Patients › Rehabilitation
Dupuytren's Release
Rehabilitation after Dupuytren's fasciectomy — the extension splint regime and exercise program, with hand-therapist follow-up.

This protocol guides your recovery after surgical release of Dupuytren's contracture (fasciectomy) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. The two pillars of a good result are the splint, which holds the freed fingers straight while everything heals, and the exercise program, which keeps them moving. Bring this page or its PDF to your hand therapist so your rehabilitation stays coordinated.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
Surgery for Dupuytren's disease removes the diseased cords of tissue that were pulling your fingers into the palm, restoring the ability to straighten them. The condition itself is explained on the Dupuytren's disease page; there is no permanent cure, and the goal of surgery is to excise the diseased tissue and restore finger extension.
You will usually be referred to a hand therapist 2–3 days after surgery. The therapist will make you a custom plastic splint that holds the operated fingers in an extended (straight) position, and will start you on the gentle exercise program below. The splint and the exercises work together: the splint defends the straightness the surgery won, and the exercises keep the fingers bending so they don't stiffen.
Keep the wound clean and dry until your sutures are removed. Once the sutures are out you can get the skin wet, but avoid soaking or submerging the hand in water for another week. The practice's wound care page covers dressings, signs of infection and scar care in detail. Scar massage matters after Dupuytren's surgery, and your therapist will guide it once the wound has healed.
Caring for your scar¶
The scar in the palm is often firm, raised and tender for the first weeks after Dupuytren's surgery before it gradually softens and fades over the following months. Scar massage is a routine part of Australian hand-therapy care: in a national survey of accredited hand therapists, almost all used it after hand surgery (typically starting around suture removal, once the wound has fully healed) to soften the scar, improve how the skin glides over the tissues beneath, and settle scar sensitivity, usually combined with silicone gel or sheeting rather than used on its own [6]. The research evidence behind scar massage is still developing, but it supports its use for reducing scar-related discomfort and improving movement [6]. Your therapist will show you the technique and may add a silicone product, often worn at night alongside the splint.
Recovery, work and the long term¶
Swelling and stiffness are normal in the early weeks and settle as the hand is used; comfort, motion and grip generally keep improving over several months. Keeping the hand elevated and gently moving in those early weeks helps the swelling settle and guards against the small joints stiffening. The straightness gained at surgery is usually well maintained through this period. In a randomised trial of rehabilitation after Dupuytren's release, most operated fingers held or improved their extension over the first three months of hand therapy [2].
Time off work depends on what you do with your hands. In a study of more than 2,500 people treated for Dupuytren's disease, the median return to work after open fasciectomy was about two weeks, and around nine in ten people were back at work within the year; physically demanding jobs took longer [4]. Dr Hirpara will discuss timing for your particular work at review; heavier manual work usually waits until the wound is soundly healed and grip is comfortable.
Because Dupuytren's is a lifelong condition, some tightness can return over the years, and reported recurrence rates vary widely between studies depending on how recurrence is defined. The long-term picture is generally reassuring: in a follow-up of 142 fasciectomies over roughly four years using the modern consensus definition, true recurrence of contracture occurred in around 3–4% of hands, although about a third kept some residual curvature, usually mild and well short of the contracture corrected at surgery [5]. The splint, scar care and exercise program are all aimed at protecting your result; if a finger does begin to tighten again at any point, let the rooms know.
Your splint¶
- First week or so: wear the splint day and night, removing it only for your exercises (and washing, once permitted).
- After the first week: most people move to night-only splint wear, and can begin using the hand for light activity during the day.
- Night splinting continues for about 3 months (and in some cases up to 6 months) to protect against the fingers drifting back toward the palm while the tissues mature.
- Your hand therapist and Dr Hirpara will advise you specifically about your splint-wear schedule and activity. The timings above are the usual pattern, not a fixed rule.
You must not drive while your hand is in the splint. Once you move to night-only wear, daytime driving can resume as comfort and a safe grip on the wheel allow.
For your physiotherapist / hand therapist:
Management
- Referral 2–3 days post-operatively for fabrication of a thermoplastic extension splint
- Splint regime: day and night for approximately the first week (off for exercises), then night-only with light functional day use; night splinting continued for approximately 3 months (up to 6 months where needed), per surgeon/therapist review
- Home exercise program as per the cards below: active extension, blocked DIP flexion, DIP/PIP flexion over a pen, composite flexion, wrist tenodesis
- Wound care per the practice's wound care guidance; scar management once healed
- Repetitions and daily frequency set by the treating therapist
Precautions
- Keep the wound clean and dry until suture removal; no soaking/submersion for a further week after
- Splint compliance is central to maintaining the extension gained at surgery
- No driving while the hand is in the splint
These are the exercises from your handout, started with your hand therapist and continued at home.
Your exercises¶
Kieran Hirpara 4.0
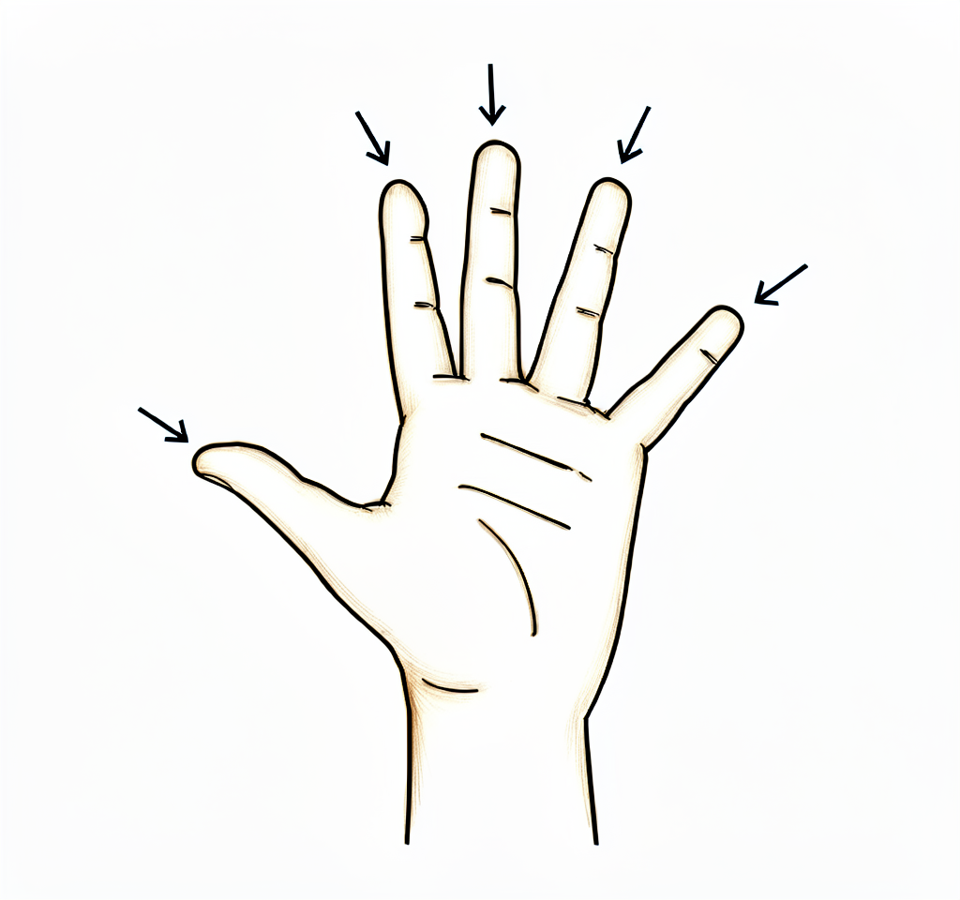
Active extension
With your wrist straight, straighten and spread your fingers as far as you can. You may assist gently with your other hand. Relax and repeat.
As prescribed by your hand therapist
Kieran Hirpara 4.0
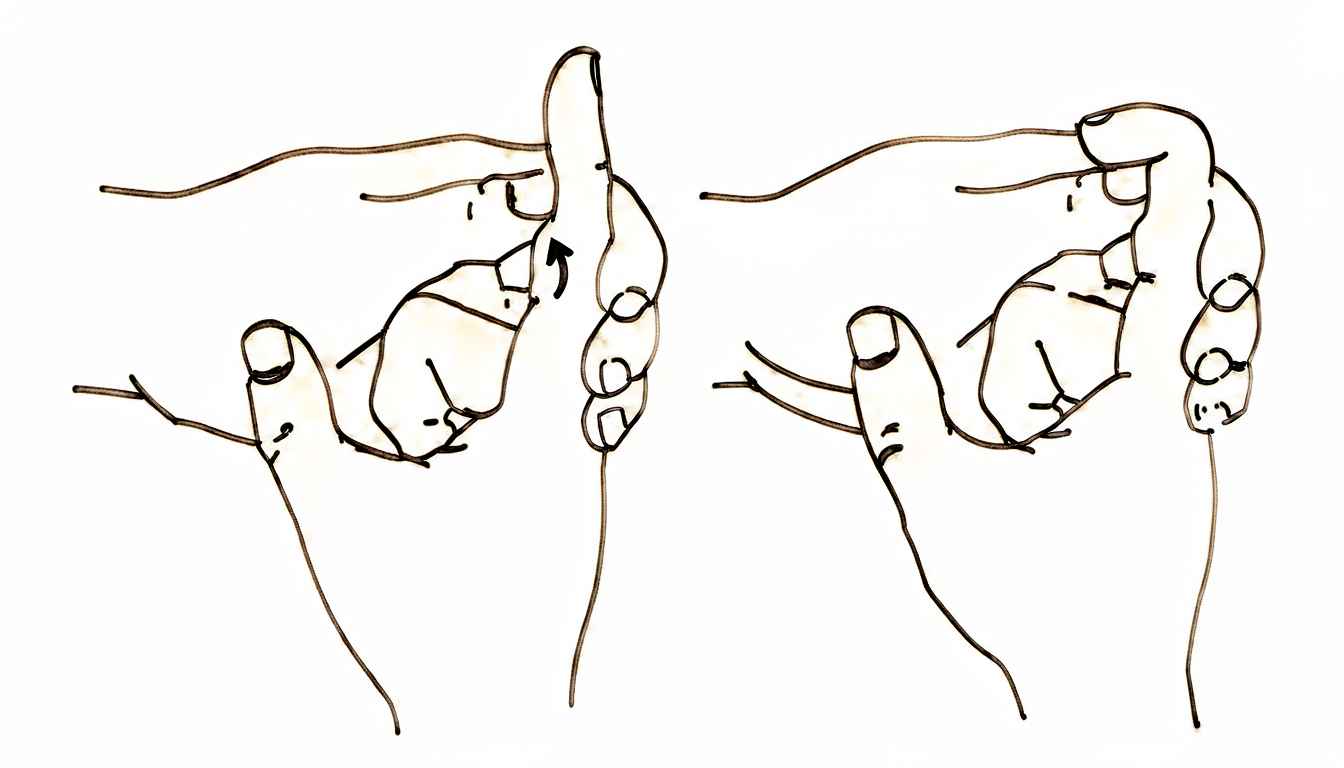
Active DIP flexion
Support the finger just below the crease of the end (DIP) joint with your other hand. Bend the end joint firmly, then relax.
As prescribed by your hand therapist
Kieran Hirpara 4.0
Active DIP/PIP flexion
Place a pen across the base of your fingers. Curl your fingers around the pen so that both finger joints (the middle and end joints) bend, then relax.
As prescribed by your hand therapist
Kieran Hirpara 4.0
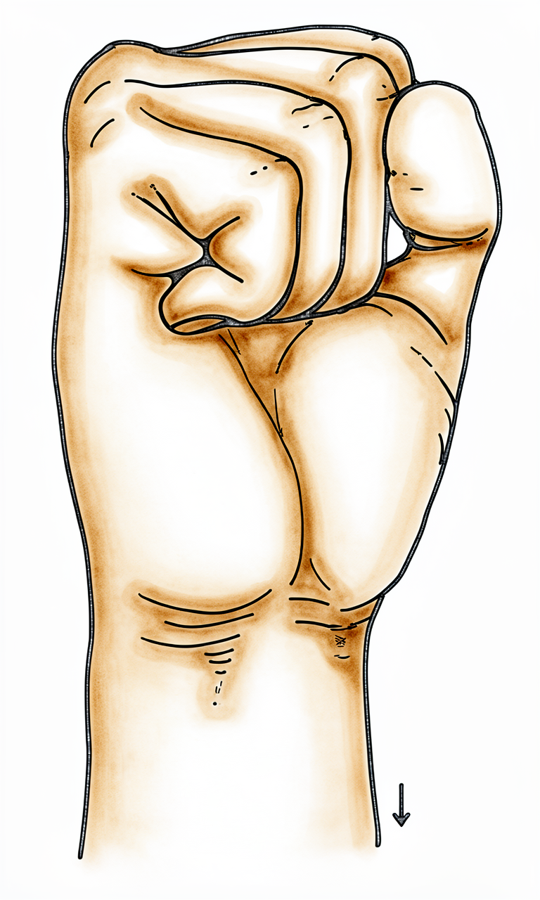
Composite flexion
Gently make a loose fist, then relax and let the fingers straighten.
As prescribed by your hand therapist
Kieran Hirpara 4.0
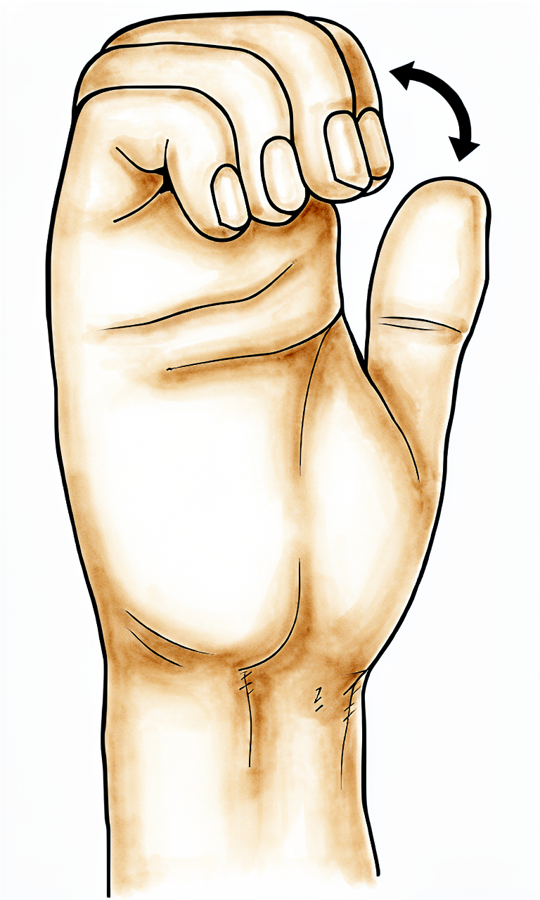
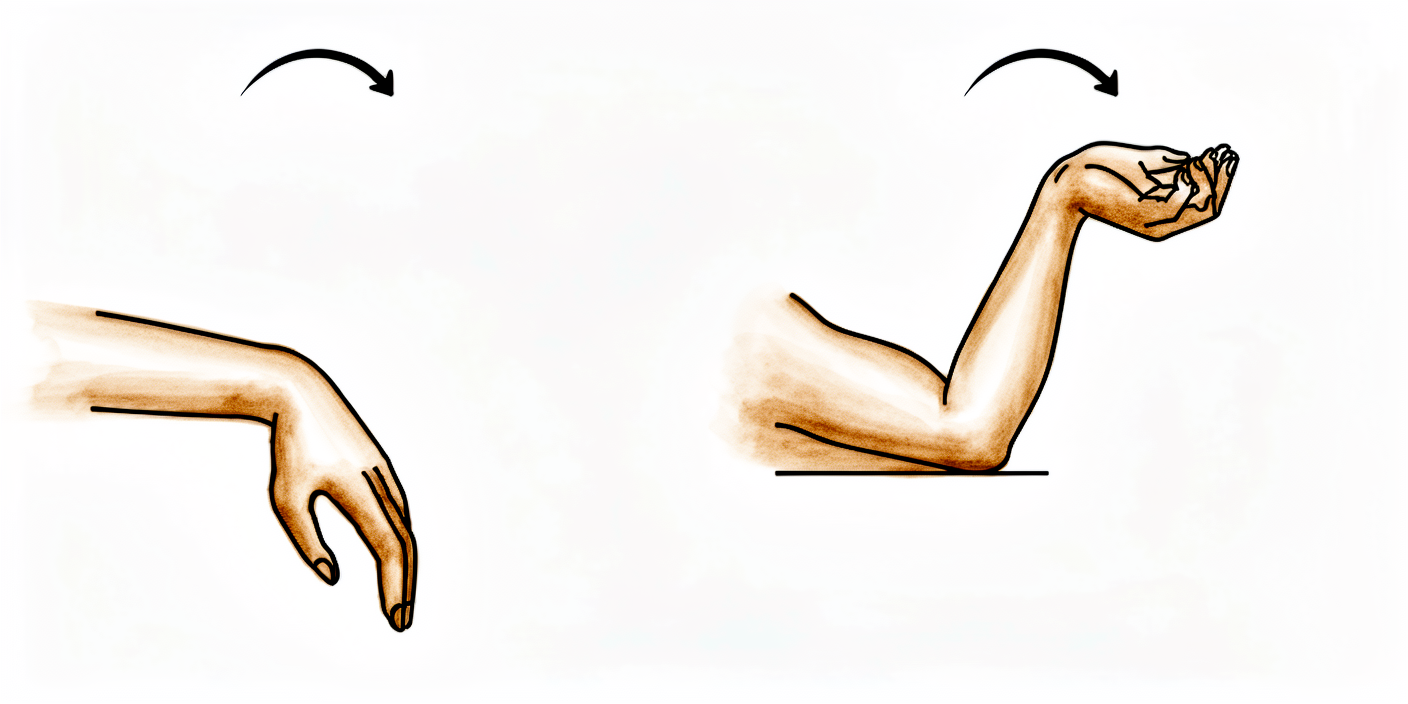
Wrist tenodesis
Resting on your elbow with your fingers relaxed, bend your wrist forwards and then backwards, letting the fingers follow naturally.
As prescribed by your hand therapist
After your protocol¶
This protocol was written in association with Ruby Doolan, Accredited Hand Therapist, Extend Rehabilitation. It works alongside the practice's general recovery advice: see managing post-operative pain, wound care and hand therapy basics. For the operation itself, see Dupuytren's fasciectomy.
The recovery expectations, return-to-work figures and scar-care guidance above are drawn from published trials, reviews and surveys of rehabilitation after Dupuytren's surgery, including randomised trials and a systematic review of splinting and hand therapy after fasciectomy [1–3]. The splint regime and exercise program are the practice's own, agreed between Dr Hirpara and your hand therapist, and your splint-wear schedule is individualised at your reviews.
References
- Jerosch-Herold C, Shepstone L, Chojnowski AJ, Larson D, Barrett E, Vaughan SP. Night-time splinting after fasciectomy or dermo-fasciectomy for Dupuytren's contracture: a pragmatic, multi-centre, randomised controlled trial. BMC Musculoskeletal Disorders. 2011;12:136.
- Collis J, Collocott S, Hing W, Kelly E. The effect of night extension orthoses following surgical release of Dupuytren contracture: a single-center, randomized, controlled trial. Journal of Hand Surgery (American). 2013;38(7):1285–1294.e2.
- Karam M, Kahlar N, Abul A, Rahman S, Pinder R. Comparison of hand therapy with or without splinting postfasciectomy for Dupuytren's contracture: systematic review and meta-analysis. Journal of Hand and Microsurgery. 2022;14(4):308–314.
- Blake SN, Poelstra R, Andrinopoulou ER, et al. Return to work and associated costs after treatment for Dupuytren's disease. Plastic and Reconstructive Surgery. 2021;148(3):580–590.
- Radhamony NG, Nair RR, Sreenivasan S, et al. Residual deformity versus recurrence following Dupuytren's palmar fasciectomy — a long-term follow-up of 142 cases. Annals of Medicine and Surgery. 2022;73:103224.
- Scott HC, Robinson LS, Brown T. Scar massage as an intervention for post-surgical scars: a practice survey of Australian hand therapists. Hand Therapy. 2024;29(1):21–29.
Evidence & references
Dupuytren Contracture — Surgical Release & Post-operative Hand-Therapy Rehabilitation (Open Fasciectomy)¶
Topic scope: post-operative rehabilitation after open excision of diseased palmar/digital fascia for Dupuytren contracture — limited/regional fasciectomy, extending to dermofasciectomy (fascia plus overlying involved skin, replaced with a graft) for aggressive or recurrent disease. The procedure-selection literature (fasciectomy vs needle aponeurotomy vs collagenase) is summarised only as far as it frames recurrence expectations and rehabilitation; the rehab focus is the post-fasciectomy pathway — early active and passive finger extension and flexion, oedema control, scar management, and night extension splinting.
Defining principle of this rehab: fasciectomy removes diseased tissue and restores extension that the disease had taken away — it does not cure the diathesis, and the corrected finger sits in a tissue bed that wants to contract back. So the rehab is a "regain-and-hold" pathway: early motion to keep the freed joints supple and prevent the new flexor-tendon and skin-glide planes from binding down, oedema and scar control so the soft tissues mature without tethering, and a night extension orthosis to defend the surgical correction during healing. The defining clinical question is not whether a construct needs protection (there is no construct), but how aggressively to splint — and here the evidence has shifted decisively toward selective, not routine, splinting.
A. PROCEDURE OUTCOMES & RECURRENCE (context for the rehab)¶
Open partial (limited) fasciectomy is the long-standing reference operation for Dupuytren contracture and gives the most durable correction of the three mainstream options:
- Correction is reliable and recurrence is the dominant long-term limitation. Across modern series the operation restores extension well, but Dupuytren is a lifelong diathesis and some tightening returns over years. Reported recurrence rates vary enormously because studies define recurrence differently (any palpable disease vs a threshold extension loss vs need for re-intervention). Using the modern consensus definition, true recurrence of contracture is low at medium-term follow-up, though a substantial minority retain mild residual curvature well short of the pre-operative deformity [corpus: jhsa.2012.06.032; literature: Radhamony 2022].
- Fasciectomy vs minimally invasive options. Compared with needle aponeurotomy/fasciotomy and collagenase Clostridium histolyticum, open fasciectomy has a longer recovery and higher minor complication rate but lower recurrence — the recurring trade-off in this disease. Needle and collagenase are quicker with faster return to function but recur sooner [corpus: jhsa.2021.05.022; jhsa.2011.08.004; 1753193418786947]. This trade-off is why fasciectomy is typically chosen for denser, multi-ray or PIP-predominant contractures — the same cases whose rehab is hardest and whose splinting is most likely to be justified.
- Repeat limited fasciectomy for recurrence is safe and effective, supporting fasciectomy as a durable, repeatable mainstay rather than a one-shot procedure [corpus: bjj-2020-1393.r2].
Why this matters for rehab: recovery counselling and splint expectations must be framed against a disease that cannot be cured, only corrected — the rehab protects a correction, it does not prevent the diathesis.
B. THE SPLINTING CONTROVERSY (the central rehab question)¶
Historically, every patient was issued a static night extension orthosis after fasciectomy on the assumption it preserved the correction. The best available evidence does not support routine splinting — it supports selective splinting for patients who lose extension.
- Jerosch-Herold 2011 (pragmatic multi-centre RCT, n = 154). Hand therapy alone vs hand therapy + night splinting after fasciectomy/dermofasciectomy. No between-group difference in self-reported function (DASH), finger range of motion, or satisfaction. Authors concluded routine night splinting for all patients is not recommended, reserving it for cases where extension deficits recur [literature: Jerosch-Herold 2011, BMC Musculoskelet Disord].
- Collis 2013 (single-centre RCT, n = 56). Night extension orthosis + hand therapy vs hand therapy alone after surgical release. No significant difference in total active extension or any secondary outcome at 3 months. Same conclusion: provide an orthosis selectively, when extension loss occurs, not universally [corpus: jhsa.2013.04.012; literature: Collis 2013].
- Karam 2022 (systematic review + meta-analysis, 4 RCTs, n = 295). Pooling the splint-vs-no-splint trials found no significant difference in total active flexion/extension, DASH, pain, grip or satisfaction. The collective signal is consistent and now moderately strong: adding a splint to good hand therapy does not improve the average outcome [corpus: 1055/s-0041-1725221; literature: Karam 2022].
- Earlier/smaller work (e.g., post-fasciectomy splinting pilot studies) pointed the same way — splinting is low-yield as a blanket policy [corpus: 1753193412437631].
Practical reading for this protocol. The practice's pattern — splint day-and-night for ~1 week, then night-only with a low threshold to continue (or reinstate) splinting if a finger starts to drift back into flexion — is a reasonable, evidence-aligned middle path: it defends the correction during the highest-risk early healing window and during sleep, while honouring the trial finding that indefinite routine splinting adds little. The trials measured average outcomes; they do not say splinting is useless for the individual who is losing extension, which is exactly the subgroup the authors carved out. This is a defensible selective-splinting stance, not a contradiction of the protocol.
C. HAND-THERAPY & EXERCISE EVIDENCE¶
- Early supervised hand therapy is the backbone of recovery and is where the demonstrable benefit lies (the splint trials all compared against a hand-therapy baseline, not against nothing). Active and passive extension and flexion, oedema control and scar management are standard from the first post-operative therapy visit, typically 2–3 days after surgery.
- Most operated fingers hold or improve their extension over the first three months of hand therapy — the window in which the protocol concentrates splinting and exercise [corpus: jhsa.2013.04.012, control arm; literature: Collis 2013].
- Scar management. Scar massage is near-universal in hand-therapy practice after Dupuytren surgery to soften the palmar scar, improve skin glide and settle sensitivity, generally combined with silicone gel/sheeting and begun around suture removal once the wound is healed. The supporting evidence is developing rather than definitive but favours reduced scar-related discomfort and improved movement [literature: Scott 2024, Australian hand-therapist survey].
- Return to work. In a large cohort, median return after open fasciectomy was ~2 weeks with ~90% back at work within the year; physically demanding jobs took longer [literature: Blake 2021].
- Pre-operative hand therapy has a thinner evidence base and is not a substitute for the post-operative programme [corpus: 17589983241227162].
Phased rehabilitation timeline (matching the synthesis phases)¶
| Phase | Window | Splint | Movement / use | Scar & oedema | Notes |
|---|---|---|---|---|---|
| I — Protect & mobilise | ~Days 2–7 | Custom thermoplastic extension orthosis day & night, off for exercises | Gentle active extension + active DIP/PIP and composite flexion from the first therapy visit; wrist tenodesis | Oedema control (elevation, gentle movement); wound kept clean & dry | Therapy referral 2–3 days post-op; splint defends the surgical correction during the highest-risk window |
| II — Restore motion | ~Week 1 → 6–8 | Transition to night-only; light functional day use of the hand | Progress active + passive extension and flexion; restore full composite fist and full extension | Scar massage + silicone once wound healed (around suture removal) | Most extension is held or regained through this window; daytime driving resumes once out of the splint and grip is safe |
| III — Strengthen & return | ~Week 6–8 → 3 months | Night-only continues ~3 months (up to ~6 months selectively if extension is being lost) | Grip and functional strengthening; return to heavier manual work as wound is soundly healed and grip comfortable | Ongoing scar maturation over months | Splinting beyond this window is selective, driven by extension loss — not routine (see §B) |
The phase structure and timings are protocol/consensus, agreed between the surgeon and hand therapist; the trials inform the splinting policy within them, not the exact week boundaries.
D. COMPLICATIONS (rehab-relevant)¶
- Flare reaction / early CRPS-spectrum. A proportion of patients develop a post-operative inflammatory "flare" — disproportionate swelling, stiffness, redness and pain — which can progress to complex regional pain syndrome (CRPS type 1). Early recognition, oedema control, gentle continued motion and analgesia matter; CRPS is one of the more feared rehab-derailing complications after hand surgery [corpus: jht.2024.09.002 (Dupuytren CRPS-1 case); hcl.2009.11.001 (CRPS after hand surgery)].
- Digital nerve / vessel injury. The neurovascular bundles are displaced by Dupuytren cords, especially in recurrent disease and at the PIP; injury is a recognised operative risk. New sensory change post-operatively warrants surgeon review [corpus: hansur.2017.07.002 — complications systematic review; 17531934231206317 — surgical complications/adverse events].
- Wound healing, haematoma, infection, stiffness. Open fasciectomy has a higher minor-complication rate than the minimally invasive options; meticulous wound care and early motion mitigate stiffness and tethering [corpus: hansur.2017.07.002].
- Incomplete correction / residual PIP deficit. PIP contractures correct less completely than MCP; residual deficit may persist and is the usual trigger for selective ongoing splinting.
E. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Routine vs selective splinting — the headline controversy, now reasonably settled toward selective: three RCTs and a meta-analysis show no average benefit from adding a static night orthosis to good hand therapy, with all authors carving out the extension-loss subgroup. The practice's "night-only, low threshold to continue if drifting" approach is consistent with this. Moderate (multiple RCTs + SR/MA).
- Recurrence is definition-dependent — headline recurrence figures are not comparable across studies; the consensus definition gives lower, more credible rates. Counsel against the cure expectation. Moderate.
- Procedure choice frames rehab — fasciectomy trades a longer recovery and more minor complications for lower recurrence than needle/collagenase. The fasciectomy cohort is, by selection, the harder-rehab cohort. Moderate.
- The phase timings are consensus — drawn from surgeon/therapist protocols, not a rehab RCT. The splinting policy within them is trial-informed; the week boundaries are typical, not trial-derived. Weak/consensus.
F. EVIDENCE STRENGTH FLAGS (summary)¶
- MODERATE (multiple RCTs + SR/MA): routine night splinting adds no average benefit over hand therapy alone after fasciectomy — splint selectively for extension loss (Jerosch-Herold 2011; Collis 2013; Karam 2022 meta-analysis of 4 RCTs / 295 patients).
- MODERATE (cohorts / comparative): fasciectomy gives durable correction with lower recurrence but longer recovery and more minor complications than needle aponeurotomy/collagenase; repeat fasciectomy is safe and effective; CRPS and digital-nerve injury are recognised rehab-relevant complications.
- WEAK / CONSENSUS: the post-operative phase structure and timings themselves (surgeon + hand-therapist protocol; no defining rehab RCT). Scar-massage benefit is supportive but the evidence base is still developing.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Correction of contracture and recurrence rates of Dupuytren contracture following fasciectomy. J Hand Surg Am. 2012. DOI: 10.1016/j.jhsa.2012.06.032
- Repeat limited fasciectomy is a safe and effective treatment for recurrence of Dupuytren's contracture. Bone Joint J. 2021. DOI: 10.1302/0301-620X.103B5.BJJ-2020-1393.R2
- Limited fasciectomy versus collagenase Clostridium histolyticum for Dupuytren contracture. J Hand Surg Am. 2021. DOI: 10.1016/j.jhsa.2021.05.022
- The efficacy and safety of fasciectomy and fasciotomy for Dupuytren's contracture. J Hand Surg Eur. 2011. DOI: 10.1177/1753193410397971
- Cost-effectiveness of open partial fasciectomy, needle aponeurotomy, and collagenase injection for Dupuytren contracture. J Hand Surg Am. 2011. DOI: 10.1016/j.jhsa.2011.08.004
- Three-year recurrence of Dupuytren's contracture after needle fasciotomy and collagenase injection. J Hand Surg Eur. 2018. DOI: 10.1177/1753193418786947
- The effect of night extension orthoses following surgical release of Dupuytren contracture: a single-centre RCT. J Hand Surg Am. 2013. DOI: 10.1016/j.jhsa.2013.04.012
- Comparison of hand therapy with or without splinting postfasciectomy for Dupuytren's contracture: systematic review and meta-analysis. J Hand Microsurg. 2022. DOI: 10.1055/s-0041-1725221
- Does use of a night extension orthosis improve outcomes in patients with Dupuytren contracture? J Hand Surg Glob Online. 2021. DOI: 10.1016/j.jhsg.2021.05.001
- A pilot study assessing the effectiveness of postoperative splinting after limited fasciectomy. J Hand Surg Eur. 2012. DOI: 10.1177/1753193412437631
- Pre-operative hand therapy management of Dupuytren's disease: a systematic review. Hand Ther. 2024. DOI: 10.1177/17589983241227162
- Current concepts in the management of Dupuytren disease of the hand. J Am Acad Orthop Surg. 2020. DOI: 10.5435/JAAOS-D-20-00190
- Complications after treating Dupuytren's disease: a systematic literature review. Hand Surg Rehabil. 2017. DOI: 10.1016/j.hansur.2017.07.002
- Surgical complications: errors and adverse events (hand surgery). J Hand Surg Eur. 2023. DOI: 10.1177/17531934231206317
- The case of a woman with bilateral Dupuytren's contractures who developed CRPS-1. J Hand Ther. 2024. DOI: 10.1016/j.jht.2024.09.002
- Complex regional pain syndrome after hand surgery. Hand Clin. 2009. DOI: 10.1016/j.hcl.2009.11.001
Splinting & hand-therapy literature (URLs)¶
- Jerosch-Herold C, Shepstone L, Chojnowski AJ, et al. Night-time splinting after fasciectomy or dermo-fasciectomy for Dupuytren's contracture: a pragmatic, multi-centre, randomised controlled trial. BMC Musculoskelet Disord. 2011;12:136. https://pmc.ncbi.nlm.nih.gov/articles/PMC3146906/
- Collis J, Collocott S, Hing W, Kelly E. The effect of night extension orthoses following surgical release of Dupuytren contracture: a single-centre, randomised, controlled trial. J Hand Surg Am. 2013. https://pubmed.ncbi.nlm.nih.gov/23790420/
- Karam M, Kahlar N, Abul A, et al. Comparison of hand therapy with or without splinting postfasciectomy for Dupuytren's contracture: systematic review and meta-analysis. J Hand Microsurg. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC10042625/
- Blake SN, Poelstra R, Andrinopoulou ER, et al. Return to work and associated costs after treatment for Dupuytren's disease. Plast Reconstr Surg. 2021. https://pubmed.ncbi.nlm.nih.gov/34292887/
- Radhamony NG, Nair RR, Sreenivasan S, et al. Residual deformity versus recurrence following Dupuytren's palmar fasciectomy — long-term follow-up of 142 cases. Ann Med Surg. 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC8767281/
- Scott HC, Robinson LS, Brown T. Scar massage as an intervention for post-surgical scars: a practice survey of Australian hand therapists. Hand Ther. 2024. https://pmc.ncbi.nlm.nih.gov/articles/PMC10901164/
Society guidance & published rehab protocols¶
- The British Society for Surgery of the Hand (BSSH) — Dupuytren's disease patient and professional guidance. https://www.bssh.ac.uk/patients/conditions/25/dupuytrens_disease
- BSSH — Assessing the outcome of surgery for Dupuytren's disease of the hand. https://www.bssh.ac.uk/assessing_the_outcome_of_surgery_for_dupuytrens_disease_of_the_hand.aspx