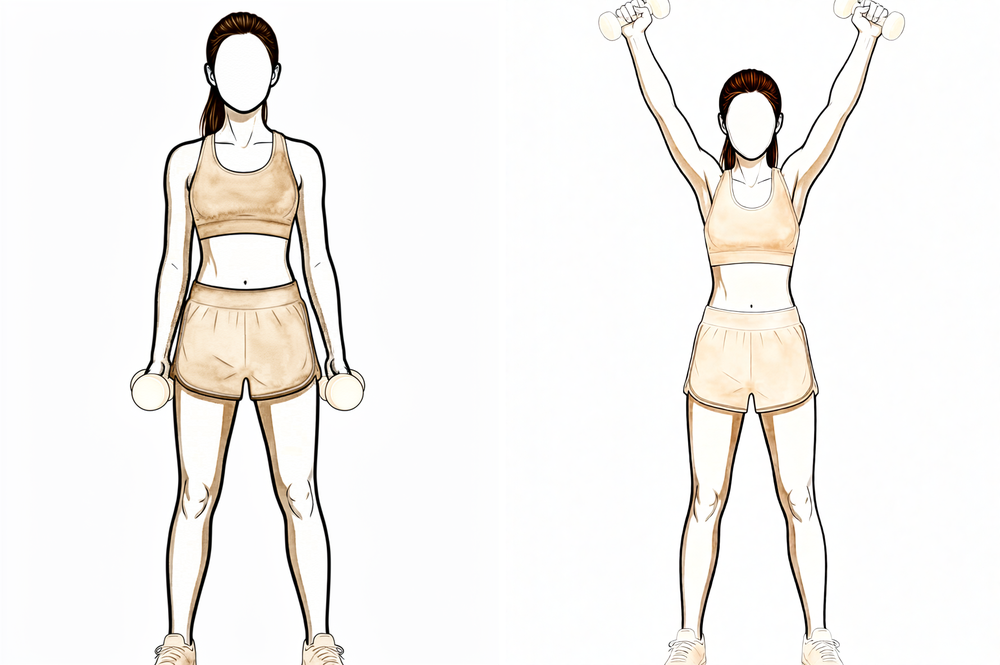
Kieran Hirpara 4.0
Overhead full-can lift
From about week 16, once your strength below shoulder height is good. Raise your arm forwards and slightly out to the side with your THUMB UP, now progressing above shoulder height, with a light, gradually increasing weight. Stop if the shoulder is painful or swells afterwards.
As guided by your physiotherapist
Kieran Hirpara 4.0
Progressive resistance-band row
Continue the band row, now building the resistance and repetitions as a base for heavier work and sport-specific conditioning. Keep good shoulder-blade control.
As guided by your physiotherapist
This phase is the bridge back to a fully working shoulder and a graduated return to sport and heavier work. You keep the range you have won and build the strength, power and endurance to use it confidently, including overhead. Returns are staged, not sudden; for sport, an interval programme that builds volume and intensity step by step is the safest route back.
- Sling: none.
- Exercises: overhead full-can lifts with a light, increasing weight once strength below shoulder height is good; progressive band rows; sport- and work-specific conditioning and, late in the phase, controlled higher-speed (plyometric) drills as appropriate. Push-ups may be added with the elbows kept from travelling far back.
Ready to return when: your outward-rotation strength is within about 8–10 degrees of the other side and your overall rotation strength is building evenly; you have full, pain-free movement with no reactive swelling under heavier load; and you pass the task-specific tests for your sport or job. Return to sport is usually around 20 weeks, and contact or collision sport is often a little later (around 5–6 months), based on meeting these criteria and on Dr Hirpara's and your physiotherapist's clearance, not the calendar alone.
Returning to sport and work¶
Your return is criteria-based: pain-free, with adequate range, strength and endurance, and signed off by both Dr Hirpara and your physiotherapist, not decided by the calendar alone. Because the Latarjet uses solid bone, recovery is generally quicker than a soft-tissue repair, but everything heavier than gentle movement waits until the bone block has united (about 6–8 weeks, confirmed by your surgeon).
- Light, chest-level activity returns from around 10–15 weeks.
- Overhead and throwing activity from around 4 months.
- Return to sport is around 20 weeks on average; full contact or collision sport is often around 5–6 months, and always once you meet the strength and movement criteria.
After your protocol¶
This protocol works alongside the practice's general recovery advice; see managing post-operative pain and wound care.
Evidence & references
Latarjet (Coracoid Transfer) for Anterior Instability with Bone Loss: Rehabilitation Evidence¶
Topic: Open Latarjet / Bristow-Latarjet coracoid transfer for anterior glenohumeral instability with glenoid bone loss (>~20% glenoid, or off-track Hill-Sachs / failed soft-tissue repair). Compiled: 2026-06-16. Sources: local RAG Orthopaedic corpus + published fellowship/PT "standard of care" protocols.
How Latarjet rehab DIFFERS from arthroscopic Bankart¶
- It is a BONY procedure (coracoid autograft screw-fixed to the antero-inferior glenoid). Fixation is rigid -> the structural construct is stronger than soft-tissue suture anchors, so AROM and return to sport are generally FASTER than Bankart (Beletsky 2020: mean RTS ~19.6 wk Latarjet vs ~32.4 wk Bankart, p<0.001).
- BUT two distinct soft-tissue structures must be protected that Bankart does not involve: (1) the subscapularis (split, or taken down and repaired, to pass the graft); (2) the coracoid graft osseous union (~6-8 weeks to unite) plus the conjoint-tendon (biceps short head + coracobrachialis) "dynamic sling" still attached to the graft.
- Graft-protection precautions: avoid aggressive shoulder extension and combined extension + external rotation stretching early (tensions the conjoint origin on the graft). Progress biceps/coracobrachialis strengthening gradually. If subscapularis was taken down & repaired, slow ER progression and avoid aggressive IR strengthening until subscap healed - get an intra-operative "safe-zone" ER from the surgeon.
- Expect a permanent mild ER deficit (Hovelius: mean loss ~7.4 deg in adduction, ~8 deg in abduction) - this is accepted, not a complication.
Consensus phased timeline (BWH Latarjet standard of care)¶
| Phase | Week window | Sling/brace | ROM allowed & restrictions | AROM / strengthening | RTS |
|---|---|---|---|---|---|
| I - Immediate post-surgical | 0-2 wk | Sling at all times (remove only to shower, arm at side); towel under elbow to prevent hyperextension (graft protection); sleep in sling | No AROM. PROM only, no forcing: flexion/elevation & scaption to tolerance; IR to 45 deg at 30 deg abd; ER 0-25 deg in scapular plane at 30-40 deg abd (open-packed); respect anterior capsule; use intra-op ER measurements | Scapular isometrics, ball squeezes; cryotherapy | None |
| II - Intermediate / ROM | 3-9 wk | Wean from sling beginning wk 3 | Early (wk 3-4): ER to 0-45 deg at 30-40 deg abd, IR 45 deg at 30 deg abd. Late (wk 6): ER to tolerance, progress to multiple abd angles once >=35 deg; IR multi-angle. AAROM from wk 3 -> AROM by ~wk 6 (good mechanics, up to 90-110 deg elevation) | Begin balanced AROM/strengthening late phase II (~wk 6): high-rep/low-load (1-3 lb), full-can scaption to 90 deg, ER/IR tubing at 0 deg abd (towel roll), prone rows, rhythmic stabilisation. Subscap-specific work (upper+lower fibres) | None |
| III - Strengthening | 10-15 wk | None | Continue A/PROM; near-full ROM before loading a plane | Biceps curls light; progressive pec major/minor (avoid anterior-capsule-stress positions); subscap strengthening (push-up plus, cross-body diagonals, IR band 0/45/90, forward punch) | Chest-level functional activities |
| IV - Overhead / return to activity | 16-20 wk | None | Full pain-free ROM | Overhead strengthening once sub-90 strength good; progressive weightlifting (15-25 reps); plyometrics/interval program if cleared; push-ups allowed but elbows not past 90 deg | Throwing/overhead not before 4 months; pre-injury sport when cleared by MD |
Active ROM start: AAROM wk 3, AROM ~wk 6. Strengthening start: scapular isometrics immediately; isotonic/RC strengthening ~wk 6. RTS: chest-level ~10-15 wk; overhead/throwing >=4 months; full/contact sport typically ~5-6 months (RAG cohorts: open Latarjet RTS averages ~6 months; bone-block soft-tissue/graft healing requires the 3-month minimum). ER milestones to advance: PE >=155 deg, ER within 8-10 deg of contralateral at 20 deg abd and >=75 deg at 90 deg abd.
Graft-protection summary (the Latarjet-specific precautions): no aggressive extension or extension+ER stretch early; protect conjoint tendon/biceps origin; protect subscapularis (slower ER + delayed IR strengthening if taken down); no pec flys/wide-grip bench/military press/behind-neck lat pulls; tricep dips avoided; osseous union ~6-8 wk gates heavier loading.
Key controversies & evidence flags¶
-
Is a sling even necessary after open Latarjet? An RCT (Kourimpetis/PMC9969622, "Is sling immobilization necessary after open Latarjet surgery...") challenges routine immobilisation - because rigid bony fixation may not need the soft-tissue protection a Bankart does. This is the leading edge of "accelerated Latarjet." Evidence: STRONG (single RCT) - emerging, not yet standard.
-
Accelerated Latarjet rehab / faster RTS. Multiple comparative studies (Beletsky 2020; Delgado 2025 matched-pair; Rogowski 2025 JSES) confirm Latarjet RTS is earlier than Bankart and that bony union (~3 months) - not soft-tissue - is the rate limiter. Rogowski (JSES 2025) argues functional dominant/non-dominant testing at 4.5 months predicts successful RTS better than time alone, supporting criteria-based acceleration. Evidence: MODERATE (good cohorts, no large RCT on the rehab pace itself).
-
Contact/collision-sport return & procedure choice. Latarjet is often preferred in collision athletes (rugby) precisely because of bone block + dynamic sling. Tanaka 2022 / Hirose 2026 (Bristow vs Latarjet in rugby) and Gowd 2021 (JSES, RTS after Latarjet) inform RTS rates and timing; subluxation/pain after RTS more frequent in some Latarjet vs Bristow series. Contact RTS still generally ~5-6 months and criteria-based. Evidence: MODERATE cohort-level.
-
Subscapularis split vs takedown-and-repair changes ER progression: takedown demands slower ER and delayed IR strengthening. Protocol explicitly defers to an intra-operative surgeon-defined ER "safe zone." Evidence: consensus / biomechanical rationale.
CITATIONS¶
Published rehabilitation protocols (URLs)¶
- Brigham & Women's Hospital, Dept. of Rehabilitation Services - Anterior Stabilization of the Shoulder: Latarjet Protocol (orig. 2009, updated May 2016): https://www.brighamandwomens.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/shoulder-latarjet.pdf
- Rehabilitation Guidelines for Latarjet/Coracoid Process Transfer (Eichinger, MD): https://www.josefeichingermd.com/pdf/rehab-guideline-for-latarjet.pdf
- Rehabilitation Protocol - Latarjet (Coracoid Transfer/Eden-Hybinette), Lindsay Sports Med (2025): https://www.lindsaysportsmed.com/pdf/laterjet-and-edenhybinette-center-2025.pdf
- Rehabilitation Protocol: Latarjet Coracoid Process Transfer (Utz, MD): https://www.christopherutzmd.com/pdfs/latarjet-protocol.pdf
- Latarjet Procedure overview - Physiopedia: https://www.physio-pedia.com/Latarjet_Procedure
Local RAG corpus (article / journal / year)¶
- Beletsky A, Cancienne JM, Manderle BJ, et al. A Comparison of Physical Therapy Protocols Between Open Latarjet Coracoid Transfer and Arthroscopic Bankart Repair. Sports Health. 2020. [protocol comparison - Latarjet RTS ~19.6 wk vs Bankart ~32.4 wk, p<0.001; AAROM ~6-8 wk]
- Matache BA, Hurley ET, Wong I, et al. Anterior Shoulder Instability Part III - Revision Surgery, Rehabilitation and Return to Play - An International Consensus Statement. Arthroscopy. 2021;38(2). (Poses the open questions on immobilisation duration after coracoid transfer vs Bankart vs glenoid bone grafting.) [consensus]
- Gowd AK, Liu JN, Polce EM, et al. Return to sport following Latarjet glenoid reconstruction for anterior shoulder instability. Journal of Shoulder and Elbow Surgery. 2021;30(11):2549-2559. [systematic review - RTS]
- Rogowski I, Nove-Josserand L, Godeneche A, et al. Are the dominant-nondominant functional differences at 4.5 months after open Latarjet better predictors for successful RTS at 1 year than operated-nonoperated differences? Journal of Shoulder and Elbow Surgery. 2025;34(10):2338-2349. (3-month delay needed for graft healing; RTS ~6 months; criteria-based prediction.) [prospective cohort]
- Delgado C, Calvo E, Valencia M, et al. Arthroscopic Bankart Repair Versus Arthroscopic Latarjet for Anterior Shoulder Instability: A Matched-Pair Long-Term Follow-up Study. Orthopaedic Journal of Sports Medicine. 2025. [matched-pair comparative]
- Tanaka M, Hanai H, Kotani Y, et al. Open Bristow Versus Open Latarjet for Anterior Shoulder Instability in Rugby Players. Orthopaedic Journal of Sports Medicine. 2022. [comparative - contact athletes]
- Hirose T, Tanaka M, Nakai H, et al. Comparing Bristow and Latarjet procedures for anterior shoulder instability in competitive rugby players. Journal of Shoulder and Elbow Surgery. 2026;35(4). [within-subject comparative]
- Bonnevialle N, Girard M, Dalmas Y, et al. Short-Term Bone Fusion With Arthroscopic Double-Button Latarjet Versus Open-Screw Latarjet. The American Journal of Sports Medicine. 2021. [fixation/union]
- Salem HS, Vasconcellos AL, Sax OC, et al. Intra-articular Versus Extra-articular Coracoid Grafts: A Systematic Review of Capsular Repair Techniques During the Latarjet Procedure. Orthopaedic Journal of Sports Medicine. 2022. (Documents post-Latarjet ER loss ~4.5-6.3 deg.) [systematic review]
Additional online RCT/evidence¶
- "Is sling immobilization necessary after open Latarjet surgery for anterior shoulder instability? A randomized controlled trial." PMC9969622: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9969622/ [STRONG - RCT challenging routine immobilisation]
- "Latarjet procedure enables 73% to return to play within 8 months depending on preoperative SIRSI and Rowe scores." PMC8298242: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8298242/ [cohort - RTS rate/timing]
Overall evidence grade for the phased protocol itself: CONSENSUS / institutional standard-of-care (Level V). The "sling necessary?" question is the only RCT-level datapoint; accelerated/criteria-based RTS rests on good comparative cohorts (Level III).