This protocol covers the rehabilitation after a Comprehensive Arthroscopic Management (CAM) procedure with Dr Kieran Hirpara at Mater Private Hospital Rockhampton, both what happens in hospital and over the weeks and months afterwards. Bring this page or its PDF to your first physiotherapy visit so your rehabilitation stays coordinated. Your rehabilitation is progressed individually by your physiotherapist through the phases below, depending on how your shoulder is moving and what was done at the time of your operation.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
The CAM procedure is a keyhole (arthroscopic) operation for a worn, arthritic shoulder. Rather than replacing the joint, it aims to clean it up and free it off so it moves and hurts less: the surgeon smooths the rough cartilage, removes loose fragments and bone spurs, releases the tight joint lining so the shoulder can rotate again, and frees the nerve at the front of the joint. The goal is to buy you good years of a more comfortable, more mobile shoulder and to put off, or avoid, a joint replacement.
That mix of work shapes how you recover. Because the surgeon has released a tight, stiff shoulder and worked hard to restore your rotation, the most important job afterwards is to keep that movement: a shoulder like this will try to stiffen up again if it is left still. But because the surgeon has also worked on the worn joint surfaces themselves, the early movement is done in a measured, graded way: you move early and often, but you ease into the stretches rather than forcing them, so the joint settles rather than flares up. Recovery is therefore led by movement, like a frozen-shoulder release, but it is gentler and more gradual.
Your exercises use three kinds of movement, and your team will mark which apply to you:
- Passive movement means the shoulder stays completely relaxed while your other arm, a stick or a pulley does the work.
- Active-assisted movement means you move the arm yourself with some help from the other arm or an object.
- Active movement means you move the arm under its own power, without help.
About your sling¶
You will usually be given a sling for comfort in the first week or two. It is there to rest the arm and protect it from being knocked while the joint settles; it does not hold a repair together. The key message is the opposite of a tendon or ligament repair: the sling is for comfort only, and the shoulder must not be left to stiffen. Come out of the sling for your exercises from day one, use the arm for light everyday tasks as comfort allows, and leave the sling off as much as you can once the early soreness eases.
If the surgeon reattached your biceps tendon as part of the operation (a biceps tenodesis), your team will ask you to avoid lifting and forceful bending of the elbow for about six weeks while that heals, and they will tell you if this applies to you.
Key points¶
- Keep it moving. Use the arm for light everyday tasks such as washing, dressing and eating from the start. Gentle, regular movement is what stops the shoulder stiffening up again.
- Work the rotation. Turning the arm outwards (external rotation) is one of the main movements this operation restores, so keep coming back to it. Regaining and keeping it is a key goal.
- Ease into stretches, do not force them. Stretch to the point of a gentle pull, not sharp pain. The joint surfaces have been worked on, so forcing hard, painful stretches can inflame the shoulder and set you back. Little and often beats long, forceful sessions.
- Control the pain so you can move. Take your pain relief before your exercises and before your physiotherapy appointments. Many people find heat before stretching and ice afterwards helpful.
- Go to physiotherapy regularly. Aim for regular sessions through the first six weeks. Bring this page to your first visit.
In hospital — your first exercises¶
Kieran Hirpara 4.0
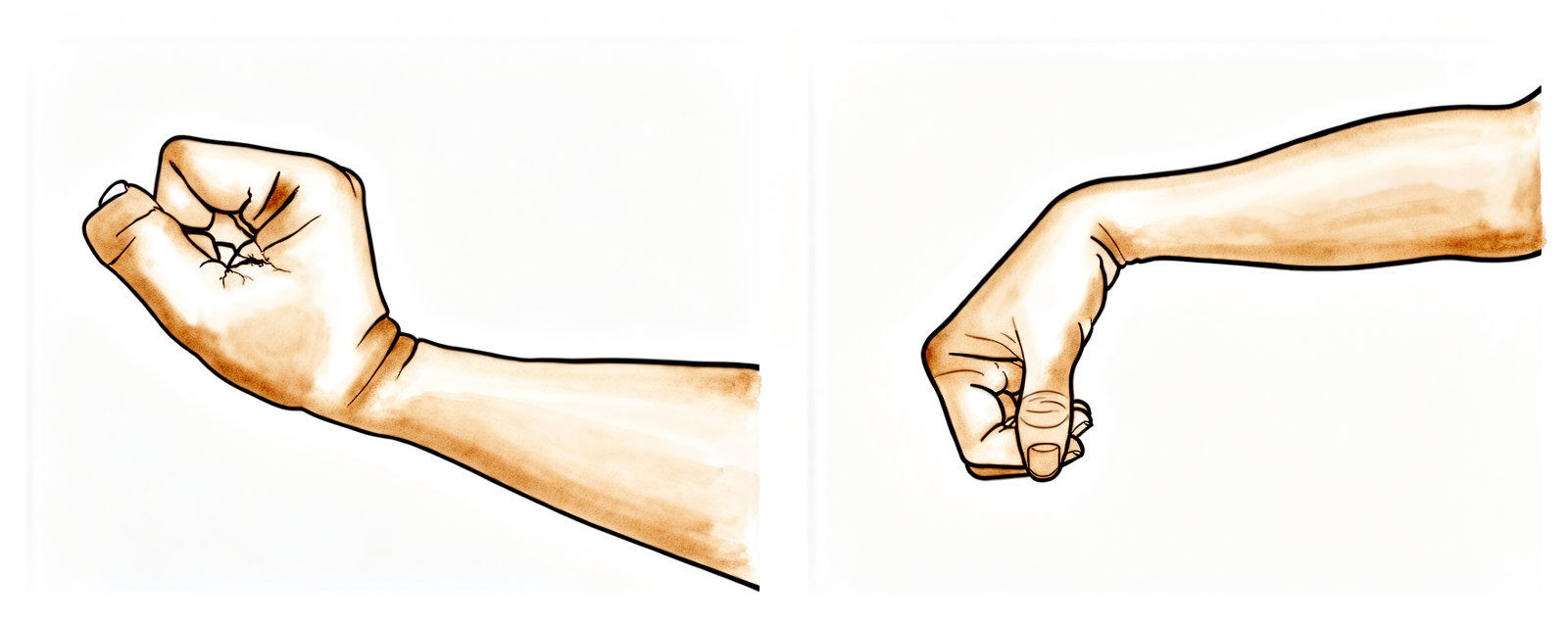
Wrist movement
Keep your hand moving by bending your wrist forwards, backwards and side to side.
10 times, 3 times per day
Kieran Hirpara 4.0
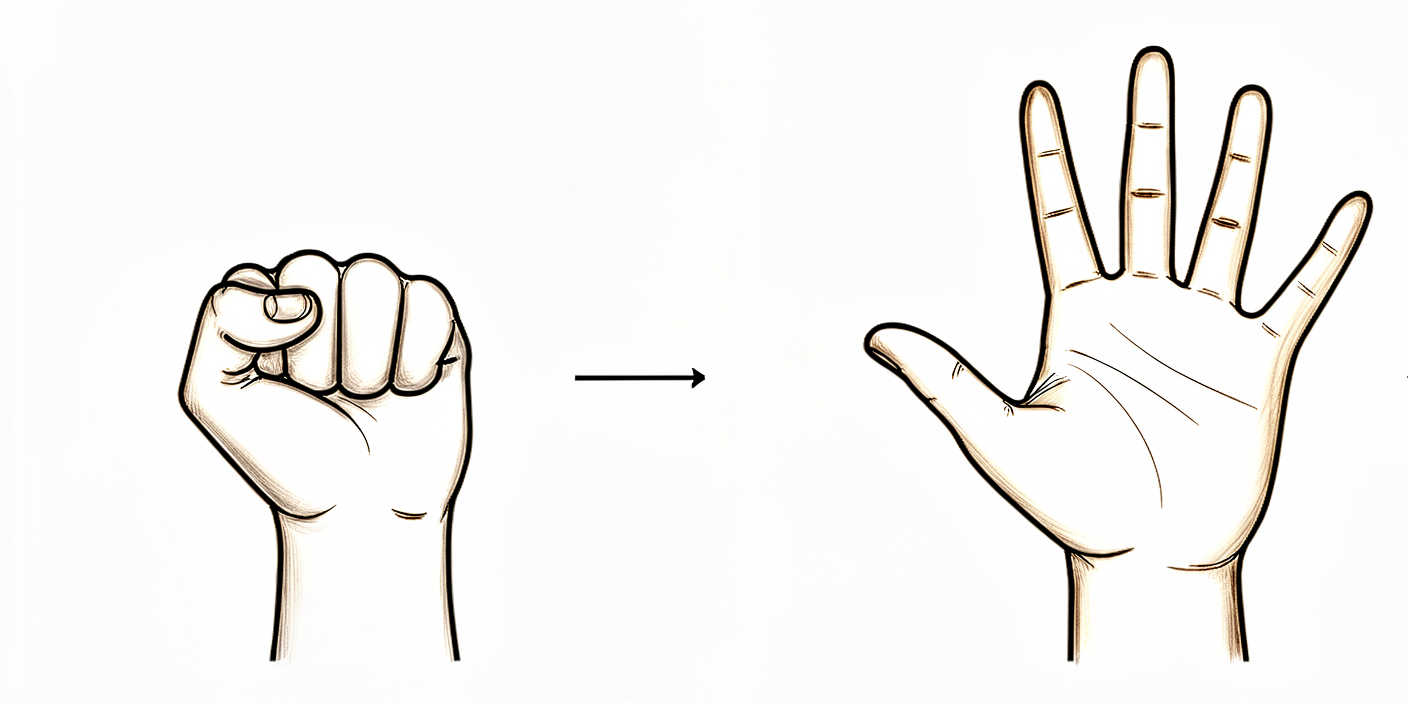
Open and close hand
Keep your hand and fingers moving by opening and closing them, or by squeezing a soft ball.
10 times, 3 times per day

Kieran Hirpara 4.0
Elbow bends
Bend and straighten your elbow. If your biceps tendon was reattached during the operation, your team will tell you to take this gently and avoid lifting with the arm for the first few weeks.
10 times, 3 times per day
Kieran Hirpara 4.0
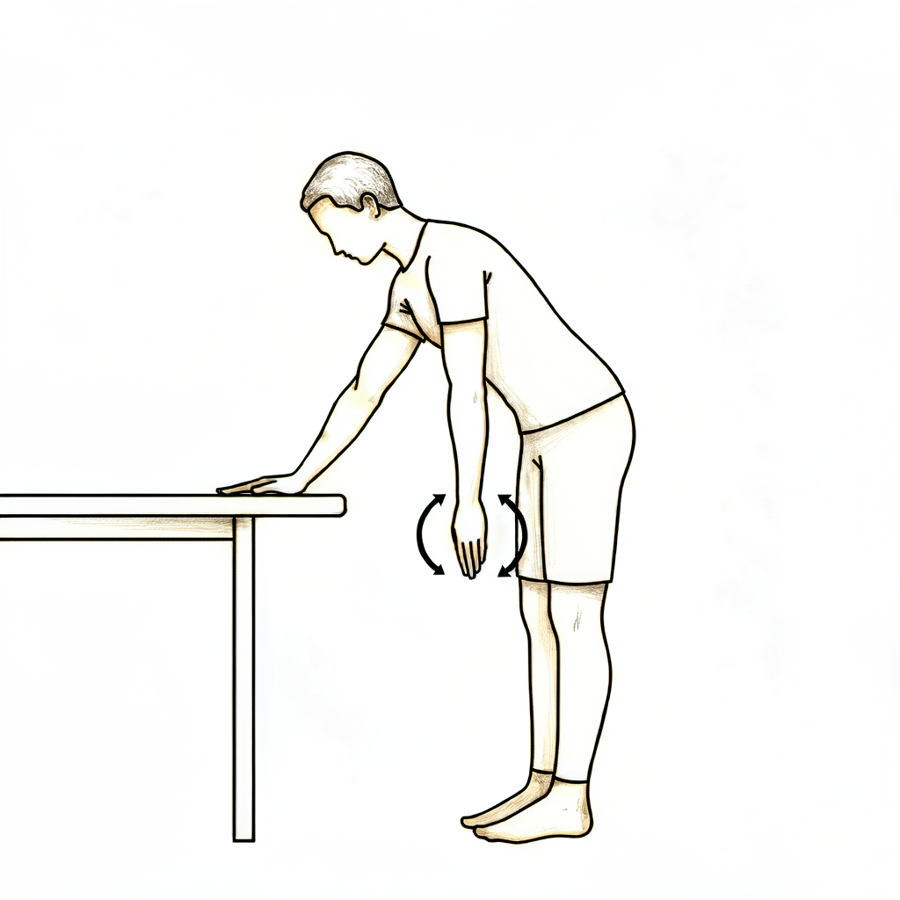
Pendulums
This is a relaxed, passive exercise. Lean forward and let your arm hang and relax down. Use your body to swing the arm gently in small circles, clockwise and anti-clockwise, and to and fro. Let the weight of the arm do the work, with the shoulder muscles relaxed.
About 30 seconds each way, 3 times per day
Kieran Hirpara 4.0
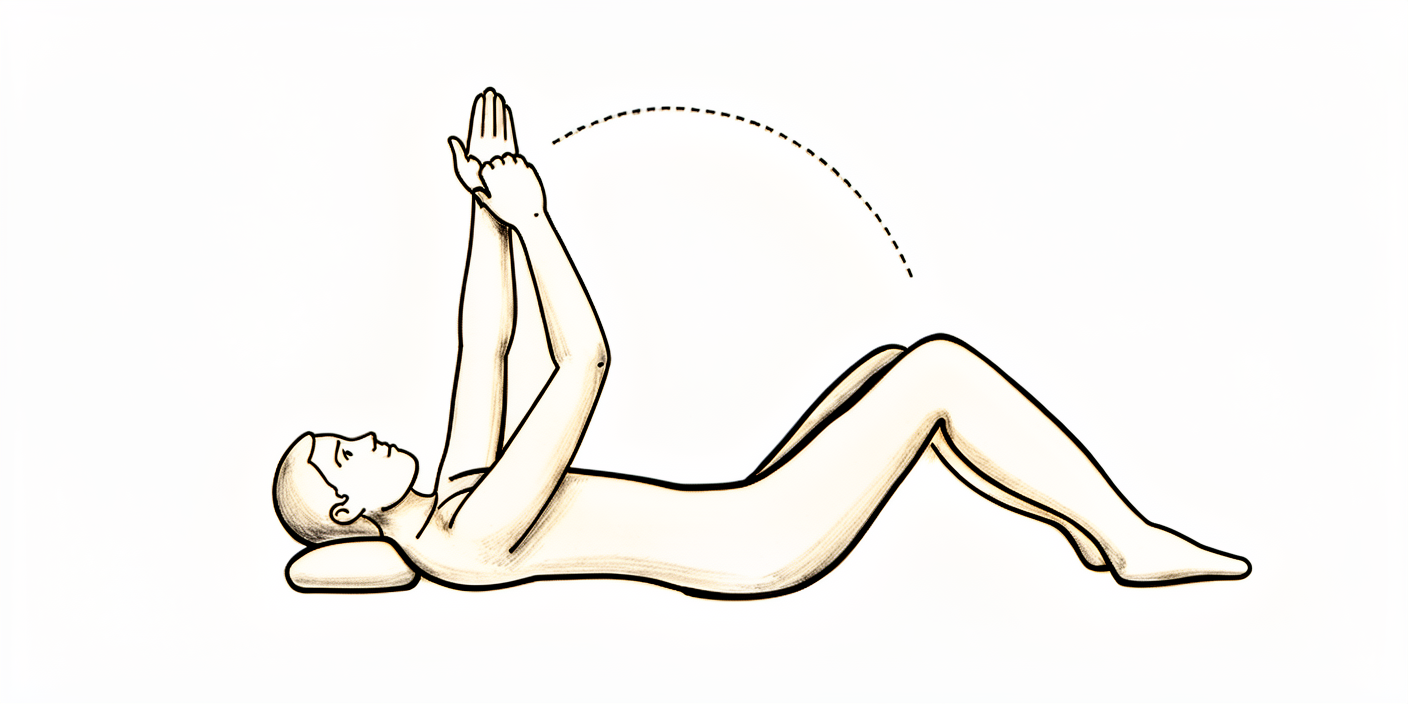
Assisted forward flexion (lying)
If you prefer, lie on your back and hold a stick (or a rolled towel) in both hands. Use your good arm to guide the operated arm up over your head, as far as it comfortably goes, then lower it slowly.
10 times, 3 times per day

Kieran Hirpara 4.0
Assisted abduction (cradle)
Cradle the operated arm in your other arm, supporting it under the elbow, and gently rock it out to the side and back, like rocking a baby. Take it to a comfortable stretch out to the side each time.
10 times, 3 times per day
Kieran Hirpara 4.0
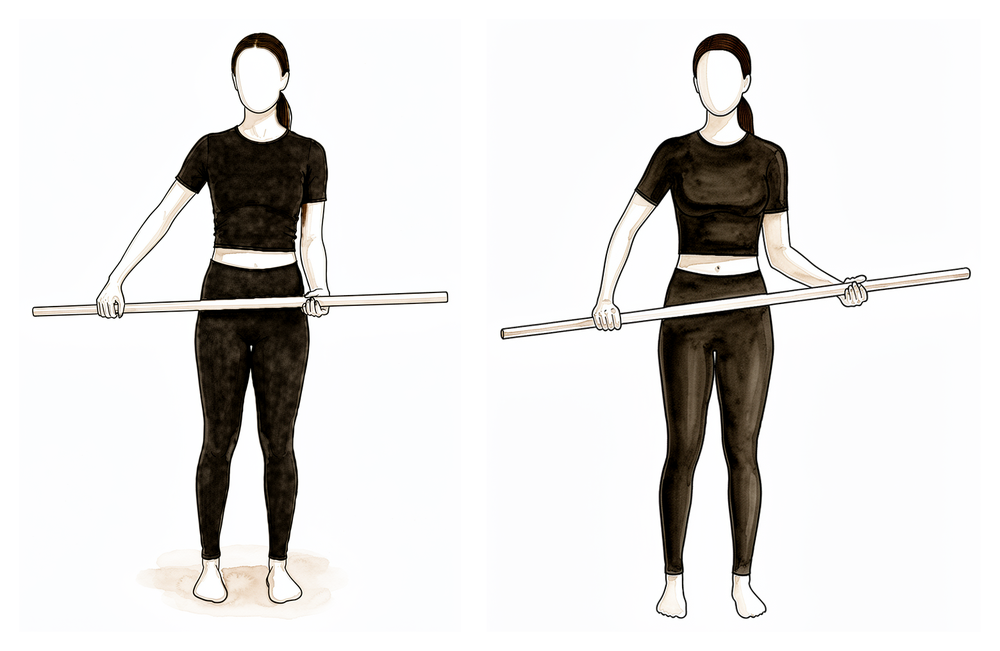
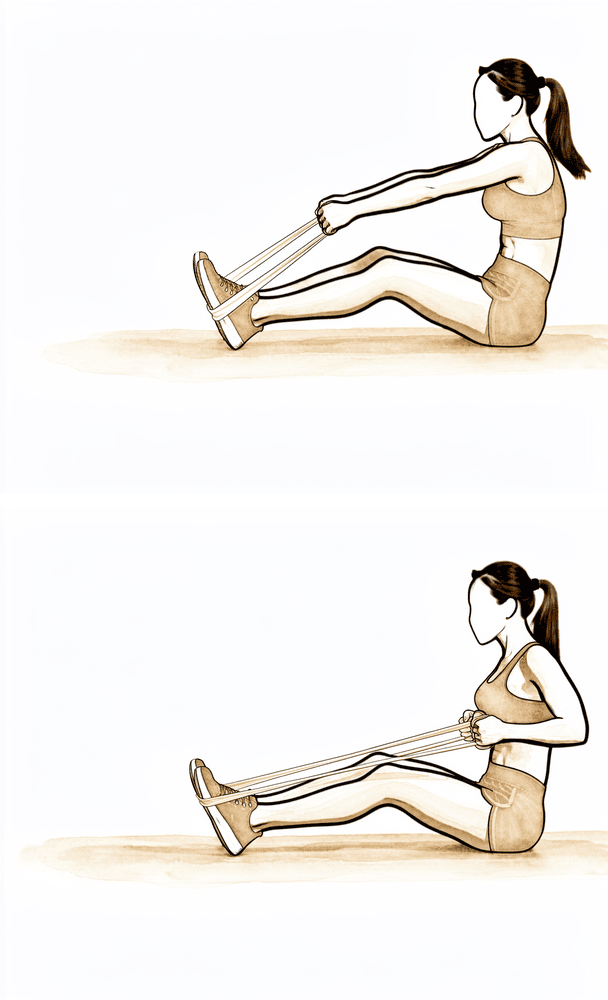
Assisted external rotation with a stick
Lie on your back with your elbow tucked by your side and bent to 90 degrees. Hold a stick in both hands and use your good arm to turn the hand of the operated arm outwards, rotating the shoulder. Rotating outwards is an important movement to regain after this operation, so keep working it gently and a little further as the weeks go on.
10 times, 3 times per day
Kieran Hirpara 4.0
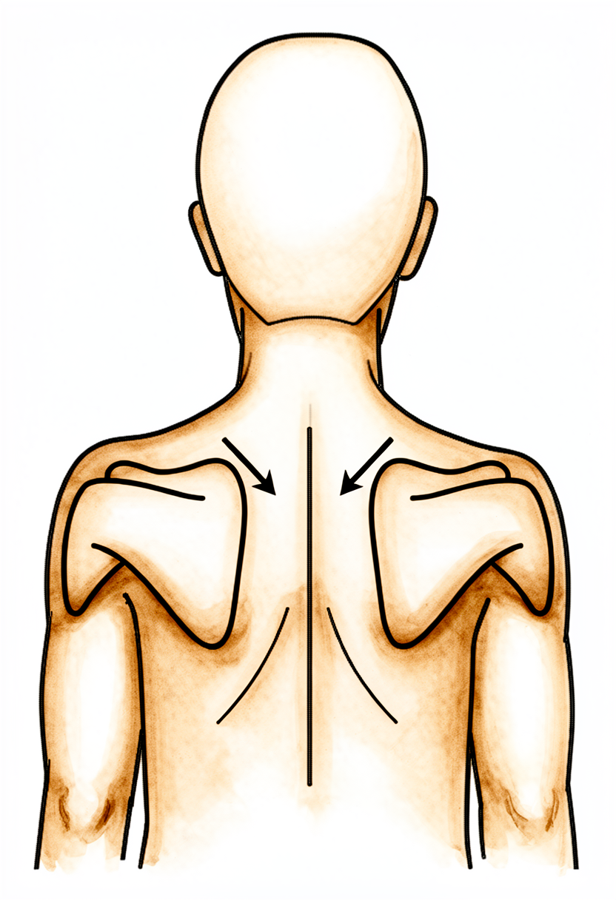
Lower trapezius setting
Squeeze your shoulder blades downwards and together, hold, then relax.
Hold 5 seconds, 5 times; repeat 3 times daily
A physiotherapist will see you in hospital and start you on the exercises below before you go home. These keep the hand, elbow and shoulder moving and begin restoring the shoulder's range straight away. Take your pain relief beforehand so you can move comfortably. Do them as marked by your team, and carry on with them at home.
Your outpatient rehabilitation¶
After a CAM procedure, rehabilitation is led by movement: the shoulder was stiff and has been freed off, so the early effort goes into keeping and rebuilding that range before it tightens again, but in a graded way that respects the joint surfaces that were worked on. Physiotherapy starts early, stays regular, and continues for some months. The phases below follow the pattern of the published rehabilitation protocol for this operation (the sources are listed at the end). The week ranges are typical rather than fixed: your physiotherapist will progress you on how your shoulder is moving, not on the calendar. Clinic review is usually arranged at about 2 weeks, 6 weeks, and 3 to 4 months.
The journey at a glance:
- Phase I — Early motion: roughly the first two weeks
- Phase II — Restoring your range: week 2 to 6
- Phase III — Strengthening: week 6 to 12
- Phase IV — Return to full activity: week 12 onwards (around three months)
Most people notice meaningful pain relief and easier movement within the first one to three months, and improvement typically continues to build over six to twelve months.
Phase I — Early motion (Week 0–2)¶
The goal of these first two weeks is to get the shoulder moving and keep the range that was freed at surgery, without stirring the joint up. You carry on the hospital exercises at home several times a day: passive and active-assisted movements, pendulums, and gentle stretches in all directions, including turning the arm outwards. Use the sling for comfort only, and take it off for your exercises and light daily tasks. Good pain control is what makes the movement possible, so keep taking your pain relief before your exercises, and use heat before and ice after if it helps. Ease into each stretch to a gentle pull, not sharp pain.
Ready for the next phase when… you are doing your home program confidently several times a day, your pain is settling, and the shoulder is moving freely into its early range.
Phase II — Restoring your range (Week 2–6)¶
Kieran Hirpara 4.0
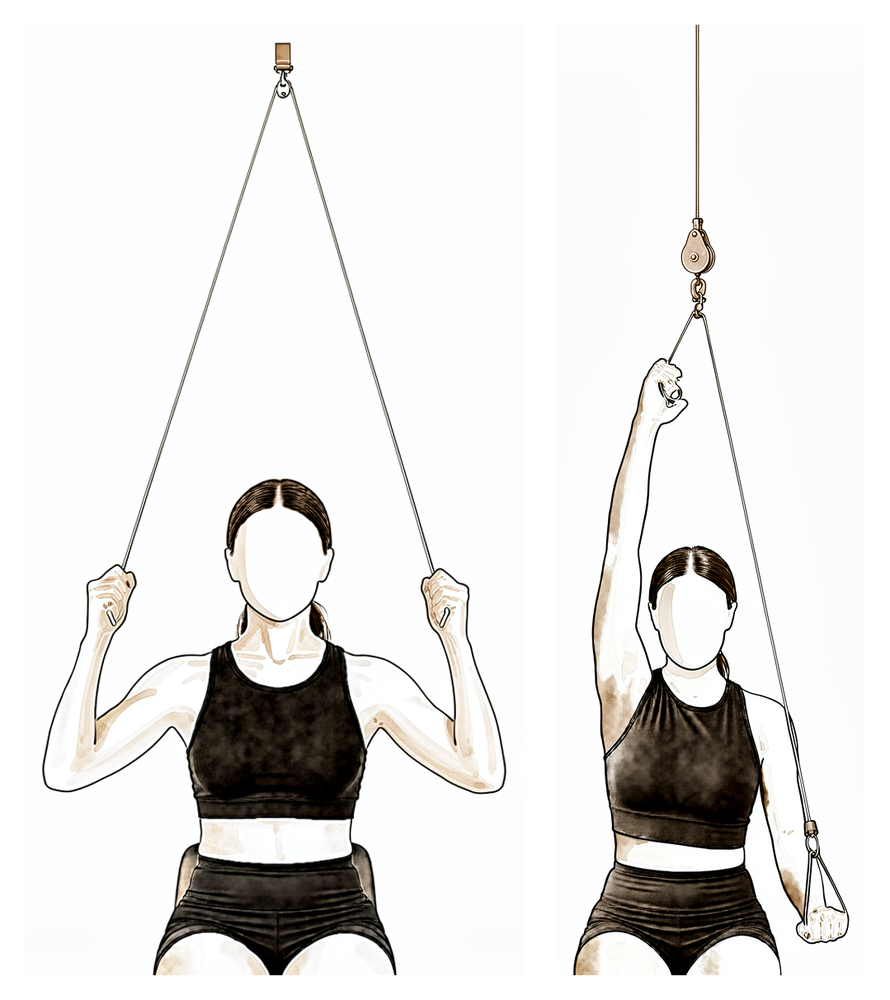
Over-door pulley
Sit under an over-door pulley with a handle in each hand. Pull down with your good arm to raise the operated arm overhead as far as it comfortably goes, then lower slowly. Work into a gentle stretch, not sharp pain.
10 times, 3 to 4 times daily
Kieran Hirpara 4.0
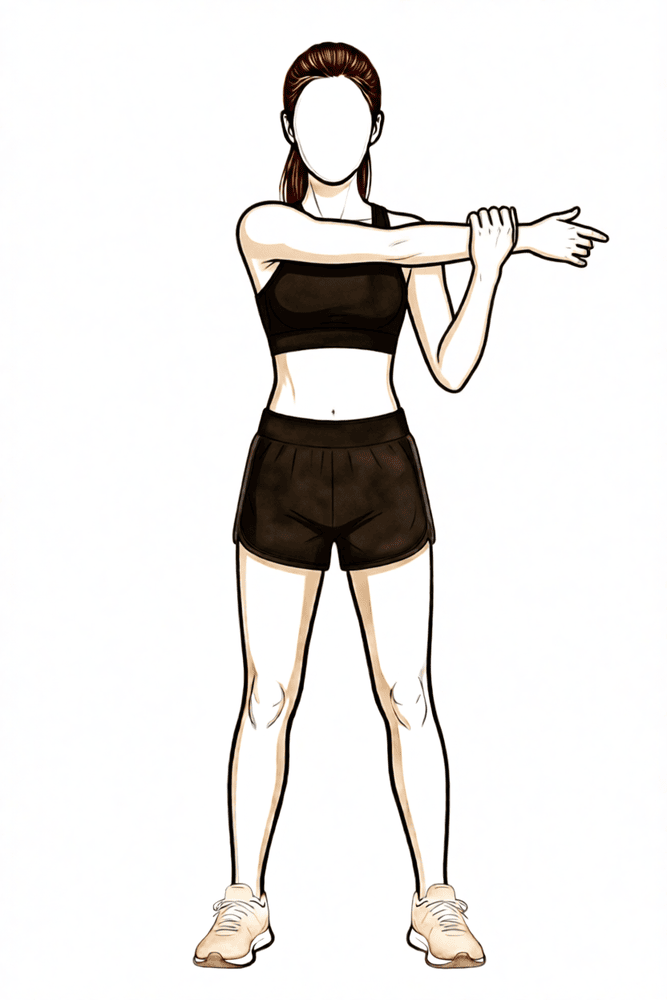
Cross-body stretch
Use your good hand to draw the operated arm across your chest until you feel a gentle stretch at the back of the shoulder, then release.
10 times, 3 to 4 times daily
Kieran Hirpara 4.0
Wand external rotation
Continue the stick-assisted external rotation from hospital, working a little further as the range frees up. With the elbow by your side, turn the forearm outwards as far as it comfortably goes, then return.
10 times, 3 to 4 times daily
Kieran Hirpara 4.0
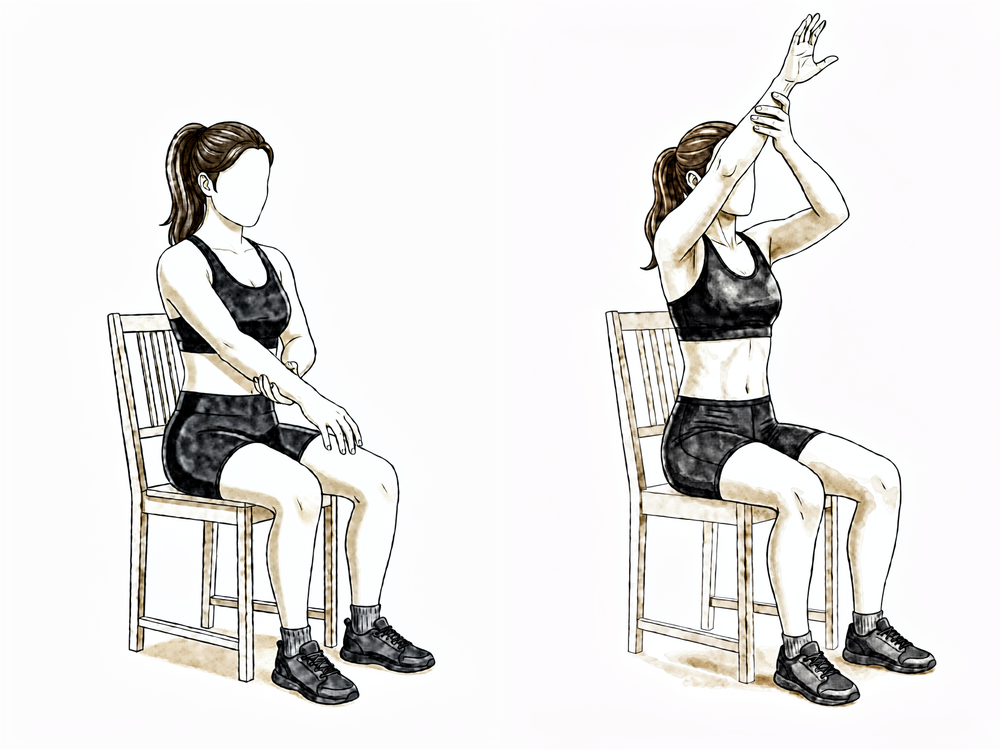
Assisted forward elevation (sitting)
Sitting and leaning forward slightly, support the operated forearm with your good hand and use it to lift the operated arm forwards and up in front of you, as far as is comfortable, then lower it slowly. Let the good arm do the work so the operated shoulder stays relaxed.
As guided by your physiotherapist
This phase keeps up the regular physiotherapy and the home program, working the range further as the shoulder allows. Your exercises progress from assisted movements towards moving the arm actively in all directions, your physiotherapist may add hands-on joint mobilisation, and you keep returning to external rotation. Stretching stays graded, firmer than week one, but still easing in rather than forcing. Most people are out of the sling and using the arm normally for light daily activities through this phase.
Ready for the next phase when… your range is steadily improving, movement below shoulder height is comfortable, and your pain has settled enough to begin gentle resistance work.
Phase III — Strengthening (Week 6–12)¶
Kieran Hirpara 4.0
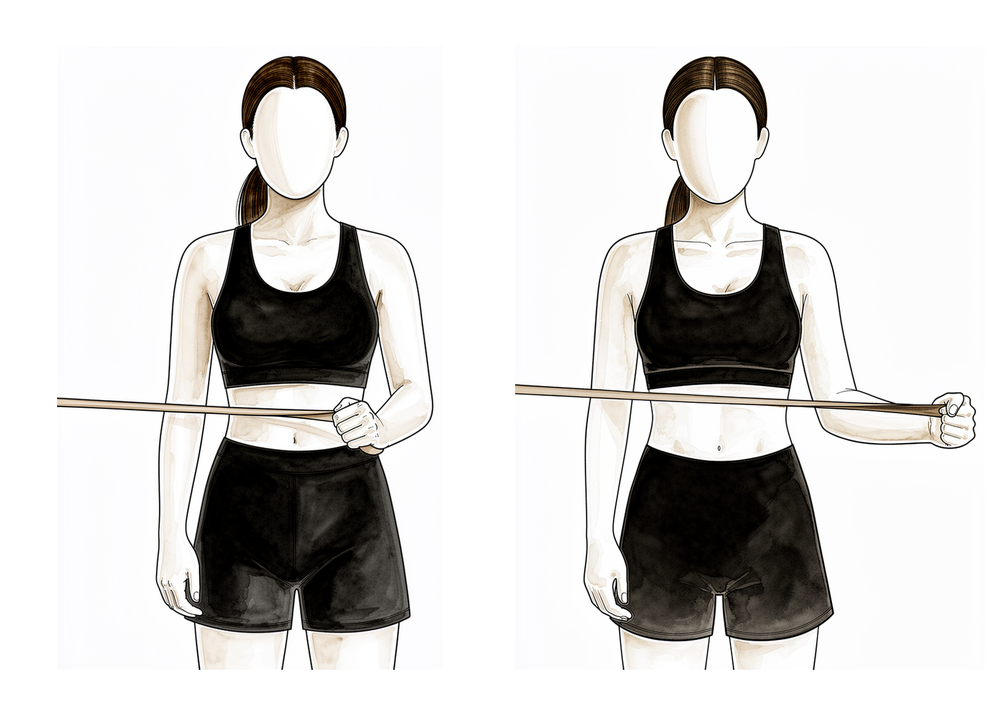
Band external rotation
Stand with your elbow tucked into your side and bent to 90 degrees, holding an elastic band anchored at waist height. Keeping the elbow at your side, rotate the forearm outwards against the band, then return slowly.
2 to 3 sets of 10 to 15, 5 days per week
Kieran Hirpara 4.0
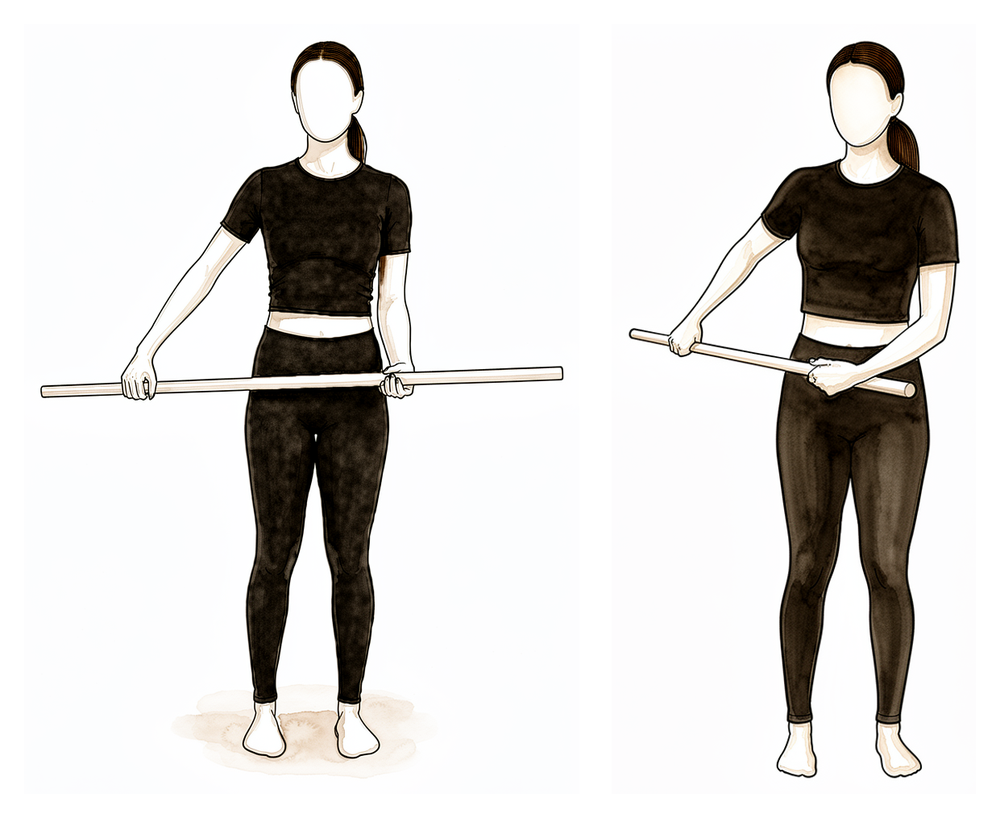
Band internal rotation
With your elbow tucked into your side, hold a band anchored to one side and rotate the forearm inwards across your body against the band, then return slowly.
2 to 3 sets of 10 to 15, 5 days per week
Kieran Hirpara 4.0
Low row
Hold a band anchored in front of you at waist height. Keeping your arm fairly straight, pull it back and down towards your hip, squeezing the shoulder blade down and back, then return slowly.
2 to 3 sets of 10 to 15, 5 days per week
Kieran Hirpara 4.0
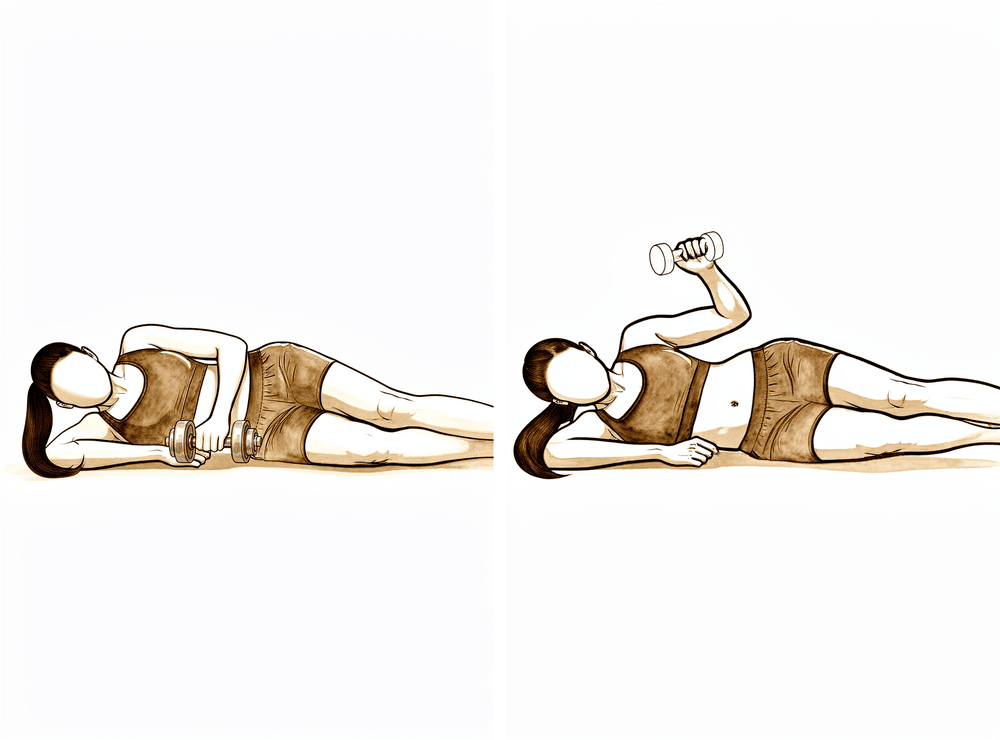
Side-lying external rotation (light weight)
Lie on your good side with the operated elbow bent to 90 degrees and tucked against your side, holding a light weight (about 0.5 to 1.5 kg). Rotate the forearm upwards, then lower slowly: the slow lowering is the important part. Keep the work below shoulder height.
2 to 3 sets of 10 to 15, low load
With your range improving, attention turns to rebuilding strength. Gentle stretching continues so you do not lose the movement you have worked for. Resistance work starts lightly at around six weeks, using elastic bands and light weights for the rotator cuff and shoulder-blade muscles, with low loads and higher repetitions. Normal daily activities should be largely back to usual, and lighter recreational activities typically resume during this phase, as guided by your physiotherapist.
Ready for the next phase when… you have full, or near-full, comfortable movement in all directions, and you can manage the strengthening exercises without a flare-up of pain.
Phase IV — Return to full activity (Week 12 onwards)¶
The final phase, from around three months, is a graduated return to heavier work, overhead tasks and sport, with more advanced strengthening. The shoulder keeps improving well beyond this point: most people continue to gain comfort and confidence over six to twelve months. Progression stays guided by how you feel: if stiffness or an ache starts to build, ease back, restore the range and settle the joint rather than pushing through.
Returning to activity¶
Most people are back to desk work and light daily activities within the first few weeks, once they are comfortable and out of the sling. Heavier, more physical work and overhead sport come back gradually over the following weeks to months, usually from around three months, as your strength returns. Driving after any shoulder operation follows the practice's standard policy rather than a fixed point in this protocol: see driving after upper-limb surgery and confirm with your surgeon at review.
Your exercises¶
After your protocol¶
The outpatient phases above are adapted from the published rehabilitation protocol for the CAM procedure, with recovery milestones drawn from the same sources. The week ranges are typical rather than fixed, and your ongoing rehabilitation is guided individually by your physiotherapist, working with the practice, based on how your shoulder recovers and exactly what was done at your operation. This page works alongside the practice's general recovery advice: see managing post-operative pain and wound care. For the operation itself and the condition it treats, see comprehensive arthroscopic management and shoulder arthritis.
Evidence & references
Comprehensive Arthroscopic Management (CAM) of Glenohumeral Osteoarthritis — Post-operative Rehabilitation¶
Topic scope: Post-operative rehabilitation after the Comprehensive Arthroscopic Management (CAM) procedure — a joint-preserving arthroscopic treatment for advanced glenohumeral osteoarthritis in young, active patients who wish to avoid or defer arthroplasty.
Defining principle of CAM rehab (a hybrid): CAM is not a repair, so — like a capsular release for frozen shoulder — there is no healing construct to protect and the priority is to keep the motion that was restored at surgery, especially external rotation freed by the capsular release and axillary nerve neurolysis. BUT, unlike a pure capsular release, CAM also resurfaces and reshapes the articular surfaces themselves (chondroplasty, microfracture, humeral osteoplasty). So the rehab is motion-led but graded: early and frequent passive/active-assisted ROM, short sling for comfort only, stretching eased to end-range rather than forced — Millett's own protocol instructs the patient to "proceed with caution while stretching to avoid joint inflammation and pain." Re-stiffening is the failure mode to prevent; joint flare from over-aggressive forcing is the one to avoid.
A. THE PROCEDURE (what is being rehabilitated)¶
CAM is a systematic, inclusive arthroscopic approach to the multiple pathologies of early-to-advanced glenohumeral OA, described by Millett and colleagues. It bundles, in one sitting, as many of the following as the joint requires [Millett 2013; Millett EATS 2015]:
- Debridement, chondroplasty, synovectomy and loose-body removal — smoothing frayed cartilage and clearing mechanical debris.
- Capsular release — to restore range, particularly external rotation, lost to the arthritic contracture.
- Inferior humeral osteoplasty — excision of the inferior humeral "goat's-beard" osteophyte that tethers the axillary nerve and blocks motion.
- Axillary nerve neurolysis — freeing the nerve adjacent to that osteophyte (a defining CAM step; note a validated CAM variant deliberately omits axillary nerve release and subacromial decompression with satisfactory durable results [Mahmoud/KSSTA 2023]).
- Subacromial decompression ± biceps tenodesis ± microfracture of focal chondral defects, where indicated.
Patient selection (drives prognosis, not the rehab itself): best results with > 2 mm of joint space and glenohumeral congruity without significant deformity; less joint space and abnormal posterior glenoid shape (Walch B2/C) predict early failure [Millett 2016 predictors]. Survivorship (freedom from arthroplasty): 76.9% at minimum 5 years, 63.2% at minimum 10 years in suitable candidates [Mitchell 2016; Spiegl/Horan 2020].
B. POST-OPERATIVE PHASED TIMELINE¶
The published protocol is a 3-phase, individually-tailored program (Millett group; mirrored in clinic patient materials). Mapped here onto the practice's standard 4-phase patient structure. Clinic follow-up at 2 weeks, 6 weeks, and 3–4 months.
| Phase | Window | Sling | ROM | Strengthening | Notes |
|---|---|---|---|---|---|
| I — Early motion | Week 0–2 | Comfort only, ~1–2 wk, off for exercise from day 0 | Passive + active-assisted ROM immediately; pendulums; gentle stretch in all planes incl. external rotation; caution — ease to end-range, do not force | Hand/elbow/scapular setting only | Goal: maintain the motion gained at surgery + prevent scar/re-contracture; pain control to permit motion |
| II — Restoring range | Week 2–6 | Off | Progress AAROM → AROM all planes; keep working external rotation; add joint mobilisation; stretching graded (firmer, still not forced) | Light scapular/cuff activation as pain allows | Most back to light daily activity/work by this window |
| III — Strengthening | Week 6–12 | Off | Maintain full/near-full ROM | Elastic-resistance + light-weight cuff & scapular strengthening from ~6 wk, low load / higher reps; continued stretching | Lighter recreation resumes |
| IV — Return to function/sport | ~3 months + | Off | Full | Advanced strengthening; graduated return to sport/heavy work | Outcomes continue to improve over 6–12 months |
Procedure-specific modifiers (surgeon-dependent): - Biceps tenodesis performed → avoid resisted elbow flexion / lifting ~6 weeks. - Microfracture of a focal chondral defect → early passive motion is beneficial for the marrow-stimulation clot (as in knee microfracture), but avoid heavy axial loading in the early weeks; favour motion over load. - Axillary nerve neurolysis performed → prioritise early external-rotation ROM to hold the gain; transient axillary nerve paraesthesia is recognised and usually settles.
Recovery milestones (from CAM outcome series, not a rehab trial): meaningful pain/function improvement within the first 1–3 months; sustained patient-reported improvement and satisfaction by 6–12 months [Outcomes/Survivorship series].
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- No rehabilitation RCT exists for CAM. The post-operative regimen is expert/consensus from the originating group (Millett), not a tested protocol. Intensity and timing are reasoned from the procedure's components, not from comparative data. Weak/consensus.
- The evidence base for the operation is itself debated. CAM outcome series are predominantly Level IV (case series from a small number of high-volume centres); systematic reviews conclude arthroscopic debridement for GHOA lacks high-quality evidence for routine use, and isolated debridement + capsular release "may not provide substantial benefit" in most patients [Kelly 2014; van der Bracht 2013 critical review]. CAM's value is strongest in carefully selected young, high-demand patients with preserved joint space.
- Motion vs protection balance. The capsular-release component argues for aggressive early motion (re-stiffening is the enemy); the cartilage/microfracture/osteoplasty components argue for graded loading (joint flare is the enemy). The published protocol resolves this as early but cautious motion — the central rehab judgement.
- CAM is a family of procedures, not one operation. Exactly which steps were done (axillary nerve release, microfracture, biceps tenodesis) legitimately shifts the rehab — hence the per-patient modifiers above. A validated variant omits axillary nerve release/SAD entirely [Mahmoud 2023].
D. EVIDENCE STRENGTH FLAGS (summary)¶
- MODERATE (large/long-term cohorts): CAM mid- and long-term survivorship + PRO improvement (Mitchell 2016 n-series, 76.9% @5 yr; Spiegl/Horan 2020, 63.2% @10 yr); preoperative predictors of failure (Morrison/Millett 2016).
- WEAK / CONSENSUS ONLY: the post-operative rehabilitation protocol itself (no defining RCT; expert protocol from the originating group); debridement-based arthroscopy for GHOA (systematic reviews: low-quality evidence, Kelly 2014; van der Bracht 2013).
- EXTRAPOLATED: early-motion rationale borrowed from arthroscopic capsular-release rehab; microfracture early-motion / load-caution rationale borrowed from marrow-stimulation cartilage literature.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles) — CAM clinical evidence base¶
- Millett PJ, Gobezie R, Boykin RE. Comprehensive Arthroscopic Management (CAM) procedure for treatment of glenohumeral osteoarthritis. Arthroscopy Techniques. 2015. (technique + post-op rehab description) DOI: 10.1016/j.eats.2015.04.003
- Millett PJ, et al. Comprehensive Arthroscopic Management (CAM) Procedure: clinical results of a joint-preserving arthroscopic treatment for young, active patients with advanced shoulder osteoarthritis. Arthroscopy. 2013. DOI: 10.1016/j.arthro.2012.10.028
- Mitchell JJ, et al. Survivorship and patient-reported outcomes after CAM of glenohumeral osteoarthritis (minimum 5 years; 76.9% survivorship). Am J Sports Med. 2016. DOI: 10.1177/0363546516656372
- Morrison/Millett, et al. CAM of glenohumeral osteoarthritis: preoperative factors predictive of treatment failure. Am J Sports Med. 2016. DOI: 10.1177/0363546516668823
- Survivorship and PROs after CAM, minimum 10-year follow-up (63.2% survivorship). Am J Sports Med. 2020. DOI: 10.1177/0363546520962756 / OJSM 2021. DOI: 10.1177/2325967121s00213
- Comprehensive arthroscopic management without axillary nerve release or subacromial decompression — satisfactory durable results in young patients. Knee Surg Sports Traumatol Arthrosc. 2023. DOI: 10.1007/s00167-023-07377-0
- Arthroscopic Management of Glenohumeral Arthritis: a joint-preservation approach. JAAOS. 2018. DOI: 10.5435/jaaos-d-17-00214
- Outcomes and survivorship after arthroscopic treatment of glenohumeral arthritis: a systematic review (ROM + PRO improvement, minimal complications). Arthroscopy. 2020. DOI: 10.1016/j.arthro.2020.02.036
- Kelly EW, et al. Arthroscopic debridement and capsular release for the treatment of shoulder osteoarthritis (may not justify routine use). Arthroscopy. 2014. DOI: 10.1016/j.arthro.2014.08.025
- van der Bracht H, et al. What is the role of arthroscopic debridement for glenohumeral arthritis? A critical examination of the literature (lacks high-quality evidence). Arthroscopy. 2013. DOI: 10.1016/j.arthro.2013.02.022
- CAM vs total shoulder arthroplasty and hemiarthroplasty in patients < 50 years. EFORT Open Reviews. 2026. DOI: 10.1530/eor-2023-0156
Published rehab protocol (URLs)¶
- Dr Peter Millett — Comprehensive Arthroscopic Management of Glenohumeral Osteoarthritis (procedure + components incl. inferior humeral osteoplasty, axillary nerve neurolysis, biceps tenodesis, microfracture): https://drmillett.com/wp-content/uploads/2017/02/comprehensive-arthroscopic-management-glenohumeral-osteoarthritis.pdf
- The Upper Limb Clinic — Comprehensive Arthroscopic Management (3-phase rehab description: sling few weeks; Phase 1 passive/active-assisted ROM + cautious stretching; Phase 2 strengthening ~6 wk; Phase 3 advanced/return-to-sport ~3 mo; follow-up 2 wk / 6 wk / 3–4 mo): https://theupperlimbclinic.co.uk/comprehensive-arthroscopic-management-a-joint-preserving-solution-for-shoulder-arthritis/
- Millett PJ, et al. CAM clinical results (open journal record): https://www.arthroscopyjournal.org/article/S0749-8063(12)01801-4/fulltext
- CAM (EATS technique record, PubMed): https://pubmed.ncbi.nlm.nih.gov/26697301/
Note on the rehab evidence: there is no CAM-specific rehabilitation trial in the corpus or the literature. The phased protocol above is the originating group's expert protocol (Millett, mirrored in clinic patient materials), with the early-motion and load-caution rationale extrapolated from arthroscopic-capsular-release and cartilage marrow-stimulation rehab respectively. Treat phase timings as typical, surgeon-adjustable defaults — not as trial-derived prescriptions.