Patients › Rehabilitation
Mallet Finger
A splint-led recovery plan for mallet finger, holding the fingertip joint completely straight without interruption for about six to eight weeks so the extensor tendon can heal, while the other finger joints keep moving.

This protocol guides your recovery from a mallet finger (a drooping fingertip caused by injury to the tendon that straightens the very last joint of the finger), under the care of Dr Kieran Hirpara at Mater Private Hospital Rockhampton. Most mallet fingers are treated without an operation, using a splint that holds the fingertip straight while it heals. It begins with your home program, followed by the structured clinical protocol written for your hand therapist. Bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about the finger, the skin under the splint, or your progress, get in touch with the rooms. It is often helpful to take a photo and email it for review.
What to expect¶
A mallet finger happens when the terminal extensor tendon (the fine tendon that straightens the very last joint of the finger, the DIP nearest the nail) is torn away from the bone. It usually follows a forced bend of a straight fingertip, such as a ball or a knock "jamming" the end of the finger. Sometimes the tendon pulls off a small flake of bone with it (a bony mallet); sometimes it tears on its own (a tendinous mallet). Either way the result is the same: the fingertip droops and you cannot straighten it yourself, even though the rest of the finger works normally.
The good news is that this injury heals very reliably with splinting alone; no operation is needed for most people. The whole treatment rests on one simple principle:
- The fingertip joint must be held completely straight, without interruption, while the tendon heals. A splint keeps the last joint straight (or very slightly back) so the torn ends can knit together. This is worn full-time (day and night) for about eight weeks for a tendinous mallet or about six weeks for a bony mallet.
- The fingertip must never be allowed to bend during this period. If the tip droops even briefly (for example while changing the splint or washing), the healing breaks and the clock starts again from zero. Because of this, how carefully you keep the tip straight is the single biggest factor in how well the finger recovers.
- The other joints of the finger stay free and keep moving. The middle joint (PIP) and the knuckle (MCP) are left out of the splint and should be moved freely from the start; moving them does not disturb the healing tip.
After the full-time period, the splint is gradually weaned (first to night-time and risky-activity use only, then off) while you slowly begin to bend the tip again. It is normal to be left with a slight permanent droop of about five to ten degrees; this is expected, does not usually affect how the finger works, and most people are very satisfied with the result.
Precautions and limitations¶
- NEVER let the fingertip bend while it is in the splinting phase, not even for a second when washing or changing the splint. If it droops, the healing resets and the splinting period starts again.
- Wear the splint full-time (day and night) for the whole period your therapist sets: about 8 weeks for a tendinous mallet, about 6 weeks for a bony mallet.
- Only take the splint off to clean and dry the skin, and only if you can keep the tip dead straight the whole time (rest it flat on a table or hold it straight with your other hand).
- Keep the middle joint and knuckle moving freely from the start; only the very last joint is held still.
- Check the skin daily. Tell your hand therapist if the skin over the top of the joint goes pale, white or sore; the splint may be holding the tip too far back and need adjusting.
- Do not start bending the fingertip until your hand therapist begins the weaning phase.
For wound, swelling and skin management, see the practice's wound care guidance.
Your exercises¶

Davplast / Wikimedia Commons, CC BY-SA 4.0
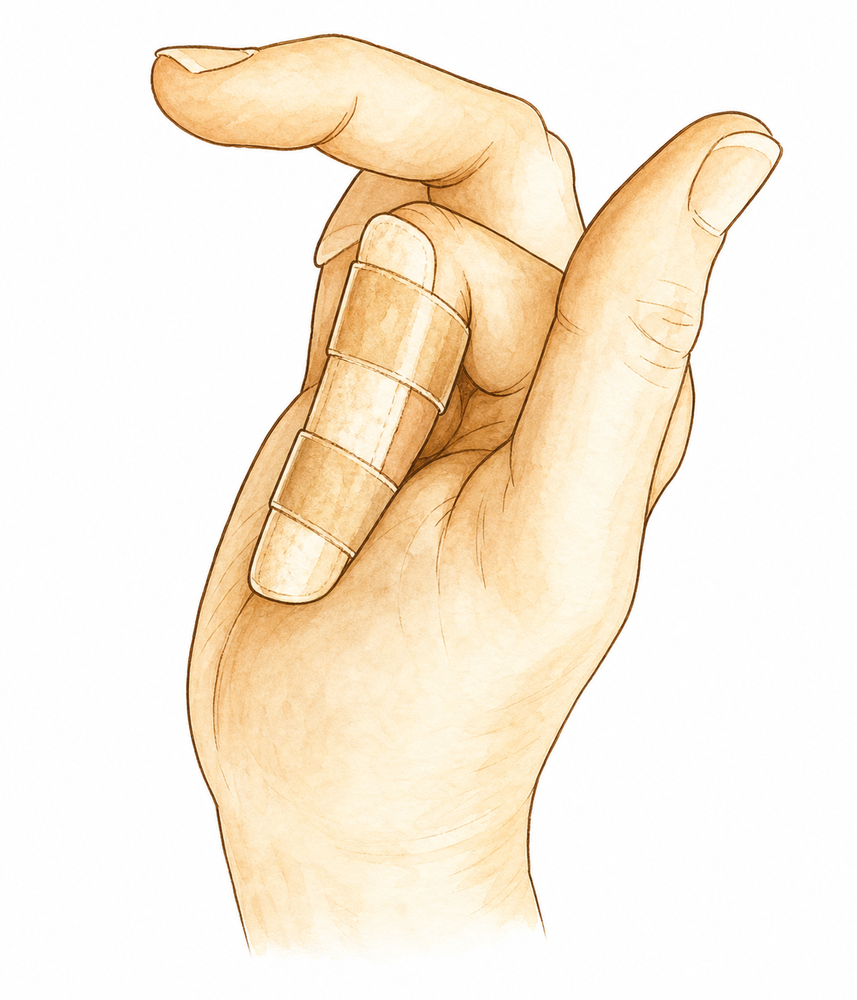
Wearing your DIP extension splint (the fingertip must never bend)
Wear your splint on the fingertip joint at ALL times — day and night — so the very last joint (the DIP, the one nearest the nail) is held completely straight. This is the single most important part of your treatment. The fingertip must NEVER be allowed to bend, even for a moment: if it droops at any time, the healing starts again from zero and the clock resets. Keep the splint on while washing, sleeping and working, and check that the tip always stays straight inside it.
Worn continuously — tendinous mallet about 8 weeks, bony mallet about 6 weeks
Kieran Hirpara 4.0
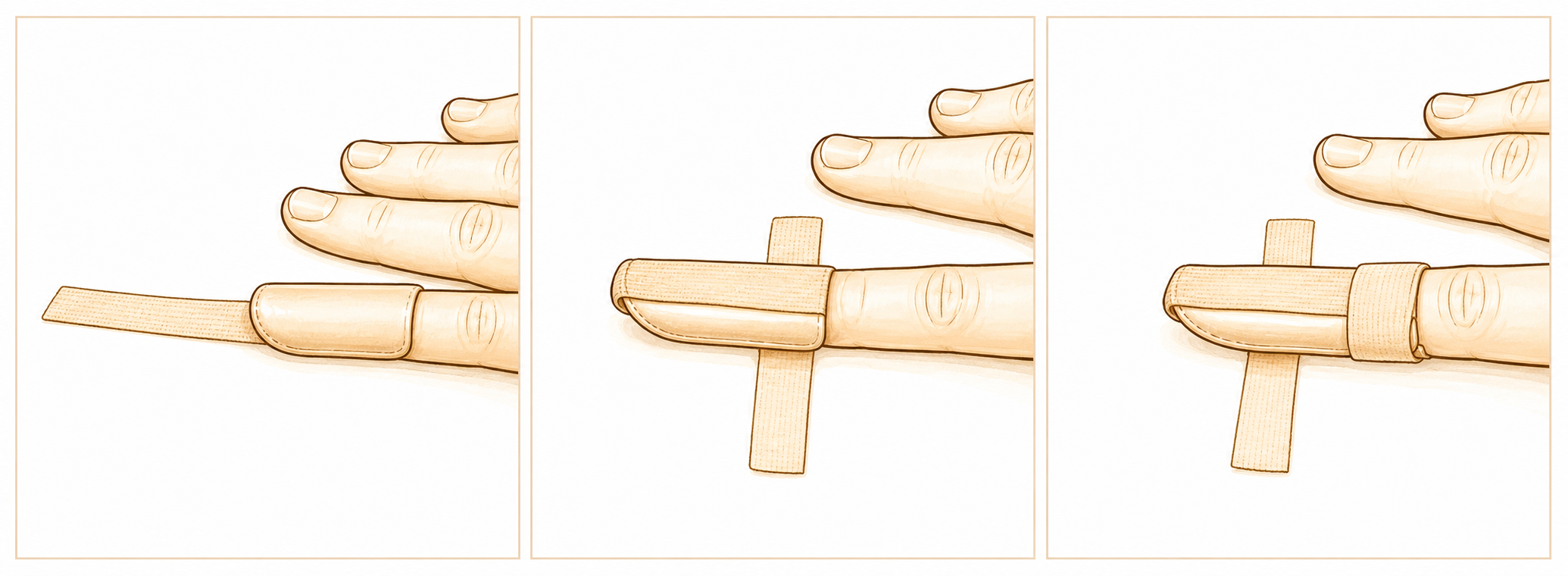
Changing the splint safely (keep the fingertip straight)
The splint only comes off to clean and dry the skin — and only if you can keep the fingertip dead straight the whole time. Rest the finger flat along the edge of a table so the tip is supported and cannot drop, or use your other hand to hold it straight. Slide the old splint off, clean and dry, then slide the new one on — all without ever letting the tip bend. If you are not confident doing this, leave it to your hand therapist.
Once a day for skin care, only with the fingertip kept fully straight
Kieran Hirpara 4.0
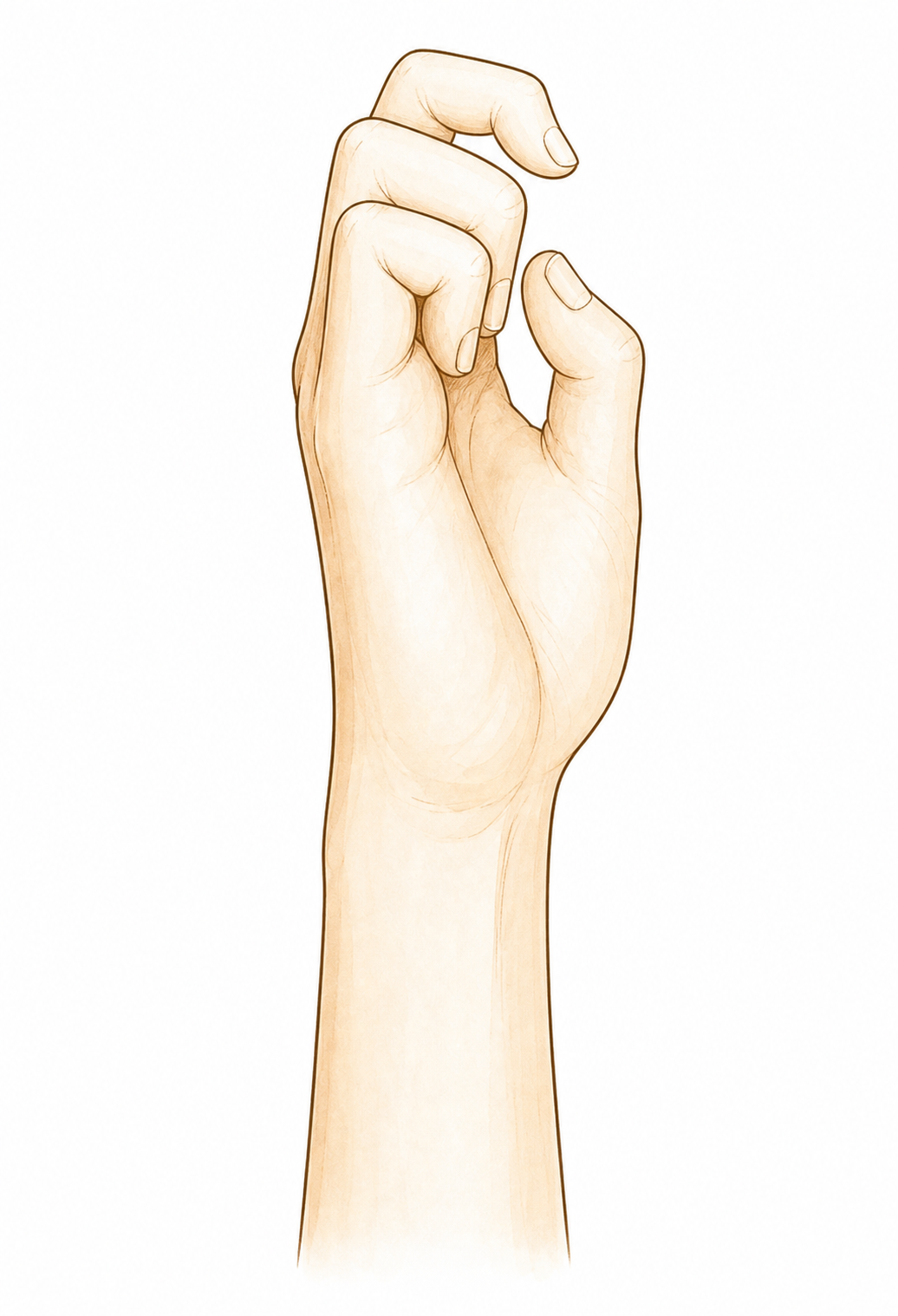
Keep the middle and knuckle joints moving (PIP and MCP)
While the fingertip is splinted straight, keep the OTHER joints of the finger moving so they do not stiffen. Bend and straighten the middle joint (the PIP) and the knuckle (the MCP) fully and freely — these joints are safe to move and moving them does not disturb the healing tendon at the tip. Make a part-fist and open out again, keeping the splinted tip straight throughout.
10 times at each joint, a few times a day, splint left on

Kieran Hirpara 4.0
Skin and swelling care under the splint
Each day, with the fingertip kept straight, check the skin — especially over the top of the joint and the nail. Some pinkness is normal, but if the skin looks pale, white or sore where the splint presses, the splint may be holding the tip too far back; tell your hand therapist so it can be adjusted. Keep the finger and splint clean and dry, and elevate the hand if it swells.
Check daily; report any pale, sore or broken skin
Kieran Hirpara 4.0
Graded fingertip bending (weaning phase)
A LATER exercise — only once your hand therapist starts weaning (commonly from about 6 to 8 weeks) and there is no, or only acceptable, droop of the tip. Out of the splint, gently bend the fingertip joint a SMALL amount, then straighten it fully again, staying well within comfort. Do not force it. If the tip starts to droop again, go back to full-time splinting and tell your therapist.
A few gentle bends, only as guided in the weaning phase
These are the exercises from your handout. The most important "exercise" of all is simply wearing your splint correctly and keeping the fingertip straight at every moment; everything else is built around that. Early on, your job is to keep the splint on, keep the skin healthy, and keep the other finger joints moving freely. The gentle fingertip-bending and blocked-straightening exercises belong to the later weaning phase and should not be started until your hand therapist specifically begins them. Stop anything that makes the fingertip droop and go back to full-time splinting.
Your clinical protocol¶
The rest of this page is the staged clinical protocol for splint-led rehabilitation of a mallet finger. This section is to be provided to the hand therapist, and each phase opens with a plain-English explanation of what is happening. Healing depends on uninterrupted DIP extension: the terminal tendon (or the avulsed bony fragment) unites only if the DIP is never allowed to flex during the splinting period, while the PIP and MCP are kept free, because their motion does not disturb terminal-tendon healing. Patient compliance is the dominant outcome driver.
Before treatment, confirm whether the mallet is tendinous or bony and review imaging. A DIP extension orthosis is used: Stack, thermoplastic, or volar/dorsal alumifoam; splint type makes no meaningful difference to outcome, so choose for fit, skin tolerance and compliance. Hold the DIP in full extension or slight hyperextension, but AVOID excessive hyperextension (dorsal-skin blanching/ulcer risk). For a bony mallet, prefer a straight/neutral DIP rather than hyperextension to avoid volar subluxation of the distal phalanx. The PIP is always left free.
Phase I — uninterrupted full-time extension splinting (weeks 0 to 6/8)¶
The fingertip joint is held continuously straight, day and night, so the tendon or bony fragment heals. The splint comes off only for skin care, and only with the DIP kept extended throughout; any single episode of DIP flexion restarts the healing clock. The PIP and MCP move freely.
For your hand therapist:
Education and precautions - Fit a DIP extension orthosis (Stack/thermoplastic/alumifoam), DIP in full extension or slight hyperextension; avoid excessive hyperextension (skin blanching/ulcer); bony mallet → straight/neutral, not hyperextended (subluxation risk) - Continuous wear: tendinous ~8 weeks, bony ~6 weeks; the DIP must never flex during this window - Teach a flat-surface splint change technique so the DIP is never allowed to drop; if the patient cannot maintain extension, the therapist performs changes - PIP and MCP left free and actively moved from day 1
Management - Skin: daily inspection over the dorsal DIP and nail fold; adjust the orthosis if blanching/pressure; keep clean and dry - Oedema: elevation; gentle proximal-joint motion - Exercises: full active PIP and MCP ROM; no DIP motion - Bony mallet: maintain radiographic surveillance during splinting (alignment/subluxation), as splinting is non-inferior to pinning for extensor lag but the fragment position must be monitored
Criteria to progress - Full-time period completed (tendinous ~8 wk / bony ~6 wk) with no DIP extensor lag beyond an acceptable amount, and healthy skin
Phase II — weaning and starting controlled DIP motion (weeks 6/8, then +2 to 6)¶
Once the full-time period is complete and there is no, or only acceptable, extensor lag, the splint is weaned to night-time and risky-activity wear while gentle controlled DIP flexion begins. Night-splinting can be framed as optional (a Level-I study found it non-essential) and is used pragmatically. If a significant lag recurs, the patient returns to full-time extension splinting.
For your hand therapist:
Assessments - DIP active extension lag (degrees) and active flexion; skin; patient confidence with the tip out of the splint
Education and precautions - Wean to night-time + high-risk-activity splinting for about 2 to 6 more weeks; night wear optional per current evidence - If extensor lag >20° recurs after splinting, resume full-time extension splinting for ~4 to 6 weeks
Management - Exercises: begin gentle, graded active DIP flexion (small range first) and blocked active DIP extension (stabilise the PIP, extend the DIP); progress flexion range as the lag allows - Reduce daytime splint wear once the DIP holds extension actively with no, or acceptable (≤10–20°), lag - Continue full PIP/MCP motion; scar/skin care as needed - Chronic or delayed-presentation mallets still respond to extension splinting; a delayed start is not a contraindication
Criteria to progress - DIP holds active extension with acceptable lag; controlled, pain-free DIP flexion regained; skin intact
Phase III — strengthening and return (from about weeks 8 to 12)¶
With the tendon healed and active motion regained, the finger is weaned fully out of the splint and graded strengthening and return to activity begin. A small permanent extensor lag (mean ~8°) is expected and compatible with an excellent functional result.
For your hand therapist:
Assessments - DIP active extension lag and flexion arc; grip; readiness for loading and sport
Education and precautions - Splint-free daily use; protective splinting for contact sport during return - Counsel that a residual ~5–10° extensor lag is normal and does not affect satisfaction
Management - Exercises: graded grip and pinch strengthening; full-finger ROM; task- and sport-specific progression - Return to sport/heavy work from ~8 to 12 weeks on a criterion basis (protective splint for contact sport) - Discharge once strength and function are adequate and the lag is stable; refer back if a marked lag persists or recurs
Getting back to work and activity¶
Light use of the splinted hand is fine from the start: the splint stays on, the fingertip stays straight, and you can use the hand for everyday tasks within that limit. A small fingertip splint is not usually a reason you cannot drive once you can grip the wheel and control the car safely, but check this with Dr Hirpara at your review. Gripping and strengthening build up from about six to eight weeks, as the splint is weaned. Return to sport and heavier manual work is usually from about eight to twelve weeks, judged on regaining controlled movement rather than the calendar alone, and a protective splint is worn for contact sport during that return. Expect a slight permanent droop of the fingertip of about five to ten degrees; this is normal, does not affect how the hand works, and most people barely notice it.
After your protocol¶
This protocol works alongside the practice's general recovery advice; see managing post-operative pain, wound care and scar management. The phased plan above reflects published guidance for mallet-finger splinting, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your fingertip progresses.
A note if your mallet finger is fixed surgically¶
Most mallet fingers never need an operation. Surgery is only considered for a bony mallet when the fracture involves a large part of the joint surface (more than about a third) or when the last joint is slipping out of place (volar subluxation). When fixation is done, it is commonly an extension-block (Ishiguro) K-wiring, sometimes with a temporary wire passed across the fingertip joint to hold it straight. That wire is usually kept in for about four to six weeks and removed at around five to six weeks, after which active fingertip movement begins and a night splint may be worn for about four more weeks. The evidence shows splinting is non-inferior to pinning for the final amount of droop, so an operation is reserved for the specific situations above rather than used routinely.
Evidence & references
Mallet Finger — Injury Outcomes & Splint-Led Rehabilitation (Terminal Extensor Tendon, DIP)¶
Topic scope: non-operative (and, where indicated, post-fixation) management of a mallet finger — disruption of the terminal extensor tendon at the distal interphalangeal (DIP) joint, either purely tendinous or with an avulsion bony fragment (bony mallet). This is a healing injury, not a reconstruction: the entire treatment is uninterrupted DIP extension splinting that holds the tendon (or fragment) in apposition while it unites, with the PIP and MCP left free.
Defining principle of the rehab here: the terminal extensor tendon heals only if the DIP is held in continuous extension and is never allowed to flex during the splinting period. Any single lapse into DIP flexion separates the healing ends and restarts the healing clock, which is why patient compliance is the dominant outcome driver. The PIP is deliberately kept mobile because proximal-joint motion does not disturb terminal-tendon healing. Splint type (Stack, thermoplastic, volar/dorsal alumifoam) does not materially change the outcome — fit, skin tolerance and compliance matter more than the device. The single branch point is the bony mallet with a large articular fragment or DIP volar subluxation, where surgical fixation is considered; even there, splinting is non-inferior to pinning for the final extensor lag, so operation is reserved rather than routine.
A. INJURY OUTCOMES (tendinous vs bony mallet; splinting vs fixation)¶
Mallet finger is one of the most reliably treated closed tendon injuries in the hand: the great majority heal well with splinting alone, and the principal debate is over the bony mallet — when, if ever, to fix it.
- Continuous extension splinting is the standard of care and works well for both tendinous and bony mallets, including chronic and delayed presentations, which still respond to splinting weeks after injury [Valdes systematic review LoE 1a; Salazar Botero review; Medscape; StatPearls]. Strong (SR + reviews).
- Splint type makes no meaningful outcome difference. A randomised comparison of splint designs found no superiority of one orthosis over another; the determinant is uninterrupted DIP extension and compliance, not the device [Pike RCT]. Strong (RCT).
- Splinting is non-inferior to extension-block pinning for the final extensor lag. A randomised trial comparing conservative extension splinting with operative extension-block K-wiring for bony mallet found no advantage to pinning in the residual lag, supporting non-operative management as the default even for many bony mallets [Thillemann RCT]. Strong (RCT).
- Surgery is reserved for the large bony fragment or subluxating DIP. Operative fixation is
considered when the fracture involves a large part of the articular surface (often cited as
~30%) or there is volar subluxation of the distal phalanx; common techniques are extension-block (Ishiguro) K-wiring with or without a trans-articular DIP pin. Single-K-wire constructs perform less well in non-compliant settings [Aksan; Salazar Botero; Medscape]. Moderate.
- Stack splints can subluxate a bony mallet. Volar-based Stack-type orthoses holding the DIP in hyperextension can displace a bony-mallet fragment / promote subluxation, which is why a straight/neutral DIP is preferred for bony mallets rather than hyperextension [Kaplan]. Moderate (mechanistic/clinical).
- The underlying mechanism is a terminal tendon avulsion at the distal phalanx. Anatomical and injury studies characterise the lesion as avulsion of the terminal extensor at its distal-phalanx insertion, and a very small amount of tendon lengthening translates into a large extensor lag — roughly 1 mm of lengthening ≈ 25° of lag — which is the biomechanical reason apposition must be maintained so strictly [Tuttle; Yeh; PMC current concepts]. Mechanistic.
B. REHABILITATION / THERAPY EVIDENCE¶
The central rehab questions are (1) how long and how strictly to splint, (2) whether the PIP should be included, and (3) whether night-time and post-splinting splinting are needed. The evidence supports uninterrupted full-time DIP extension splinting (~6–8 weeks) with the PIP free, followed by a weaning phase, and downgrades routine night-splinting to optional.
- Uninterrupted DIP extension is the active ingredient; the PIP must stay free. Splinting holds the DIP in full extension (or slight hyperextension) continuously; the PIP and MCP are mobilised from the outset because proximal-joint motion does not load the terminal tendon. Full-time wear is about 8 weeks for tendinous and 6 weeks for bony mallets [Valdes SR 1a; Salazar Botero; StatPearls; Physiopedia]. Strong (SR + guideline-level reviews).
- Compliance is the dominant outcome driver. Because any DIP flexion restarts healing, outcome tracks adherence to continuous extension more than any device choice; patient education and a safe flat-surface splint-change technique are central [Valdes SR; Cook BAHT survey of therapist practice]. Strong (mechanism + practice consensus).
- Avoid excessive hyperextension. Holding the DIP in marked hyperextension risks dorsal-skin blanching and pressure ulceration over the joint; slight hyperextension or neutral is sufficient, and bony mallets should be held straight/neutral to avoid fragment subluxation [Azad dorsal splinting outcomes; Kaplan]. Moderate.
- Night-time splinting after the full-time phase is non-essential (optional). A Level-I study found that continued night-splinting after the primary full-time period was not essential to the result, so the ~2–6 week post-splinting night/risky-activity phase is framed as optional and pragmatic rather than mandatory [Valdes SR 1a evidence base]. Moderate (Level I within SR).
- Recurrent lag responds to re-splinting. If an extensor lag (>~20°) recurs after the splinting period, a further ~4–6 weeks of full-time extension splinting is appropriate; chronic/delayed mallets likewise still respond [Salazar Botero; Medscape; StatPearls]. Moderate.
- A small residual extensor lag is the expected, satisfactory result. Most patients are left with a slight permanent lag (mean ~8°, typically 5–10°) that does not impair function or satisfaction; this should be counselled as normal rather than as failure [Salazar Botero; PMC current concepts; Physiopedia]. Moderate–strong (natural history).
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Continuous DIP extension splinting | Week 0–6/8 (bony ~6, tendinous ~8) | DIP held continuously extended; never flex the DIP | Full-time extension orthosis (Stack/thermoplastic/alumifoam); flat-surface splint changes only; PIP + MCP moved freely from day 1; daily dorsal-skin checks | No DIP loading; light splinted hand use | Any DIP flexion resets the clock; bony mallet held straight/neutral + radiographic surveillance |
| II — Weaning & controlled DIP motion | +2–6 weeks after full-time phase | Night / high-risk-activity splinting (night wear optional) | Begin gentle graded active DIP flexion + blocked active DIP extension; reduce day wear once lag ≤10–20° | Light functional load | Lag >20° recurring → re-splint full-time ~4–6 wk; chronic mallets still respond |
| III — Strengthening & return | From ~week 8–12 | None (protective splint for contact sport) | Splint-free use; graded grip/pinch strengthening; full ROM; sport-/work-specific progression | Grip/strength built up; driving once able to grip the wheel safely | Expect ~5–10° permanent lag (mean ~8°) — normal, satisfaction preserved |
(Phase windows mirror the precautions in the patient protocol; they are typical guides, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Splint type. Stack vs thermoplastic vs volar/dorsal alumifoam — randomised data show no meaningful outcome difference; the determinant is uninterrupted extension and compliance, not the device [Pike RCT]. Strong evidence of equivalence.
- Splinting vs operative fixation for bony mallet. Randomised data show extension splinting is non-inferior to extension-block pinning for the residual lag; surgery is reserved for the large articular fragment (>~30%) or volar DIP subluxation, not used routinely [Thillemann RCT; Aksan; Salazar Botero]. Strong (RCT) for non-inferiority; moderate for the fixation indications.
- Hyperextension vs neutral. Slight hyperextension aids tendinous apposition but excessive hyperextension risks dorsal-skin ischaemia/ulcer, and in bony mallets can subluxate the fragment — hence straight/neutral for bony mallets [Azad; Kaplan]. Moderate.
- Is night-splinting necessary? A Level-I study found continued night-splinting after the full-time phase non-essential; the post-splinting phase is therefore optional/pragmatic rather than mandatory [Valdes SR 1a]. Moderate.
- Residual lag as expected outcome, not failure. A small permanent lag (mean ~8°) is the norm and is compatible with full function and satisfaction; mislabelling it as failure drives unnecessary intervention [Salazar Botero; PMC current concepts]. Strong natural-history data.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (RCT / SR): uninterrupted DIP extension splinting as standard of care (6–8 wk full-time, tendinous ~8 / bony ~6); splint-type equivalence; PIP-free mobilisation; compliance as the key outcome driver; expected ~5–10° residual lag; splinting non-inferior to pinning for bony mallet (with radiographic surveillance during splinting).
- MODERATE: exact length of the weaning/night-splinting phase (night wear non-essential per a Level-I study); strengthening and return-to-sport/work timing (~8–12 weeks, criterion-based); hyperextension-vs-neutral splint positioning and the bony-mallet subluxation caveat; surgical indications (>~30% articular fragment / volar subluxation) and fixation technique.
- WEAK / CONFIRM: driving — a fingertip splint is not usually a contraindication once the wheel can be gripped safely, but this is confirmed clinically rather than evidence-defined.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- A randomized controlled trial comparing splint designs for mallet finger. J Hand Surg Am. 2010. DOI: 10.1016/j.jhsa.2010.01.005
- Conservative management of mallet finger: a systematic review (Level of Evidence 1a). J Hand Ther. 2015. DOI: 10.1016/j.jht.2015.03.001
- Mallet finger: a survey of British Association of Hand Therapists practice. Hand Therapy. 2016. DOI: 10.1177/1758998316664822
- The mallet finger injury: a review (current concepts in diagnosis and management). Arch Plast Surg. 2016. DOI: 10.5999/aps.2016.43.2.134
- Outcomes of dorsal splinting for mallet finger. Hand (N Y). 2022. DOI: 10.1177/15589447221093674
- Conservative splinting versus extension-block K-wiring for bony mallet finger: a randomized controlled trial. J Hand Surg (Eur Vol). 2020. DOI: 10.1177/1753193420917567
- Tendon avulsion fractures of the distal phalanx (terminal extensor avulsion). Clin Orthop Relat Res. 2006. DOI: 10.1097/01.blo.0000205903.51727.62
- Tendon ruptures in the hand. Hand Clin. 2012. DOI: 10.1016/j.hcl.2012.05.040
- Single K-wire fixation of bony mallet finger in non-compliant patients. Arch Orthop Trauma Surg. 2021. DOI: 10.1007/s00402-021-03793-4
- Subluxation of bony mallet fractures with Stack splint immobilisation. J Hand Surg Am. 2013. DOI: 10.1016/j.jhsa.2013.08.111
Mallet-finger management literature (URLs)¶
- Medscape — Mallet Finger Treatment & Management. https://emedicine.medscape.com/article/1242305-treatment
- StatPearls — Mallet Finger (NCBI Bookshelf). https://www.ncbi.nlm.nih.gov/books/NBK459373/
- Current concepts in the management of mallet finger (PMC; ~1 mm terminal-tendon lengthening ≈ 25° extensor lag). https://pmc.ncbi.nlm.nih.gov/articles/PMC4022957/
- Physiopedia — Mallet Finger. https://www.physio-pedia.com/Mallet_Finger