How Tendons Work and Heal PDF In-depth PDF¶
Tendons are the body's cables — tough cords that connect muscle to bone and transmit the pull of the muscle into movement. When you bend a finger or lift your arm, it is tendons doing the work of carrying that force across the joint. Tendons are strong, but they heal slowly and in a particular way, and — importantly — not all tendons heal the same way. A cut flexor tendon in the finger and a torn rotator cuff tendon in the shoulder follow quite different healing stories, which is why their surgery and rehabilitation are so different. This page explains, in plain language, what tendons are and how they mend — and then, for the curious, goes deeper into the biology, including why a flexor-tendon repair gets weaker before it gets stronger, and why a rotator cuff heals onto bone the way it does.
What a tendon is and what it does¶
A tendon is a rope made mostly of collagen — the same tough protein that gives bone its flexibility — packed into tightly-aligned bundles that run along the line of pull. One end blends into muscle; the other anchors into bone. Its job is simple but vital: to transmit the force a muscle generates to the bone, so the joint moves. Some tendons also have to glide — the flexor tendons that bend your fingers slide back and forth through narrow tunnels every time you make a fist.
Tendons are living tissue, but only just: they have relatively few cells and a sparse blood supply compared with muscle or skin. That is a large part of why they heal slowly.
How tendons heal¶
When a tendon is cut or torn, it heals in three overlapping phases, much like other tissues:
- Inflammation (first week). A clot forms and repair cells move in. At this stage the join is held together mostly by the surgeon's stitches — the tendon itself is contributing very little strength.
- Repair (weeks). Cells lay down new collagen across the gap, but it is disorganised and weak at first — like a hastily-tied bundle of threads rather than a neat rope.
- Remodelling (months). With time and gentle use, that disorganised collagen is gradually replaced and re-aligned along the line of pull, and the tendon regains strength. This continues for many months — often up to a year or more.
A key point: tendon heals largely by forming scar, not by perfectly re-growing the original tissue. The repaired stretch is never quite as pristine as the original — which is why careful rehabilitation, and patience, matter so much.
What helps a tendon heal¶
- The right amount of movement. Tendons respond to load. Controlled, graded exercise (guided by a hand or physiotherapist) tells the healing collagen how to organise itself. Too much, too soon, ruptures the repair; too little leads to stiffness and a tendon stuck down by scar.
- Protecting the repair early. A fresh tendon repair is fragile for weeks even when it feels fine — following your splint and activity limits is what stops it pulling apart.
- Good general health. Not smoking, controlling diabetes, and avoiding unnecessary steroids all help; smoking in particular impairs tendon healing.
- Time. Tendon is slow tissue. Real strength takes months, not weeks.
Advanced reading: the deeper science (optional)
This section steps up to a more detailed, student-level explanation of the biology. It isn't needed to understand a tendon injury or its treatment — but if you're curious about how tendons actually work, and why a finger tendon and a shoulder tendon heal so differently, read on.
Tendon as living tissue¶
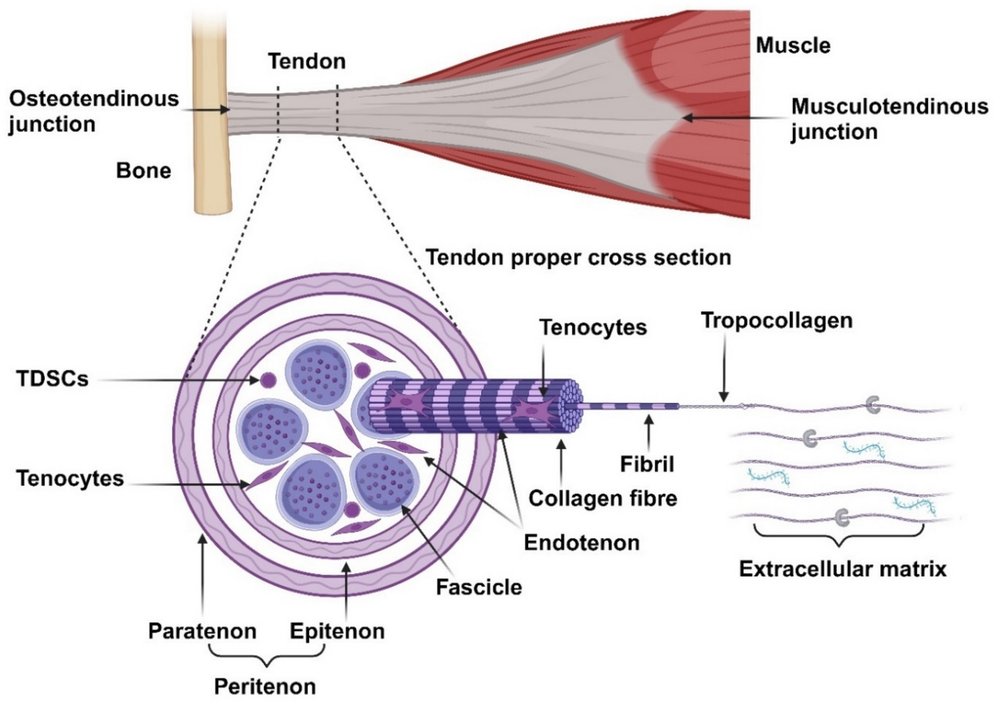
A tendon is built as a hierarchy of collagen, like a rope made of ever-smaller strands. Collagen molecules bundle into fibrils, fibrils into fibres, fibres into fascicles, and fascicles into the whole tendon — and at each level a thin connective-tissue wrapping (the endotenon, and the epitenon around the whole tendon) carries the small blood vessels and nerves. The collagen is mostly type I, exceptionally strong in tension and laid down almost perfectly parallel to the direction of pull.
At rest the fibres have a wavy, crimped pattern. When you first load a tendon this crimp straightens out, which is why a tendon is slightly stretchy at the very start of a pull before becoming stiff and strong — it has a little built-in give. Tendon is also viscoelastic: it behaves differently depending on how fast it is loaded (stiffer when loaded quickly), and it slowly creeps — lengthens — under a sustained load.
The living cells are tenocytes, sparse spindle-shaped cells strung between the collagen bundles. They maintain and very slowly renew the matrix. Because cells and blood vessels are relatively few — and some regions of certain tendons are genuinely hypovascular ("watershed" zones with a poor blood supply) — tendon healing is slow, and those poorly-supplied zones are exactly where some tendons tend to tear and to heal badly.
How tendons heal — and why it's mostly by scar¶
The three phases above, in more detail: an inflammatory phase (roughly the first week) clears debris and recruits cells; a proliferative phase (about one to three weeks) in which cells churn out large amounts of disorganised type III collagen — quick to lay down but mechanically weak; and a long remodelling phase (months, up to about 18 months) in which that type III collagen is gradually replaced by strong, aligned type I collagen, cross-linked and oriented along the line of load.
The crucial concept is that this is repair by scar, not regeneration. The body patches the gap rather than recreating the original, beautifully-ordered tendon — and what turns that early weak scar into something strong and aligned is mechanical load. That is the whole rationale behind modern tendon rehabilitation: controlled force, applied at the right time, literally instructs the scar how to become tendon.
Flexor tendon healing: intrinsic vs extrinsic, and the work of flexion¶
The flexor tendons that bend your fingers are a special case, because they have to glide through a tight tunnel (the flexor sheath, with its pulleys) to work. That creates a tension at the heart of flexor surgery, and two different ways the tendon can heal:
- Intrinsic healing comes from the tendon's own cells, nourished by the synovial fluid inside the sheath and by tiny blood-vessel folds called the vincula. The flexor tendon is largely fed not by blood vessels but by that synovial fluid, which is actively pumped into the tendon — a process called imbibition — each time the finger bends and straightens; so movement itself feeds the healing tendon. Intrinsic healing knits the tendon back together without sticking it to its surroundings — so it can still glide.
- Extrinsic healing comes from cells and scar invading from outside, from the sheath and surrounding tissue. It heals the tendon too — but it glues it to its tunnel, forming adhesions that stop it gliding, so the finger won't fully bend or straighten.
Modern repair plus early controlled movement is designed to tip the balance toward intrinsic healing and away from adhesions.
This is where the work of flexion comes in — the force the muscle has to generate to actually flex the finger. It is not just the weight being moved; it is the resistance to the tendon gliding: friction in the sheath, the bulk of the repair itself, post-operative swelling, and tight pulleys all add to it. If the work of flexion (the resistance) climbs higher than the repair can withstand, the repair gaps or ruptures — or the finger simply won't move and adhesions set in. So the surgeon is balancing two competing demands: a repair strong enough to tolerate early movement, yet slim and smooth enough to glide with a low work of flexion. Early motion only works if both are achieved.
Why a flexor repair gets weaker before it gets stronger¶
Here is the counter-intuitive part that explains the whole, cautious rehabilitation timeline. A tendon repair does not steadily get stronger from day one. It follows a U-shaped curve:
- In the first days, essentially all the strength comes from the suture — the tendon tissue itself adds almost nothing.
- Over the first one to three weeks, the cut tendon ends actually soften: the body resorbs and remodels the collagen right at the repair site before the new collagen has matured. So the whole construct reaches its weakest point in the early weeks — often around the end of the first week through the third — even though the wound looks healed and the finger feels fine.
- Then strength climbs. As disorganised type III collagen is replaced by aligned, cross-linked type I, the repair regains and then exceeds its starting strength, reaching enough for most everyday activity by around 12 weeks and continuing to mature for many months.
That dip is why hand therapy is so carefully staged, and why "it feels fine at three weeks" is a trap: that is often precisely when the repair is most vulnerable. Gentle, controlled motion in the early phase keeps the tendon gliding (favouring intrinsic healing) and aligns the new collagen — without overloading a repair that is, biologically, at its weakest. Tendon ruptures after repair cluster in these vulnerable early weeks for exactly this reason.
Tendon-to-bone healing: the rotator cuff and the enthesis¶
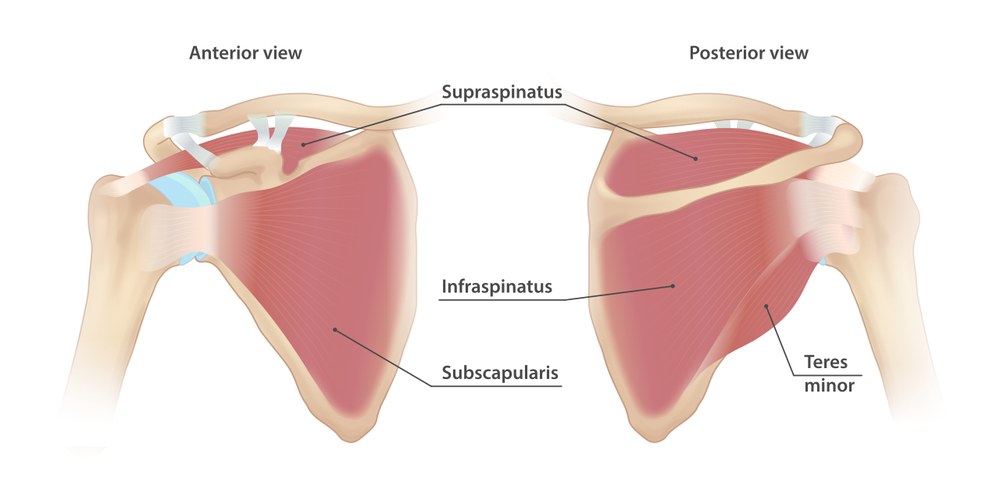
A rotator cuff tear is a completely different problem, because here the tendon has to heal back onto bone — and the junction between tendon and bone is a remarkable structure called the enthesis.
In healthy tissue the enthesis is a graded transition, built in roughly four zones: tendon → uncalcified fibrocartilage → calcified fibrocartilage → bone. This gentle gradient from soft, flexible tendon to hard, stiff bone spreads out the stress, so the soft tendon isn't simply ripped off the hard bone at a sharp boundary.
The catch is that, once torn, the body cannot rebuild that graded enthesis. A repaired cuff heals by a fibrovascular scar between tendon and bone — mechanically weaker than the original four-zone transition, and one reason rotator cuff repairs can re-tear despite well-done surgery.
It is also important that most cuff tears are degenerate rather than purely traumatic: with age, the tendon — particularly in a relatively poorly-supplied "critical zone" about a centimetre from where the supraspinatus tendon meets the bone — weakens, frays and tears with little or no injury (true cuff tears are rare before about 50). Surgery reattaches the tendon to its bony "footprint", but it is working against ageing, often poor-quality tissue. So cuff healing is fundamentally biology-limited: the operation restores the anatomy, but whether the tendon-to-bone junction truly heals depends on tendon quality, tear size, age, smoking, diabetes and how the repair is protected and loaded. This is the opposite end of the spectrum from a clean flexor laceration in a young hand — same tissue, very different healing problem.
What helps and harms tendon healing¶
- Load, correctly dosed. Controlled, progressive loading is the single most powerful tool for building tendon strength and alignment. Too much too soon ruptures the repair; too little causes stiffness and adhesions. The art of rehabilitation is the dose.
- Blood supply. Well-vascularised tendon heals better; hypovascular "watershed" zones (as in parts of the rotator cuff) heal worse.
- Smoking, diabetes, steroids and age all impair tendon healing and raise the risk of rupture and re-tear.
- Time. Tendon is slow tissue — meaningful strength takes months, and full remodelling can run beyond a year.
See also¶
- How bone heals and remodels — how the bone side of a tendon-to-bone repair behaves
- Smoking and musculoskeletal healing — why smoking slows tendon and bone healing
- Corticosteroid injections — steroids around tendons: uses and cautions