How Nerves Work and Heal PDF¶
How nerves carry signals, sense the world, and heal after injury — in plain English, with an in-depth section.
Nerves are the body's wiring. They carry tiny electrical signals between your brain and the rest of you — telling muscles to move, and carrying back what you feel: touch, temperature, position and pain. When a nerve is irritated, squashed or cut, those signals get disrupted, and you notice it as pins and needles, numbness, weakness or pain. The good news is that nerves can recover. They heal slowly and in a fairly predictable way, and understanding that pattern makes the wait far less worrying. This page explains, in plain language, what nerves do and how they mend — and then, for the curious, goes a step deeper into the biology.
What a nerve is and what it does¶
Think of a nerve as a bundle of insulated cables. Each "cable" is a single nerve fibre, and a whole nerve — like the median nerve at your wrist — contains thousands of them packed together, wrapped in protective sheaths a bit like the layers of a cable bundle.
The signals travel in two directions, so nerves do three main jobs:
- Motor — signals travel out from your brain and spinal cord to your muscles, telling them when and how hard to contract. This is how you grip, pinch and move.
- Sensory — signals travel back in from your skin, joints and tendons, carrying touch, vibration, temperature, pain and your sense of where your limb is in space.
- Autonomic — automatic background signals you never think about, controlling things like sweating and the width of small blood vessels (which is why an injured patch of skin can feel dry or change temperature).
Each fibre has a living core (the axon) that carries the signal, and many fibres are wrapped in a fatty insulation layer called myelin. Just like the plastic coating on an electrical wire, this insulation stops the signal leaking away and lets it travel much faster.
What happens when a nerve is injured¶
Nerves get into trouble in two broad ways, and the symptoms tell you which.
A squashed or compressed nerve. When a nerve is pressed on — for example the median nerve in carpal tunnel syndrome, or the funny-bone nerve at the elbow — the insulation and blood supply to that segment suffer first. The signals slow down or get blocked as they pass the squeezed spot. You feel this as pins and needles, numbness and clumsiness, often worse at night or in certain positions, and the muscles supplied by that nerve may weaken over time. Because the cable itself usually stays intact, relieving the pressure often allows a good recovery.
A cut or torn nerve. A laceration, a deep cut, or a severe stretch can divide the fibres themselves. Now the connection is physically broken: the part of the nerve beyond the injury is cut off from the brain and spinal cord, so you lose feeling and movement in everything that nerve supplied. A cleanly divided nerve usually needs to be surgically repaired — stitched together so the fibres have a path to grow back along.
The reason symptoms appear at all is simple: a signal that cannot get through is a signal that does not arrive. Block the motor fibres and the muscle weakens; block the sensory fibres and the skin goes numb or tingles; irritate the fibres and you get pain.
How nerves heal¶
Nerve healing is genuinely slow, and it helps to know that in advance so the pace doesn't feel like failure.
When fibres have been damaged, they regrow from the point of injury outwards towards the skin and muscle, at roughly one millimetre a day — about an inch a month. That rule of thumb explains a lot:
- The further the target, the longer the wait. A nerve injured high up — say near the elbow — has to regrow a long way down to reach the fingertips, which can take many months. A small cut near the fingertip recovers far sooner.
- Sensation usually returns before fine strength. As fibres reach the skin you may first notice a vague awareness, then tingling (often a buzzing or electric feeling when the area is tapped — a good sign that fibres are advancing), then crude touch, and finally finer discrimination. Power and fine coordination tend to come last.
- Early, clean repair matters. A divided nerve does best when it is repaired promptly and accurately, because the body's support cells that guide regrowth work best in the months right after injury and lose some of their effect over time.
What helps recovery: keeping the joints supple and the muscles healthy with the hand-therapy exercises you're given, protecting numb skin from burns and cuts (it won't warn you of harm), not smoking, and being patient. Re-training your brain to interpret the returning signals — through guided sensory exercises — is also part of getting a good result. If a nerve that should be improving on a timeline isn't, that's worth reviewing, as some injuries need surgery to give recovery the best chance.
In more depth¶
This section steps up to a more detailed, student-level explanation of the biology behind everything above. It isn't needed to understand your condition — but if you're curious about how the wiring actually works, read on.
The nerve cell and its membrane¶
Like the rest of your body, a nerve is built from cells — neurons. A neuron has a cell body (which holds the nucleus, the cell's control centre), short receiving branches called dendrites, and one long axon that carries the signal away — sometimes the better part of a metre.
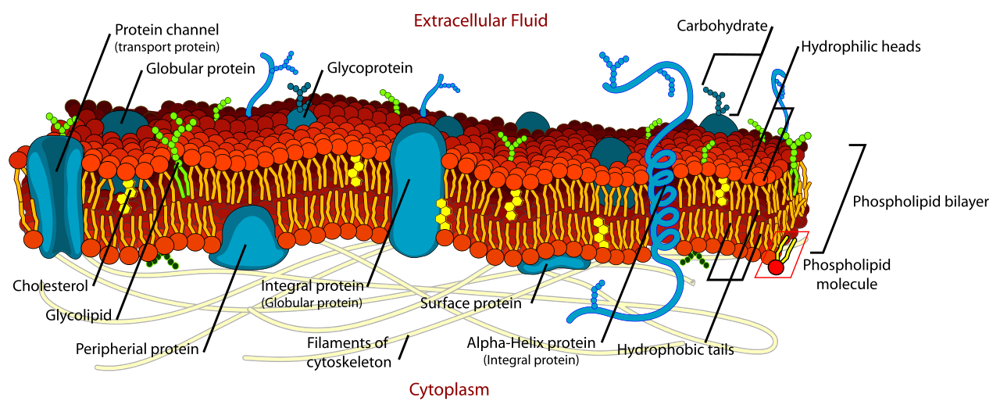
Every cell, the neuron included, is wrapped in a cell membrane, and its makeup matters for what follows. The membrane is a phospholipid bilayer — a double sheet of fatty molecules. Each phospholipid has a water-loving 'head' and two water-repelling fatty 'tails'; they line up tail-to-tail into two layers, with the heads facing the watery fluid inside and outside the cell and the oily tails tucked in the middle. This thin, fatty film is the barrier that separates inside from outside — and, crucially, it can hold an electrical charge across itself. The 'channels' and 'pumps' described in the next section are simply protein gates sitting in this fatty membrane.
The wiring: axons, myelin and nodes of Ranvier¶
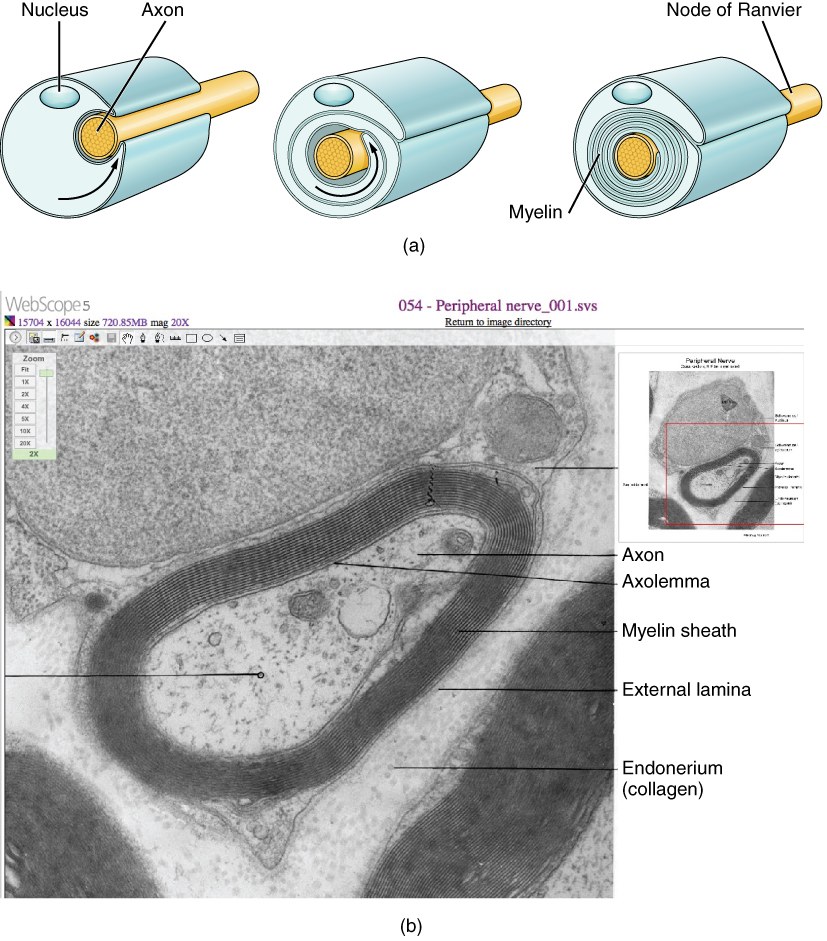
A single nerve fibre is built around an axon, a long thread-like extension of a nerve cell that carries the electrical signal. Many axons are wrapped in myelin, a fatty insulating sheath — and it is worth knowing what myelin actually is. A support cell — a Schwann cell in the peripheral nerves of your arm — wraps its own cell membrane around the axon, round and round, again and again, like rolling a sheet of cling film around a pencil dozens of times. Because that membrane is a phospholipid bilayer — fat — every wrap lays down another layer of fat, and the many stacked layers build into a thick, fatty sleeve. That sleeve of wrapped-up membrane is the insulation: myelin is mostly fat precisely because it is layer upon layer of cell membrane. The more turns the Schwann cell makes, the better insulated — and the faster — the fibre.
Crucially, the myelin sheath is not continuous. It is laid down in segments, with small bare gaps between them called the nodes of Ranvier. The electrical signal cannot leak out through the insulated stretches, so it effectively jumps from one node to the next. This is called saltatory conduction (from the Latin saltare, to leap), and it is why myelinated fibres are so fast: jumping node to node can carry a signal at speeds well over 100 metres per second, compared with under 10 metres per second in a bare, unmyelinated fibre. This is also why diseases or injuries that strip myelin slow conduction so dramatically.
How the signal travels¶
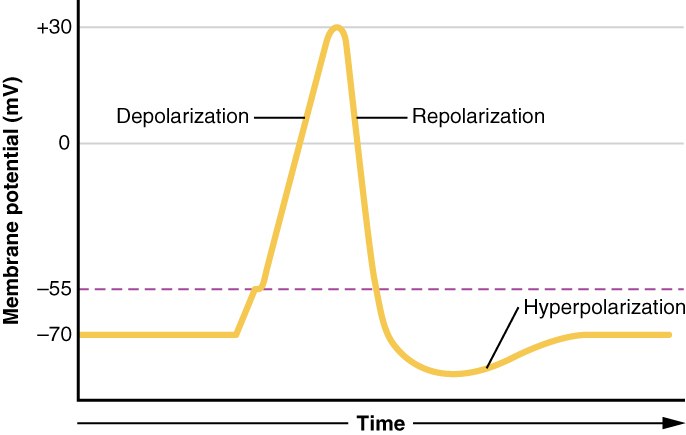
At rest, the inside of an axon is slightly negatively charged compared with the outside — the resting membrane potential, around −70 millivolts. This charge is maintained by keeping sodium ions mostly outside the cell and potassium ions mostly inside.
When the nerve fires, the sequence is precise:
- Depolarisation. Voltage-gated sodium channels snap open and sodium ions rush in. The inside swings rapidly positive, peaking around +30 millivolts. This is the action potential.
- Repolarisation. The sodium channels close and voltage-gated potassium channels open, letting potassium flow out. The inside returns towards its negative resting value.
- The refractory (latent) period. For a brief moment afterwards the patch of membrane cannot fire again, no matter how strong the stimulus, while the channels reset.
That refractory period does something elegant: because the stretch of membrane just behind the advancing signal is temporarily unable to re-fire, the action potential can only travel forwards. This is why nerve signals run in one direction along a fibre rather than bouncing back and forth.
Crossing the gap: synapses and the motor end plate¶
A nerve fibre does not physically touch the muscle it controls. Where a motor nerve meets a muscle there is a specialised junction — the neuromuscular junction — with a tiny gap (the synaptic cleft) between the nerve ending and a thickened, folded region of the muscle membrane called the motor end plate.
The electrical signal cannot cross that gap directly, so it is converted into a chemical one. When the action potential reaches the nerve ending, it triggers the release of a neurotransmitter called acetylcholine into the gap. Acetylcholine drifts across and binds to receptors on the motor end plate, opening channels that let the muscle membrane depolarise. If that depolarisation reaches threshold, it launches an action potential through the muscle and the fibre contracts. An enzyme (acetylcholinesterase) then quickly breaks the acetylcholine down, so each nerve impulse produces one crisp twitch rather than a lingering one. This chemical relay is the target of some anaesthetic drugs and of conditions such as myasthenia gravis.
Sensing the world: sensory receptors¶
The sensory side works in reverse: specialised endings convert a physical stimulus into nerve signals. Different receptors are tuned to different things:
- Pacinian corpuscles sit deep in the skin and respond to deep pressure and high-frequency vibration. They adapt quickly, firing at the moment something changes rather than continuously.
- Meissner's corpuscles lie just under the surface of fingertip and palm skin and detect light touch and low-frequency flutter — central to the fine, discriminating touch you use to feel textures and handle small objects.
- Free nerve endings are bare, unencapsulated endings that sense pain, temperature and light touch. They are the most numerous endings in the skin.
- Muscle spindles sit inside the muscles themselves and detect stretch and length, feeding back information about position and movement (proprioception) — how the brain knows where your hand is without looking.
The different qualities you can feel — a pinprick, warmth, a buzzing phone, the position of your wrist — are largely a matter of which of these receptors are firing and how fast.
Grades of nerve injury¶
Surgeons grade nerve injury by how deep the damage goes, because that determines how — and whether — it will recover. Two classifications are used together.
The older, simpler Seddon system has three categories:
- Neurapraxia — the mildest. The fibres are bruised or the insulation locally disrupted, but the axons stay intact. Conduction is blocked at that spot, like a kinked hose, but the structure is sound. Recovery is usually full and relatively quick once the cause is relieved.
- Axonotmesis — the axons themselves are torn, but the surrounding connective-tissue tubes survive. The fibres beyond the injury die back and must regrow, so recovery is slow but the preserved tubes give the new fibres a path to follow — and the outlook is often good.
- Neurotmesis — the most severe. The nerve, including its supporting framework, is completely divided. It will not recover on its own; surgical repair is needed, and even then recovery is incomplete.
The more detailed Sunderland system splits this into five grades, mapping onto Seddon as follows:
- Grade 1 = neurapraxia (conduction block only).
- Grade 2 = axonotmesis with the innermost tube (endoneurium) intact — the best regrowth prospects.
- Grade 3 = the inner tube is also disrupted, so regrowing fibres can be misdirected; recovery is partial.
- Grade 4 = only the outer sheath (epineurium) remains intact; a scar block usually prevents useful recovery without surgery.
- Grade 5 = complete division of the whole nerve — equivalent to Seddon's neurotmesis — requiring repair.
In short: the more layers that are torn, the slower and less complete the natural recovery, and the more likely surgery is needed.
Wallerian degeneration and regrowth¶
When an axon is cut or torn, the part of it beyond the injury is now disconnected from the cell that keeps it alive. Over the following days it breaks down in a tidy, programmed process called Wallerian degeneration: the stranded axon and its myelin are dismantled and cleared away by Schwann cells and recruited immune cells (macrophages).
This is not just demolition — it is preparation. The Schwann cells that lined the old fibre survive, multiply, and line up in hollow columns called the bands of Büngner, following the original route of the nerve. These columns act as living scaffolding tubes: they release growth factors and physically guide regenerating fibres back towards their targets.
From the injury site, the surviving end of each axon sends out a growth cone that creeps down its Schwann-cell tube at about one millimetre a day, eventually reaching the skin or muscle and reconnecting (reinnervation). This is why a clean repair, done early and accurately, matters so much: the cut tubes need to be lined up so fibres re-enter the correct channels, and the Schwann cells are most supportive in the months soon after injury — they have, in effect, a "best before" date. Line the ends up well and reach them in time, and far more fibres find their way home.
See also¶
- Nerve tests and conduction studies — how we measure whether a nerve is conducting normally
- Carpal tunnel and nerve compression — a common compressed-nerve problem at the wrist
- Tendon and nerve repair — what surgical repair of a divided nerve or tendon involves