Patients › Shoulder
Rotator Cuff Repair
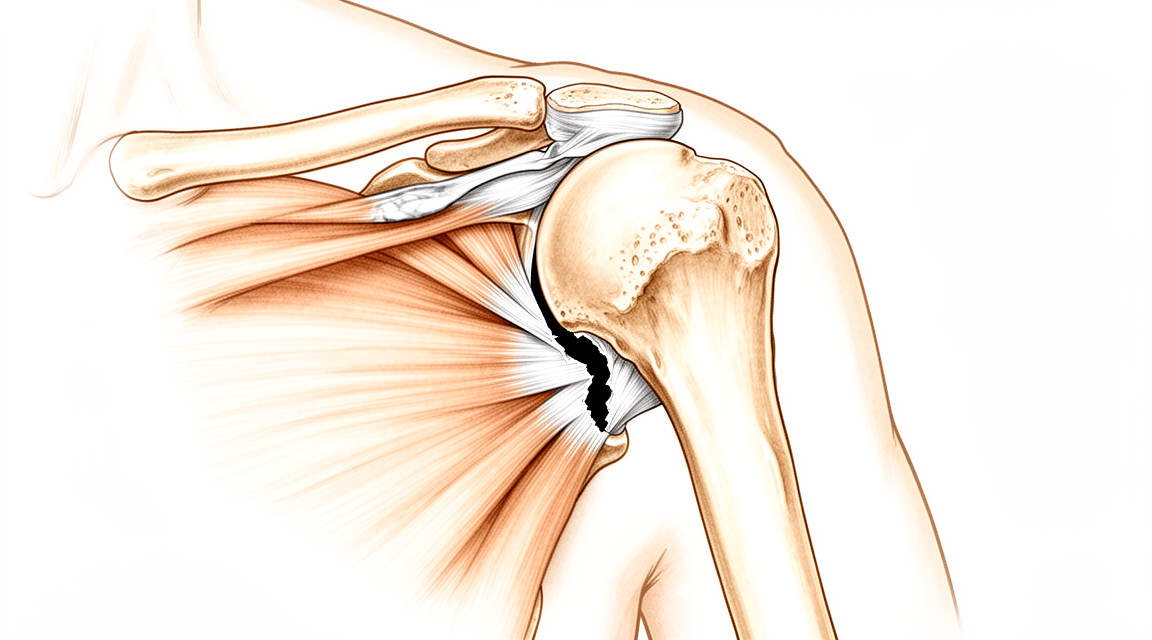
Rotator cuff repair reattaches torn tendons to bone, improving pain and function when conservative treatment fails.
Why this operation has been suggested¶
Rotator cuff repair is a procedure to reconnect torn shoulder tendons to the bone. Dr Kieran Hirpara, an upper-limb surgeon at Mater Private Hospital Rockhampton, approaches this in our clinic by focusing on restoring your shoulder’s function. You typically reach our clinic via a GP or physiotherapist referral. We use imaging to confirm the tear’s size and location.
For long-standing wear-and-tear problems, we usually start with non-operative care. This includes activity changes, physiotherapy, and injections. We consider surgery when these steps do not give enough improvement. For acute tears from injury, we may recommend surgery sooner. The main benefit is reducing pain and improving your ability to lift and move your arm. Our practice uses an arthroscopic approach with small incisions and a camera inside the joint.
Before the operation¶
We ask you to fast for six hours before your arthroscopic rotator cuff repair. Please stop taking blood-thinning medications as directed by your surgeon. Arrange for a responsible adult to drive you home and stay with you overnight. Bring a complete list of all current medications and wear loose, comfortable clothing. You may need an X-ray, MRI, or blood test to check your joint and overall health. An anaesthetic review ensures your pain management plan is safe. These steps help us prepare for a smooth procedure and recovery.
On the day¶
You will arrive at the hospital for admission. This operation is done under general anaesthetic combined with a regional nerve block. You will be fully asleep for the operation, and the block — an injection that numbs the nerves supplying the arm before you wake up — provides pain relief for the first 12 to 24 hours after surgery. The anaesthetist will meet you before the operation and talk you through both parts.
We then take you to the operating theatre. Your surgeon performs this operation as an arthroscopic (keyhole) approach with two or three small incisions and a small camera inside the joint. This method allows us to see the tear clearly while minimising injury to your shoulder muscles. After the procedure, you will wake up in our recovery area. Our team will monitor your comfort and ensure you are stable before you head home.
What the operation involves¶
We perform this surgery using an arthroscopic approach, often called keyhole surgery. This method is preferred because it allows us to see inside your shoulder clearly while causing less damage to your muscles. We make two or three small cuts, each about 1 cm long, over the front of your shoulder. Through these small openings, we insert a tiny camera and special tools. This lets us view the joint from multiple angles to fully assess the tear and any other issues inside the shoulder.
First, we carefully release any tight tissue or adhesions that are stopping your tendon from moving freely. Think of the torn tendon like a frayed rope that has pulled away from its anchor point on the bone. We gently pull this tendon back down to its original position on the bone head. To hold it there securely, we use small anchors made of biodegradable material. These anchors are screwed into the bone, and strong sutures (stitches) are passed through them to tie the tendon firmly in place.
We often use a double-row technique, which means we place anchors in two rows. This provides extra points of fixation and helps cover the entire area where the tendon attaches to the bone. This method compresses the tendon down to the bone, mimicking the natural anatomy more closely than older single-row methods. After the tendon is secured, we check that it is stable and that your shoulder can move safely. Finally, we close the small cuts with dissolving stitches or glue and apply a dressing to protect the area while you begin your recovery.
After the operation¶
You will wake up in the recovery ward with your arm in a sling and a dressing over the small incisions. We use an arthroscopic (keyhole) approach with two or three small incisions and a small camera inside the joint. Pain control is managed through general methods tailored to your needs. Most patients stay one night in hospital after this operation, though some are able to go home the same day. You must have someone stay with you for the first 24 hours. You cannot drive for at least SIX WEEKS after any shoulder operation, regardless of which arm was operated on. Patients in a sling must NOT drive. Once your surgeon clears you, typically at the six-week review, you may resume driving. See Driving after upper-limb surgery for full details.
Recovery¶
You will notice swelling and stiffness in your shoulder during the early days. This is normal as your body heals from the keyhole surgery. We use small incisions and a camera to repair the tendon, which helps keep tissue trauma low. You can expect some discomfort, but our team will provide a pain management plan tailored to your needs. This often includes medication and ice to help you rest comfortably.
For the first few weeks, you will wear a sling to protect the repair. You must not drive while wearing the sling. Our policy requires you to wait until your surgeon clears you, typically at the six-week review, before driving again. This applies regardless of which shoulder was operated on. Please read our Driving after upper-limb surgery guide for more details.
As the swelling settles, you will begin gentle movements guided by your physiotherapist. These exercises are crucial for restoring range of motion and strength. You will perform simple tasks at home, such as reaching for light objects, as tolerated. Sleep may be difficult at first; propping yourself up with pillows often helps. Your physiotherapist will adjust your routine as your healing progresses.
Recovery varies between individuals. Your timeline may differ based on your body’s response and the complexity of your tear. We focus on long-term durability, with many patients seeing significant improvement that lasts for years. Trust the process, follow our instructions, and communicate openly with your surgeon and physiotherapist about your progress.
What can go wrong¶
Most patients do well, but problems can occasionally happen. Your surgeon and the team monitor you closely to spot any issue early.
Healing is a long process. Improvement may feel slow after the first year. Some people notice their shoulder function does not keep getting better over time. This is normal for many. If you feel stuck, tell us at your next review. We can adjust your plan.
Re-tearing is a known risk. The highest chance of this happening is between six weeks and three months after surgery. You might feel a sudden pop or sharp pain. Your shoulder may feel weak or unstable. Call our clinic immediately if this happens. Early attention helps us manage it.
Surgery timing matters. Waiting three to six months before your operation is usually safe. However, waiting a year or more can increase the risk of re-tearing. If you are considering delaying, discuss this with us first. We want to protect your long-term results.
Infection is a serious concern. You might notice redness spreading from your small incisions. The area could feel hot, swollen, or very tender. You may have a fever or chills. These signs need urgent care. Go to the emergency department or call us right away.
Blood clots are rare but possible. You might feel swelling, pain, or tenderness in your calf or thigh. Your leg could look red or feel warm. This is a medical emergency. Seek immediate help if you notice these symptoms in your leg.
Revision surgery may be needed. If your first repair does not hold, a second operation might be necessary. You might feel persistent pain or limited movement. Re-tears in revision cases are often smaller than the original tear. We will discuss all options with you if this occurs.
The complications table on this page lists typical rates if you want the specifics.
When to call us¶
Call us if you develop a fever, increasing wound redness, or discharge. Go to emergency if you experience sudden severe pain, calf swelling, shortness of breath, loss of sensation, or inability to move your limb. These signs need urgent assessment. Do not wait for your next appointment if these symptoms appear. Contact our clinic immediately for guidance on your specific situation.
Evidence & references
Anatomy & Pathophysiology¶
- The rotator cuff is a complex of four muscles (subscapularis, supraspinatus, infraspinatus, and teres minor) that arise from the scapula and whose tendons blend with the subjacent capsule as they attach to the humeral tuberosities [9].
- The subscapularis arises from the anterior aspect of the scapula and attaches over much of the lesser tuberosity [9].
- The supraspinatus arises from the fossa superior to the scapular spine, passes beneath the acromion and acromioclavicular joint, and attaches to the superior aspect of the greater tuberosity [9].
- The infraspinatus arises from the fossa below the scapular spine and attaches to the posterolateral aspect of the greater tuberosity [9].
- The teres minor arises from the lower lateral aspect of the scapula and attaches to the lower portion of the greater tuberosity [9].
- The tendons of the rotator cuff blend together to form a continuous cuff around the humeral head [9].
- Histologic studies describe the rotator cuff tendons as having five distinct layers, including superficial coracohumeral ligament fibers, tendon fiber bundles, smaller tendon fascicles, loose connective tissue with thick collagen bands, and the superior joint capsule [9].
- There is significant overlap and interdigitation of the supraspinatus and infraspinatus tendons near the footprint on the greater tuberosity [9].
- The long head of the biceps tendon attaches to the supraglenoid tubercle, runs between the subscapularis and supraspinatus, exits through the bicipital groove, and may serve as a passive restraint contributing to anterior stability [9].
- The rotator cable is a thick bundle of fibers running perpendicular to the supraspinatus tendon fibers, connecting the supraspinatus and infraspinatus tendons [10].
- The hypovascular critical zone is located on the articular side of the rotator cuff close to the insertion on the greater tuberosity [10].
- The supraspinatus footprint measures 13 mm in width (medial-lateral) and 20 mm in depth (anterior-posterior) [10].
- The infraspinatus footprint measures 14 mm in width and 20 mm in superoinferior dimension [10].
- The rotator cuff functions to stabilize the head of the humerus by pulling it firmly into the glenoid whenever the deltoid lifts the arm [6].
- The coracoacromial arch, formed by the acromion, coracoid process, and coracoacromial ligament, arches over the rotator cuff [6].
- The subacromial bursa separates the rotator cuff tendons from the coracoacromial arch to allow gliding [6].
- The primary passive stabilizers of the glenohumeral joint are the capsule and scapulohumeral ligaments, which act as checkreins near the extremes of range of motion [13].
- The glenohumeral joint capsule is thickest in the inferior pouch at 2.8 mm, 2.4 mm in the anterior portion, and 2.2 mm in the posterior portion [13].
- The superior glenohumeral ligament (SGHL) crosses the rotator interval capsule and lies between the supraspinatus and subscapularis tendons [13].
- The coracohumeral ligament originates at the base of the coracoid, blends into the cuff tendons, and inserts into the greater and lesser tuberosities [13].
- The SGHL and coracohumeral ligament come under tension with glenohumular flexion, extension, external rotation, and adduction to resist posterior and inferior displacement of the humeral head [13].
- The middle glenohumeral ligament (MGHL) is tensioned by external rotation when the humerus is abducted to 45 degrees [13].
- The capsule and ligaments contribute to stability through proprioceptive functions [13].
- Rotator cuff pathology prevalence increases with age, with a consistent finding that increased age is associated with higher prevalence of rotator cuff pathology [22].
- Population-based studies show that one-quarter of patients above 60 years of age and half of patients above 80 years will have a rotator cuff tear [22].
- The prevalence of rotator cuff tears ranges from 13% for patients in their fifties to 50% for patients aged 80 years or older [24].
- Bilateral tears are common despite often unilateral symptoms [24].
- Risk factors for rotator cuff tear development include male sex, manual labor, and history of trauma [24].
- Intrinsic degeneration involves age-related changes in collagen, proteoglycan, water content, and vascularity (tendinosis), usually involving the supraspinatus and infraspinatus starting on the articular side [10].
- Extrinsic mechanisms involve chronic impingement on the coracoacromial arch, with tears usually starting on the bursal side and potentially associated with a hook-shaped acromion [10].
- Acute traumatic tears occur after a fall and/or dislocation of the shoulder, typically in patients under 40 years old [10].
- Symptoms of pain do not correlate with rotator cuff tear severity [3].
- The natural history of asymptomatic rotator cuff tears includes progression in tear size, with 53% increasing in size over time [3].
- Symptomatic progression of asymptomatic rotator cuff tears is linked to tear progression from partial to full thickness, worsening tear size, muscle atrophy, fatty infiltration development, and new biceps pathology [24].
- Symptoms in rotator cuff disease usually wax and wane periodically while a physiological decline occurs over time, resulting in eventual cuff tear arthropathy [24].
- Cuff tear arthropathy is the final stage of the shoulder impingement syndrome spectrum, affecting patients with long-term insufficient massive rotator cuff tears [14].
- Cuff tear arthropathy involves superior migration of the humeral head toward the acromion, subchondral osteoporosis, and humeral head collapse [14].
- Cuff tear arthropathy affects women more commonly than men with a 3:1 female to male ratio [14].
- Cuff tear arthropathy more commonly affects the dominant shoulder [14].
- Risk factors for cuff tear arthropathy include chronic rotator cuff tear, hemorrhagic shoulder (oral anticoagulants and hematologic diseases), rheumatic disease, and crystal-induced arthropathy [14].
- Pathogenesis of cuff tear arthropathy includes mechanical factors (insufficient cuff, superior migration, instability), nutritional factors (hypomobility-induced cartilage atrophy, poor nutrition), and crystalline-induced arthropathy [14].
- Calcific tendinitis typically affects patients aged 30 to 60 years and women more commonly than men [23].
- The supraspinatus tendon is the most often involved in calcific tendinitis [23].
- The pathogenesis of calcific tendinitis involves an active, cell-mediated process with three stages: precalcific, calcific, and postcalcific [23].
- The precalcific stage consists of predominantly fibrocartilaginous metaplasia within less vascular areas of the tendon [23].
- The resorption phase of calcific tendinitis involves an inflammatory response and is exquisitely painful [23].
- Calcific tendinitis is generally self-limited, with most cases resolving spontaneously [23].
- Genetic variations and inherited predisposition contribute to the risk for rotator cuff disease [14, 15].
- Genome-wide association studies have identified two significant single-nucleotide polymorphisms associated with full-thickness rotator cuff tears [3].
- The critical shoulder angle (CSA) is a static radiographic measure that is higher in patients with rotator cuff tears compared to asymptomatic individuals [12].
- A critical shoulder angle greater than 38° and an acromial index greater than 0.7 are associated with higher retear rates after arthroscopic rotator cuff repair [11].
- The critical shoulder angle does not influence 24-month functional outcome after arthroscopic rotator cuff repair [13].
- The critical shoulder angle does not change over time [12].
- Large critical shoulder angle is associated with higher risk of tendon retear after arthroscopic rotator cuff repair [11].
- Individual scapular anatomy, measured by the critical shoulder angle, shows statistically significant differences between asymptomatic individuals, those with osteoarthritis, and those with full-thickness rotator cuff tears [3].
- Fatty muscle degeneration in cuff ruptures can be evaluated by CT scan and is a factor associated with failure of rotator cuff repair [8].
- Factors known to be associated with failure of rotator cuff repair include muscle degeneration (fatty infiltration and atrophy), tear size, chronicity, advanced age, and environmental factors [8].
- Most rotator cuff tears result from tendon degeneration rather than impingement by the acromion [4].
- Acromioplasty is not a necessary part of surgical management for most rotator cuff tears [4].
- The preponderance of re-tears in chronic degenerative tears are from suture pullout through worn tendon [4].
- The rotator cuff presents special challenges for tendon healing because its tendons are intra-articular and intrasynovial [8].
- The native fibrocartilaginous insertion to the greater tuberosity is not reconstituted after repair [8].
- There is almost always an element of chronic tendinopathy leading to impaired biological healing capacity on both the tendon and bone side [8].
- Partial-thickness rotator cuff tears have a limited ability to spontaneously heal [5].
- A substantial portion of partial-thickness rotator cuff tears will progress in tear size, with up to 53% progressing in one study [5].
- Partial-thickness rotator cuff tears can progress to full-thickness rotator cuff tears [5].
- The prevalence of asymptomatic partial-thickness rotator cuff tears is 20% overall and increases to 26% in patients older than 60 years [5].
- Partial-thickness rotator cuff tears are classified as articular-sided, bursal-sided, or intratendinous [5].
- The Ellman classification grades partial-thickness tears as Grade 1 (≤3 mm), Grade 2 (3 to 6 mm), and Grade 3 (>6 mm) based on depth [5].
- Grade 3 tears represent tears of more than 50% of tendon width [5].
- Tears involving more than 50% of tendon width are generally best treated with repair, while those involving less than 50% are treated with debridement [5].
- A higher failure rate of debridement has been suggested for partial-thickness bursal-sided rotator cuff tears compared to articular-sided tears [5].
- Delamination-type tears of the articular side, common in overhead athletes, should be repaired using a transtendinous technique if delamination is present [5].
- Intratendinous tears identified on MRI must be localized preoperatively and repaired side-to-side using arthroscopic technique [5].
- Extensive debridement of intratendinous tears is unnecessary [5].
- The natural history of rotator cuff disease shows that symptoms improve over the first year after treatment but then plateau, representing a regression to the mean [2].
- The comfort and function of shoulders with failure of anatomic repair are not significantly different from those in which the repair attempt was successful [4].
- There is only limited evidence that rotator cuff repair is an option for patients with chronic, symptomatic full-thickness tears [4].
- There is only limited evidence that early surgical repair after acute rotator cuff tear improves outcomes [4].
- There is inconclusive evidence for or against a specific technique (arthroscopic, mini-open, or open repair) when surgery is indicated for full-thickness rotator cuff tears [4].
- Routine acromioplasty is not required at the time of rotator cuff repair [4].
- In patients older than 50 years with a degenerative rotator cuff tear, there is no difference in clinical effectiveness or cost-effectiveness between open repair and arthroscopic repair at 2 years [4].
- The rate of re-tear was not significantly different across randomized groups for open versus arthroscopic repair (46.4% for arthroscopic and 38.6% for open) [4].
- In patients older than 55 years with degenerative supraspinatus tears, there were no significantly or clinically important differences in pain, function, or satisfaction among physiotherapy alone, acromioplasty plus physiotherapy, and arthroscopic repair groups at 2 years [4].
- Arthroscopic repair and physiotherapy were significantly more expensive than physical therapy alone, resulting in less value for arthroscopic repair compared to physical therapy alone [4].
- The mean sagittal size of the tendon tear was slightly smaller (7 mm) in the repair group compared with no-repair groups at 2 years, but this did not translate to clinical benefit [4].
- The rotator cuff syndrome comprises supraspinatus impingement and tendinitis, tears of the rotator cuff, acute calcific tendinitis, and biceps tendinitis/rupture [6].
- Pain from rotator cuff disorders is typically over the front and lateral aspect of the shoulder with weakness on abduction for supraspinatus involvement [6].
- If the cuff or biceps has ruptured, there will be weakness [6].
- Night pain is typical of rotator cuff disease and is related to poor outcomes after nonsurgical treatment [10].
- A combination of age greater than 65 years, night pain, and weakness has 95% specificity for rotator cuff tears [10].
- The tangent sign corresponds with muscle atrophy and chronicity of rotator cuff tears [10].
- The Goutallier-Fuchs classification grades fatty atrophy on T1 sagittal MRI cuts from Grade 0 (normal) to Grade 4 (more fat than muscle) [10].
- Small full-thickness rotator cuff tears and painful partial-thickness tears become 25% to 50% larger within 3 to 4 years [10].
- Larger lesions progress faster than smaller lesions [10].
- Associated lesions with rotator cuff tears include acromioclavicular arthritis, proximal biceps tendinitis, and adhesive capsulitis [10].
- The prevalence of full-thickness rotator cuff tears is 7% to 40%, while partial-thickness tears are more common with 50% higher prevalence [10].
- Impingement-rotator cuff tears are a spectrum of disease starting with tendinitis (20 to 35 years), progressing to tendinosis (35 to 45 years), rotator cuff tears (>45 years), and cuff arthropathy (>65 years) [10].
- MRI is the benchmark for diagnosing rotator cuff tears with 94% sensitivity and 93% specificity [10].
- Intra-articular contrast-enhanced magnetic resonance arthrography is best for detecting partial-thickness rotator cuff tears with 95% sensitivity and 95% specificity [10].
- Ultrasonography has good accuracy (92% sensitivity and 93% specificity) but is operator dependent and has poor sensitivity for diagnosing partial-thickness rotator cuff tears [10].
- The critical shoulder angle is a static measure that does not change over time but is higher in patients with rotator cuff tears [12].
- Patients with a critical shoulder angle greater than 38° and an acromial index greater than 0.7 had higher retear rates but similar functional rates compared to controls [11].
- The critical shoulder angle and acromial index do not influence 24-month functional outcome after arthroscopic rotator cuff repair [13].
- The critical shoulder angle was determined to be a static measure that did not change over time in a study of 1,552 radiographs [12].
- Differences in critical shoulder angle between groups are small and depend on excellent radiographic technique [12].
- The rotator cable forms the middle portion of the ligament under the supraspinatus tendon and connects the supraspinatus and infraspinatus tendons [11].
- The anterior segment of the rotator cable forms the lateral part of the rotator interval [11].
- The posterior part of the rotator cable ends at the insertion region between the infraspinatus and teres minor tendons on the posterior side of the greater tuberosity [11].
- The coracohumeral ligament contributes fibers that envelope the supraspinatus tendon in the rotator interval [11].
- The rotator interval capsule creates a thicker region of the cuff visible on ultrasound [11].
- The rotator cuff tendons send fascicles into their neighbors, with complex sharing occurring at the bicipital groove [11].
- Fascicles of the subscapularis tendon create a floor for the bicipital groove by undergoing chondrometaplasia [11].
- Fascicles of the supraspinatus tendon destined for the subscapularis insertion cross over the bicipital groove to create a roof [11].
- The rotator cuff muscles attach to the capsule in their deeper regions [11].
- The most complex arrangement of muscle and tendon attachment to the capsule occurs at the rotator interval [11].
- The coracohumeral ligament and transverse humeral ligament keep the biceps tendon aligned in the groove [9].
- Electromyographic studies show the long head of the biceps may be inactive during shoulder movements but serves as a passive restraint [9].
- Changes in elbow position and loading of the biceps can lead to altered shoulder motion and muscle recruitment [9].
- The b
Classification¶
- Partial-thickness rotator cuff tears are common in the general population, with an increased incidence with increasing age [5].
- Sher et al. showed an overall prevalence of asymptomatic partial-thickness rotator cuff tears of 20% [5].
- The prevalence of asymptomatic partial-thickness rotator cuff tears increased to 26% in patients older than 60 years [5].
- Partial-thickness rotator cuff tears can be classified as articular-sided, bursal-sided, or intratendinous tears [5].
- Ellman described a classification of partial-thickness rotator cuff tears based on location and depth of tearing noted at the time of shoulder arthroscopy [5].
- Tears are classified as articular-sided (A), bursal-sided (B), or intratendinous (C) [5].
- Grade 1 tears involve 3 mm or less of tendon [5].
- Grade 2 tears involve 3 to 6 mm of tendon [5].
- Grade 3 tears involve more than 6 mm of tendon [5].
- Grade 3 tears represent tears of more than 50% of tendon width [5].
- With MRI evaluation, partial-thickness tears are classified as low grade if they involve less than 50% of the tendon width [5].
- With MRI evaluation, partial-thickness tears are classified as high grade if they involve more than 50% of the tendon width [5].
- Partial-thickness tears have a limited ability to spontaneously heal as shown by histological and radiographic studies [5].
- As many as 53% of partial-thickness rotator cuff tears will progress in tear size in one study [5].
- A portion of partial-thickness rotator cuff tears will progress to full-thickness rotator cuff tears [5].
- Most partial-thickness rotator cuff tears are best initially managed with nonoperative treatment [5].
- Surgical treatment with either rotator cuff repair or debridement is indicated for patients in whom nonoperative treatment fails [5].
- Most surgeons agree that tears involving more than 50% of tendon width are best treated with repair [5].
- Most surgeons agree that tears involving less than 50% of tendon width are best treated with debridement and potential decompression [5].
- Systematic reviews have shown that most patients can achieve good to excellent functional results with this treatment strategy [5].
- A higher failure rate of debridement has been suggested for partial-thickness bursal-sided rotator cuff tears compared to articular-sided rotator cuff tears [5].
- Some surgeons favor repair in even low-grade bursal-sided tears due to the higher failure rate of debridement [5].
- The decision for in situ rotator cuff repair or completion to a full-thickness rotator cuff tear with subsequent repair involves two techniques with no difference in functional outcome scores [5].
- The decision for in situ rotator cuff repair or completion to a full-thickness rotator cuff tear with subsequent repair involves two techniques with no difference in re-tear rates [5].
- Generally, the choice between in situ repair and completion to full-thickness repair depends on the proportion and quality of the intact tendon [5].
- For tears with poor-quality tendon remaining and involving more than 80% of tendon thickness, debridement is favored [5].
- Delamination-type tears of the articular side commonly occur in athletes involved in throwing and in sports requiring overhead motion [5].
- If delamination of the tear is present, a transtendinous repair is indicated [5].
- Intratendinous tears that can be identified on MRI must be localized through preoperative planning and use of a spinal needle to identify the tear site [5].
- The tear can be opened using an arthroscopic knife and the edge debrided back slightly to promote local healing [5].
- Goodmurphy et al. showed that extensive debridement is unnecessary for intratendinous tears [5].
- Intratendinous tears are repaired side-to-side using arthroscopic technique [5].
Clinical Presentation¶
- Clinical decision-making for the management of rotator cuff tears lacks consensus among orthopedic surgeons [1].
- Patients with rotator cuff tears can be divided into three categories: those needing urgent or early operative repair, those benefiting from a trial of conservative treatment, and those best suited for nonoperative treatment [1].
- The most common causes of pain around the shoulder are disorders of the rotator cuff, chiefly rotator cuff syndrome, calcific tendinitis, and adhesive capsulitis [6].
- The rotator cuff is composed of the subscapularis, supraspinatus, infraspinatus, and teres minor muscles [6].
- The rotator cuff stabilizes the head of the humerus by pulling it firmly into the glenoid whenever the deltoid lifts the arm [6].
- The coracoacromial arch is formed by the acromion process, coracoid process, and coracoacromial ligament [6].
- Rotator cuff syndrome comprises supraspinatus impingement and tendinitis, tears of the rotator cuff, acute calcific tendinitis, and biceps tendinitis and/or rupture [6].
- Patients with rotator cuff disorders typically complain of pain over the front and lateral aspect of the shoulder [6].
- Weakness on abduction is associated with supraspinatus involvement, tears of the cuff, and tendinitis [6].
- Pain over the front of the shoulder is associated with biceps pathology [6].
- Rupture of the cuff or biceps results in weakness [6].
- Patients with acute rotator cuff tears may present with a clear history of trauma resulting in acute pain and weakness [25].
- Patients with chronic rotator cuff disease often describe an insidious onset of lateral and/or anterior shoulder pain associated with overhead activities [25].
- Night pain is a common presenting symptom of rotator cuff disease [25].
- A family or personal history of rotator cuff disease makes the diagnosis more likely [25].
- Basic physical examination for rotator cuff tears includes assessment of range of motion, strength, and associated structures such as the biceps and acromioclavicular joint [25].
- The empty can test has a sensitivity of 71.7% and a specificity of 64.6% for full-thickness supraspinatus tears [25].
- The lift-off and belly-press tests have high specificity but low sensitivity for full-thickness subscapularis tears [25].
- Patients with an external rotation lag sign at the side likely have a large posterosuperior tear involving the infraspinatus [25].
- A positive hornblower sign suggests a massive posterosuperior cuff tear that prohibits the active positioning of the hand in space [25].
- The painful arc test has a sensitivity of 71% and specificity of 81% for rotator cuff disease [25].
- The cross-body adduction test has a sensitivity of 75% and specificity of 61% for rotator cuff disease [25].
- The Hawkins test has a sensitivity of 76% and specificity of 48% for rotator cuff disease [25].
- The Neer test has a sensitivity ranging from 64% to 68% and specificity ranging from 30% to 61% for rotator cuff disease [25].
- The Yocum test has a sensitivity of 79% and specificity of 40% for rotator cuff disease [25].
- Passive abduction has a sensitivity of 74% and specificity of 10% for rotator cuff disease [25].
- The external rotation lag sign has a sensitivity of 47% and specificity of 94% for full-thickness rotator cuff tears [25].
- The internal rotation lag sign has a sensitivity of 97% and specificity of 83% for full-thickness rotator cuff tears [25].
- The drop arm test has a sensitivity of 24% and specificity of 93% for rotator cuff disease [25].
- The dropping sign has a sensitivity of 73% and specificity of 77% for full-thickness rotator cuff tears [25].
- The Gerber (lift-off test) has a sensitivity ranging from 34% to 68% and specificity ranging from 50% to 77% for rotator cuff disease [25].
- External rotation resistance has a sensitivity of 63% and specificity of 75% for rotator cuff disease [25].
- The full can test has a sensitivity of 75% and specificity of 68% for rotator cuff disease [25].
- The Patte test has a sensitivity of 58% and specificity of 60% for rotator cuff disease [25].
- The empty can (Jobe) test has a sensitivity of 71% and specificity of 49% for rotator cuff disease [25].
- Resisted abduction has a sensitivity of 58% and specificity of 20% for rotator cuff disease [25].
- When both the Hawkins and Neer tests are positive, the sensitivity is 78% and specificity is 50% for rotator cuff disease [25].
- Ultrasonography approaches the sensitivity and specificity of MRI for detecting full-thickness rotator cuff tears with an experienced practitioner [25].
- MRI accurately assesses muscle, bone, and cartilage and is the imaging modality of choice for most providers [25].
- Patients with rotator cuff tears are usually aged over 45 and give a history of refractory shoulder pain with increasing stiffness and weakness [26].
- Partial tears may occur within the substance or on the deep surface of the cuff [26].
- In partial tears, the remaining cuff fibers permit active abduction with a painful arc [26].
- A full-thickness tear may follow a long period of chronic tendinitis or occur spontaneously after a sprain or jerking injury [26].
- In full-thickness tears, patients experience sudden pain and are unable to abduct the arm [26].
- If active abduction is possible after subacromial local anesthetic injection, the tear is likely partial; if active abduction remains impossible, a complete tear is likely [26].
- With time in full-thickness tears, there may be some recovery of active abduction, though power in abduction and external rotation remains weaker than normal [26].
- Long-standing partial or complete ruptures are associated with wasting of the supraspinatus and infraspinatus [26].
- Testing the biceps in long-standing ruptures may reveal an old tear of the long head of the biceps tendon [26].
- There is often tenderness of the acromioclavicular joint in rotator cuff tears [26].
- In long-standing cases of partial or complete rupture, secondary osteoarthritis of the shoulder may supervene with severely restricted movements [26].
- In a study of 24 patients refusing operative treatment for full-thickness supraspinatus tears, 33% had an increase in tear size at 3.5 years [27].
- In a study of 24 patients refusing operative treatment for full-thickness supraspinatus tears, 17% had no change in tear size at 3.5 years [27].
- In a cohort of 59 full and partial-thickness tears followed for at least 18 months, 48% showed progression of tear size [27].
- In a cohort of 59 full and partial-thickness tears followed for less than 18 months, 19% showed progression of tear size [27].
- Full-thickness tears are more likely to progress than partial-thickness tears [27].
- Progression of rotator cuff tears occurs in 54% of patients over the age of 60 years versus 17% in patients under 60 years [27].
- In a cohort of patients under 60 years treated nonoperatively for full-thickness rotator cuff tears, 49% of tears increased in size [27].
- Pain and duration of symptoms are not associated with the severity of rotator cuff tears in a multicenter cohort of over 400 patients [27].
- Nonoperative treatment of full-thickness rotator cuff tears is effective in 75% of patients after 2 years [27].
- A patient's perception that physical therapy would be beneficial is a strong predictor of successful conservative treatment [27].
- Tears involving the anterior portion of the supraspinatus are associated with significantly greater rates of fatty infiltration of the supraspinatus and infraspinatus [27].
- Tears not involving but close to the rotator cable may need to be more closely monitored if treated nonoperatively [27].
- Larger, symptomatic tears involving the infraspinatus are associated with increased superior migration of the humeral head compared to asymptomatic, smaller tears [27].
- A critical tear area of 175 mm², correlating to dimensions of approximately 15 mm × 12 mm, is associated with proximal humeral migration [27].
- In a longitudinal study of asymptomatic shoulders, 36% of tears developed symptoms over time [27].
- An increase in tear size in asymptomatic shoulders is associated with the development of symptoms [27].
- Asymptomatic tears that became symptomatic significantly increased in size, while those that did not become symptomatic did not increase in size [27].
- Approximately 50% of asymptomatic tears have a significant increase in size at a median time of 2.8 years [27].
- Full-thickness tears are more likely to enlarge, become painful, and progress to muscle degeneration compared with partial-thickness tears [27].
- Degenerative rotator cuff tears initiate approximately 13 to 17 mm posterior to the long head of the biceps tendon [30].
- The area 15 mm posterior to the biceps tendon correlates to the posterior supraspinatus and anterior infraspinatus [30].
- Significant interdigitation of the supraspinatus and infraspinatus fibers exists in the region 15 mm posterior to the biceps tendon [30].
- The area of tear initiation is within the "rotator crescent" tissue described by Burkhart et al. [30].
- The rotator crescent is thinner and more avascular than the rotator cable [30].
- Ultrasound data suggest that degenerative rotator cuff tears initiate in the middle of the crescent tissue and propagate in both directions [30].
- Propagation or involvement of the anterior cable of the rotator cuff has a significant impact on the rate of irreversible muscle degeneration [30].
- Loss of integrity of the anterior supraspinatus tissue may lead to accelerated retraction and degeneration of muscle tissue associated with lower rates of tendon healing [30].
- Patte Group I includes partial tears and full-substance tears measuring less than 1 cm in sagittal diameter at bony detachment [31].
- Group I lesions rarely exhibit an operative indication [31].
- Physiotherapy aiming to eliminate subacromial impingement usually results in satisfactory pain relief for Group I lesions [31].
- Group II includes full-substance tears of the entire supraspinatus with a sagittal diameter of approximately 2 cm [31].
- In Group II, the infraspinatus is intact, although an intrasubstance tear secondary to interstitial necrosis is usually present in the posterior aspect [31].
- Group III includes full-substance tears involving more than one tendon with a sagittal extent of 4 cm or more [31].
- Group III defects are serious and demand early surgical treatment [31].
- Group IV lesions are characterized by massive tears and secondary osteoarthritic changes in the humeral head [31].
- Group IV lesions often limit the possibility of repair, making arthroplasty necessary [31].
- Distally situated deep tears are the most commonly observed lesion during surgery and are characterized by detachment at the fibrocartilaginous zone [31].
- Trauma preceded 62% of distally situated deep tears [31].
- Partial tears at the critical zone can be diagnosed by arthrography [31].
- Partial superficial tears cannot be detected by arthrography and are diagnosed by bursoscopy or at the time of surgery [31].
- Partial superficial tears have a good prognosis due to adequate blood supply [31].
- Painful long head of the biceps tendon (LHBT) tendinitis may ensue from tears about the rotator interval or chronic inflammatory pathology of the glenohumeral joint [32].
- Clinical tests for LHBT pathology including O'Brien, Yergason, Speed, and direct palpation have limited specificity [32].
- Isolated traumatic LHBT tears are generally treated nonsurgically [32].
- Arthroscopic tenotomy for LHBT pathology results in cosmetic deformity (Popeye) about 30% of the time [32].
- Vigorous activity after LHBT tenotomy may result in cramping pain of the biceps muscle belly [32].
- Arthroscopic suprapectoral tenodesis may be performed for SLAP tears or in conjunction with rotator cuff repair for patients needing full supination strength and endurance [32].
- Sutures through bone tunnels have more cyclic displacement than anchors, keyhole, screw, or button techniques for biceps fixation [32].
- There is no evidence that substantiates one biceps fixation approach or method over another [32].
Investigations¶
- The overall prevalence of full-thickness rotator cuff tears is approximately 25% in patients over 60 years of age [17].
- The prevalence of full-thickness rotator cuff tears increases to 50% in patients over 80 years of age [17].
- Patients with a symptomatic full-thickness rotator cuff tear in one shoulder have a 50% chance of an asymptomatic full-thickness rotator cuff tear in the contralateral shoulder [17].
- MRI allows the surgeon to characterize the location, size, and amount of retraction of a rotator cuff tear [17].
- MRI allows the surgeon to evaluate the degree of atrophy and fatty infiltration of the rotator cuff musculature [17].
- The Goutallier classification for fatty infiltration grade 0 indicates normal muscle [17].
- The Goutallier classification for fatty infiltration grade 1 indicates some fatty streaks [17].
- The Goutallier classification for fatty infiltration grade 2 indicates more muscle than fat [17].
- The Goutallier classification for fatty infiltration grade 3 indicates equal amounts of muscle and fat [17].
- The Goutallier classification for fatty infiltration grade 4 indicates more fat than muscle [17].
- Goutallier grades 3 and 4 are indications of a long-term chronic rotator cuff tear [17].
- Goutallier grades 3 and 4 have a higher potential for failure when surgery is undertaken [17].
- Goutallier grades 3 and 4 are likely deemed irreparable [17].
- The presence of a tendon stump attached to the greater tuberosity decreases the length of tendon available for repair [17].
- An MRI is indicated in younger, active patients with acute rotator cuff tears [17].
- An MRI is indicated in patients with chronic rotator cuff tears in whom a trial of nonoperative treatment has failed [17].
- Nonoperative treatment leads to a successful outcome in 60% of patients with full-thickness tears [17].
- The risk of tear progression with nonoperative treatment is approximately 50% at 2 years [17].
- With long-standing rotator cuff tears, the size, retraction, and degree of fatty infiltration can increase [17].
- Increased size, retraction, and fatty infiltration can compromise the structural integrity and functional outcomes after rotator cuff repair [17].
- Rotator cuff repair is indicated for patients with acute, full-thickness rotator cuff tears [17].
- Rotator cuff repair is indicated for patients with chronic, full-thickness rotator cuff tears after failure of nonoperative treatment [17].
- Repair of acute rotator cuff tears generally should be performed within 3 months of injury [17].
- Inferior outcomes are reported after repair done more than 4 months after injury [17].
- Factors associated with failure after rotator cuff repair include larger tears [17].
- Factors associated with failure after rotator cuff repair include greater retraction [17].
- Factors associated with failure after rotator cuff repair include advanced Goutallier grade [17].
- Factors associated with failure after rotator cuff repair include older age [17].
- Factors associated with failure after rotator cuff repair include smoking status [17].
- Factors associated with failure after rotator cuff repair include osteoporosis [17].
- Factors associated with failure after rotator cuff repair include diabetes mellitus [17].
- Factors associated with failure after rotator cuff repair include hypercholesterolemia [17].
- Factors associated with failure after rotator cuff repair include more aggressive rehabilitation protocols [17].
- The best potential for healing is in patients younger than 70 years with acute, small tears (<3 cm) and a healthy tendon-bone interface [17].
- Patients with Goutallier grades III and IV tears, if accompanied by a tendinous stump of less than 15 mm and a positive tangent sign, have a 90% failure rate [17].
- Tears with Goutallier grades III and IV are usually deemed irreparable [17].
- Irreparable tears are treated with alternative strategies such as debridement, tendon transfer, superior capsular reconstruction, or reverse shoulder arthroplasty [17].
- Intraoperative prognostic healing factors include tendon and bone quality [17].
- Intraoperative prognostic healing factors include the ability to anatomically reduce and repair the tendon to its normal footprint on the tuberosity without undue tension [17].
- If anatomic repair cannot be achieved without significant tension, a medialised repair can be performed [17].
- Strong fixation of the repair is essential to prevent gapping of the tendon [17].
- Ultrasonography is more accurate for full-thickness rotator cuff tears and is comparable to MRI [22].
- Ultrasonography is increasing in popularity as a tool for diagnosis of rotator cuff disease [18].
- Ultrasonography is used for confirmation of intraarticular or subacromial location of injections [18].
- MRI is used to define the extent of tear, degree of tear retraction, and presence of muscular atrophy [18].
- MRI is key for evaluating fatty infiltration [18].
- The tangent sign is defined as failure of the supraspinatus muscle belly to cross a line from the superior border of the coracoid to the superior border of the scapular spine [18].
- The tangent sign correlates with muscle atrophy and fatty infiltration of the supraspinatus [18].
- Patients with the presence of a tangent sign are more likely to have an irreparable rotator cuff tear [18].
- Larger, more retracted tears (>40 mm length/width) are characterized by fatty atrophy [18].
- Larger, more retracted tears are characterized by supraspinatus width of less than 5 mm at the glenoid margin [18].
- Irreparable tears are more likely to occur when the acromiohumeral distance appears shorter (<7 mm) on AP radiograph [18].
- Radiographic views of the subacromial space such as the supraspinatus outlet view may show a spur on the undersurface of the acromion [16].
- Radiographic views may show narrowing of the subacromial space [16].
- With chronic rotator cuff disease, superior migration of the humeral head with extensive degenerative change may be present [18].
- MRI can demonstrate classic changes within the acromion or coracoacromial ligament including spurring and calcification [18].
- MRI can demonstrate cystic changes within the greater tuberosity [18].
- A positive tangent sign predicts the repairability of rotator cuff tears [21].
- Symptoms of pain do not correlate with rotator cuff tear severity [3].
- Patient-reported outcomes and pain are not correlated with rotator cuff healing on ultrasonography or MRI [20].
- Postoperative strength is better in individuals with healed rotator cuffs versus those with defects after repair [20].
- Patients with CSA greater than 38° and AI greater than 0.7 had higher retear rates but similar functional rates compared to control patients [11].
- CSA was higher in the patient group with rotator cuff tears but was a static measure that did not change over time [12].
- Differences in CSA depend on excellent radiographic technique [12].
- Critical shoulder angle and acromial index do not influence 24-month functional outcome after arthroscopic rotator cuff repair [13].
- Evidence of genetic variations associated with rotator cuff disease exists [14].
- There is evidence for an inherited predisposition contributing to the risk for rotator cuff disease [15].
- A genome-wide association study identified two significant single-nucleotide polymorphisms associated with full-thickness rotator cuff tears [3].
- There is a statistically significant difference in the critical shoulder angle between asymptomatic individuals, those with osteoarthritis, and patients with full-thickness rotator cuff tears [3].
- 53% of patients with full or partial rotator cuff tears increased in tear size over a minimum 6-month follow-up [3].
- Tear progression correlated with presenting tear size [3].
- The natural history of asymptomatic rotator cuff tears shows that symptoms improved over the first year after treatment but then plateaued, representing a regression to the mean [7].
- Regardless of treatment, symptoms improved over the first year after treatment for full-thickness rotator cuff tears [7].
- The timing of elective shoulder surgery after shoulder injection affects postoperative infection risk in Medicare patients [24].
- Current recommendations include avoiding steroid injection within 6 months prior to rotator cuff repair to decrease likelihood of failure rates [18].
- The rate-limiting step for recovery after rotator cuff repair is biologic healing of the rotator cuff tendon to the humerus, estimated to require a minimum of 8 to 12 weeks [18].
- Blood flow to the repaired rotator cuff is achieved from the peribursal tissue and bone anchor site [18].
- Vascularity of the repaired rotator cuff has been shown to increase with exercise [18].
- Ultrasonography is used for diagnosis of rotator cuff disease and confirmation of intraarticular or subacromial location of injections [19].
- MRI is used to define the extent of tear, degree of tear retraction, and presence of muscular atrophy [19].
- MRI is key for evaluating fatty infiltration [19].
- The tangent sign is defined as failure of the supraspinatus muscle belly to cross a line from the superior border of the coracoid to the superior border of the scapular spine [19].
- The tangent sign correlates with muscle atrophy and fatty infiltration of the supraspinatus [19].
- Patients with the presence of a tangent sign are more likely to have an irreparable rotator cuff tear [19].
- Larger, more retracted tears (>40 mm length/width) are characterized by fatty atrophy [19].
- Larger, more retracted tears are characterized by supraspinatus width of less than 5 mm at the glenoid margin [19].
- Irreparable tears are more likely to occur when the acromiohumeral distance appears shorter (<7 mm) on AP radiograph [19].
- MRI can demonstrate classic changes within the acromion or coracoacromial ligament including spurring and calcification [19].
- MRI can demonstrate cystic changes within the greater tuberosity [19].
- With chronic rotator cuff disease, superior migration of the humeral head with extensive degenerative change may be present [19].
Treatment¶
- Clinical decision-making for the management of rotator cuff tears lacks consensus among orthopedic surgeons [1].
- Patients requiring management of rotator cuff tears can be divided into three categories: those needing urgent or early operative repair, those benefiting from a trial of conservative treatment, and those best suited for nonoperative treatment [1].
- Most rotator cuff tears result from tendon degeneration rather than impingement by the acromion [4].
- Acromioplasty is not a necessary part of surgical management for most rotator cuff tears [4].
- Many rotator cuff tears can be successfully managed without surgery [4].
- Rates of clinical improvement and anatomically durable repairs have not noticeably improved despite an exponential increase in publications on arthroscopic management [4].
- The comfort and function of shoulders with failure of anatomic repair are not significantly different from those with successful repair attempts [4].
- There is only limited evidence that rotator cuff repair is an option for patients with chronic, symptomatic full-thickness tears [4].
- There is only limited evidence that early surgical repair after acute rotator cuff tear is beneficial [4].
- There is inconclusive evidence for or against a specific technique (arthroscopic, mini-open, or open repair) when surgery is indicated for full-thickness rotator cuff tears [4].
- Routine acromioplasty is not required at the time of rotator cuff repair, a recommendation with moderate support [4].
- The quality of the cuff tissue and patient characteristics are more dependent on the outcome of cuff surgery than the specific repair method used (single row, double row, TOE, or marginal convergence) [4].
- In patients older than 50 years with a degenerative rotator cuff tear, there is no difference in clinical effectiveness or cost-effectiveness between open repair and arthroscopic repair at 2 years [4].
- The rate of re-tear was not significantly different between arthroscopic (46.4%) and open (38.6%) surgery in patients older than 50 years with degenerative rotator cuff tears [4].
- In patients older than 55 years with degenerative supraspinatus rotator cuff tears, there were no significantly or clinically important differences in Constant score, VAS for pain, or patient satisfaction among groups treated with physiotherapy only, acromioplasty plus physiotherapy, or arthroscopic rotator cuff repair with acromioplasty and physiotherapy at 2 years [4].
- The mean sagittal size of the tendon tear was slightly smaller (7 mm) in the repair group compared to no-repair groups at 2 years, but this did not translate to clinical benefit [4].
- Arthroscopic repair and physiotherapy were significantly more expensive than physical therapy alone, resulting in less value for arthroscopic repair [4].
- Partial-thickness rotator cuff tears have an overall prevalence of 20% in the general population, increasing to 26% in patients older than 60 years [5].
- Partial-thickness rotator cuff tears are classified as articular-sided, bursal-sided, or intratendinous [5].
- The Ellman classification grades partial-thickness tears as Grade 1 (3 mm or less), Grade 2 (3 to 6 mm), and Grade 3 (more than 6 mm) based on depth [5].
- Grade 3 tears represent tears of more than 50% of tendon width [5].
- Partial-thickness tears have a limited ability to spontaneously heal [5].
- As many as 53% of partial-thickness rotator cuff tears will progress in tear size [5].
- Most partial-thickness rotator cuff tears are best initially managed with nonoperative treatment [5].
- Surgical treatment with rotator cuff repair or debridement is indicated for patients in whom nonoperative treatment fails [5].
- Tears involving more than 50% of tendon width are best treated with repair [5].
- Tears involving less than 50% of tendon width are best treated with debridement and potential decompression [5].
- A higher failure rate of debridement has been suggested for partial-thickness bursal-sided rotator cuff tears compared to articular-sided tears [5].
- For tears with poor-quality tendon remaining and involving more than 80% of tendon thickness, debridement is favored over in situ repair [5].
- Delamination-type tears of the articular side should be repaired using a transtendinous repair technique [5].
- Intratendinous tears can be repaired side-to-side using an arthroscopic technique after the tear is opened and edges are debrided slightly [5].
- Extensive debridement is unnecessary for intratendinous tears [5].
- Results of rotator cuff repair without decompression are not as good as results using the combined procedure of repair and acromioplasty [7].
- A proximal biceps tendon release or tenodesis is indicated if biceps pathology is present during open rotator cuff repair [7].
- Most rotator cuff tears begin at the supraspinatus insertion and have both transverse and longitudinal components [7].
- In tears of more than 2 to 3 cm, the infraspinatus tendon is involved [7].
- Mobilization of the rotator cuff should not dissect below the level of the teres minor to avoid injury to the axillary nerve or suprascapular nerve [7].
- If adequate length cannot be obtained with tendon mobilization, the capsule can be incised at its insertion into the glenoid labrum from the 8-o'clock to 4-o'clock position posteriorly [7].
- The goals of mobilization include obtaining tissue of adequate strength, positioning it anatomically without damage to innervation or deltoid function, and decompressing the subacromial space [7].
- The best results are obtained with the double-row technique, suturing the tendon to bone in a cancellous trough in combination with suture anchor fixation [7].
- Using transosseous tunnels through the greater tuberosity increases the surface area of tendon-to-bone healing and more closely restores the anatomic footprint [7].
- Sutures should be placed 5 to 10 mm from the free edge of the tear in a horizontal mattress manner [7].
- A 3 mm wide shallow trough should be created running the length of the exposed bone of the greater tuberosity [7].
- Suture anchors should be placed two or three immediately medial to the trough at a 45-degree angle [7].
- Holes for sutures should be drilled 2 to 3 cm distal to the trough [7].
- Suture holes should be spaced at least 1 to 2 cm apart on the cortical humeral surface [7].
- Sutures from anchors should be tied down on top of the tendon with four or five knots [7].
- Most repairs are done with the shoulder in 0 degrees of abduction [7].
- If the lateral humeral cortex is fractured during repair, anchors can be used as a salvage procedure [7].
- Symptomatic rotator cuff injuries affect up to 30% of the population [8].
- Among the aging population, the prevalence of full-thickness tears is estimated to be as high as 30% [8].
- Factors associated with failure of rotator cuff repair include muscle degeneration (fatty infiltration and atrophy), tear size, chronicity, advanced age, and environmental factors [8].
- Treatment of rotator cuff tears begins with nonsurgical measures including activity modification, physical therapy, nonsteroidal anti-inflammatory medications, and corticosteroid injection [8].
- When repair is indicated, approaches include traditional open repairs, mini-open deltoid split approaches, and arthroscopic repair [8].
- The current standard of care is arthroscopic repair [8].
- Arthroscopic repair has been shown to have similar outcomes and failure rates to open or mini-open repair, with decreased short-term pain and more rapid return to activity [8].
- The rotator cuff tends to fail at or near the tendon-bone junction [8].
- Controlled laboratory studies have generally shown superiority of double-row techniques over single-row in terms of initial and ultimate failure strength, decreased gap formation, decreased strain and suture cut-through, and improved vascularity [8].
- Arthroscopic surgery is the preferred method of rotator cuff repair for many shoulder surgeons due to advantages over traditional open repair [28].
- Arthroscopy facilitates more thorough visualization, diagnosis, and treatment of lesions within the joint [28].
- A high prevalence of concomitant intra-articular pathology has been reported in patients undergoing rotator cuff repair [28].
- Tendon mobilization is facilitated by precise releases of adhesions during arthroscopic repair [28].
- Injury to the deltoid muscle is minimized with arthroscopic repair [28].
- The acromial deltoid origin is preserved during arthroscopic repair, eliminating the risk of deltoid dehiscence [28].
- Arthroscopic repair offers decreased postoperative pain secondary to less soft tissue trauma [28].
- Anatomic footprint restoration is now possible with arthroscopic repair using fixation at both the suture-tendon interface and the anchor-bone interface [28].
- Historically, arthroscopic repair was performed using a single row of bone anchors placed within the tuberosity [28].
- The double-row technique involves two rows of suture anchors, one medially and one laterally, allowing for additional points of fixation and better coverage of the footprint area [28].
- Newer techniques involve a medial row of suture anchors with suture strands passed medially to a lateral row of anchors to compress the tendon down to the bone [28].
- Biomechanical studies show that double-row repair outperforms single-row repair in failure strength [28].
- Superior clinical results with double-row fixation over single-row fixation are still controversial [28].
- Mini-open rotator cuff repair allows direct assessment of the nature of the cuff tear and the quality of the remaining tissue [33].
- The transosseous technique for attachment of the tendon to the tuberosity is simple, expeditious, and avoids issues related to suture anchors [33].
- The creation of a trough into which the tendon is inserted increases the surface area of the repair, stimulates local stem cells and growth factors, excludes joint fluid from the repair site, and places sutures laterally [33].
- Surgery for mini-open rotator cuff repair begins with an inspection of the cuff through a deltoid-on approach [33].
- The deltoid is split longitudinally for 3 to 4 cm distal to the acromion in line with its fibers, leaving some tendon on each side of the split [33].
- Hypertrophic bursa and scar tissue are resected to allow a good view of cuff tendon involvement, tendon quality, and tendon tissue loss [33].
- The undersurface of the coracoacromial arch is palpated to detect roughness, which can be smoothed with a pinecone bur [33].
- It is essential to preserve the integrity of the coracoacromial arch [33].
- The goal of repair is strong fixation of the tendon to the humerus under normal tension with the arm at the side while leaving a smooth surface on the proximal humeral concavity [33].
- The desired attachment site is at the sulcus near the base of the tuberosity [33].
- Three stages of sequential release are required because the cuff is usually retracted and tissue is lost in chronic cuff disease [33].
- Unless releases are carried out, increased tension in the repaired tendon will predispose to tightness of the glenohumeral joint and challenge the repair site [33].
Complications¶
- Clinical decision-making for the management of rotator cuff tears lacks consensus among orthopedic surgeons [1].
- There is only limited evidence that rotator cuff repair is an option for patients with chronic, symptomatic full-thickness tears [4].
- There is only limited evidence that early surgical repair after acute rotator cuff tear is beneficial [4].
- Evidence for or against a specific technique (arthroscopic, mini-open, or open repair) when surgery is indicated for full-thickness rotator cuff tears is inconclusive [4].
- Routine acromioplasty is not required at the time of rotator cuff repair [4].
- The rate of clinical improvement and the rates of anatomically durable repairs have not noticeably improved despite an exponential rise in publications on arthroscopic management methods [4].
- The comfort and function of shoulders with failure of anatomic repair are not significantly different from those in which the repair attempt was successful [4].
- Preponderance of re-tears in rotator cuff repairs result from suture pullout through worn tendon rather than failure at the anchor-bone or suture-anchor interfaces [4].
- In patients older than 50 years with a degenerative rotator cuff tear, there is no difference in clinical effectiveness or cost-effectiveness between open repair and arthroscopic repair at 2 years [4].
- The rate of re-tear was 46.4% for arthroscopic repair and 38.6% for open surgery in patients older than 50 years with degenerative rotator cuff tears [4].
- In patients older than 55 years with degenerative supraspinatus rotator cuff tears, there were no significantly or clinically important differences in Constant score, VAS for pain, or patient satisfaction among groups treated with physiotherapy only, acromioplasty plus physiotherapy, or arthroscopic rotator cuff repair with acromioplasty and physiotherapy [4].
- At 2 years in patients older than 55 years with degenerative supraspinatus rotator cuff tears, the mean sagittal size of the tendon tear was slightly (7 mm) smaller in the repair group compared to no-repair groups [4].
- Arthroscopic repair and physiotherapy were significantly more expensive than physical therapy alone in patients older than 55 years with degenerative supraspinatus rotator cuff tears [4].
- The value (clinical benefit/cost) of arthroscopic repair was less than physical therapy alone in patients older than 55 years with degenerative supraspinatus rotator cuff tears [4].
References¶
[1] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > Indications for Rotator Cuff Repair. [2] Orthopaedic Knowledge Update Sports Medicine 6. Rotator Cuff Disease > Annotated References. [3] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Annotated References. [4] Rockwood And Matsen S The Shoulder. Arthroscopic Management of Prearthritic and Arthritic Conditions of the Shoulder and the Postarthroplasty Shoulder > Instability > Rotator Cuff. [5] Campbell S Operative Orthopaedics 4 Volume Set. ARTHROSCOPIC REPAIR OF POSTERIOR HUMERAL AVULSION OF THE GLENOHUMERAL LIGAMENT > PARTIAL-THICKNESS ROTATOR CUFF TEARS. [6] Apley And Solomon S Concise System Of Orthopaedics And Trauma. DISORDERS OF THE ROTATOR CUFF. [7] Campbell S Operative Orthopaedics 4 Volume Set. ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION WITH BONE-PATELLAR TENDON-BONE GRAFT > OPEN REPAIR OF ROTATOR CUFF TEARS > TECHNIQUE 46.2. [8] Orthopaedic Basic Science Fifth Edition Print Ebook. Lumbar Spondylosis, Degenerative Disk Disease, and Radiculopathy > Clinical Example: Rotator Cuff Repair. [9] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > RELEVANT SHOULDER ANATOMY > Rotator Cuff. [10] Aaos Comprehensive Orthopaedic Review 3. Rotator Cuff Tears and Cuff Tear Arthropathy > I. Rotator Cuff Tears. [11] Rockwood And Matsen S The Shoulder. Developmental Anatomy of the Shoulder and Anatomy of the Glenohumeral Joint > Rotator Cuff. [12] Classifications And Scores Of The Shoulder. THE WESTERN ONTARIO ROTATOR CUFF INDEX (WORC). [13] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > Rotator Cuff > Scapulohumeral Ligaments. [14] Aaos Comprehensive Orthopaedic Review 3. Rotator Cuff Tears and Cuff Tear Arthropathy > II. Cuff Tear Arthropathy. [15] Campbell S Operative Orthopaedics 4 Volume Set. ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION WITH BONE-PATELLAR TENDON-BONE GRAFT > DECOMPRESSION AND DEBRIDEMENT OF MASSIVE ROTATOR CUFF TEARS. [16] A Lange Medical Book Current Diagnosis Treatment In Orthopedics Fifth Edition. 3Sports Medicine > 1. Subacromial Bursitis and Rotator Cuff Tendinosis. [17] Campbell S Operative Orthopaedics 4 Volume Set. ARTHROSCOPIC REPAIR OF POSTERIOR HUMERAL AVULSION OF THE GLENOHUMERAL LIGAMENT > FULL-THICKNESS ROTATOR CUFF TEARS. [18] Miller S Review Of Orthopaedics. ROTATOR CUFF DISEASE > 4. Imaging. [19] Miller S Review Of Orthopaedics. SECTION 16 PATELLAR TRACKING IN TOTAL KNEE ARTHROPLASTY > ROTATOR CUFF DISEASE > 4. Imaging. [20] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Summary. [21] Orthopaedic Knowledge Update Sports Medicine 6. Current Concepts in Rehabilitation of Rotator Cuff Pathology: Nonsurgical and Postoperative Considerations > Exercise to Treat Rotator Cuff Pathology > Scapulothoracic Exercises. [22] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > NATURAL HISTORY OF ROTATOR CUFF PATHOLOGY AND IMPLICATIONS ON SURGICAL INDICATIONS. [23] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Calcific Tendinitis > Pathophysiology. [24] Orthopaedic Knowledge Update Sports Medicine 6. Rotator Cuff Disease > Natural History and Societal Impact. [25] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Rotator Cuff Tears > Evaluation. [26] Apley And Solomon S Concise System Of Orthopaedics And Trauma. SECONDARY ARTHROPATHY > TEARS OF THE ROTATOR CUFF. [27] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > Natural History of Symptomatic Rotator Cuff Tears. [28] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > ARTHROSCOPIC ROTATOR CUFF REPAIR. [30] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > NATURAL HISTORY OF ROTATOR CUFF PATHOLOGY AND IMPLICATIONS ON SURGICAL INDICATIONS > Natural History of Asymptomatic Rotator Cuff Tears. [31] Classifications And Scores Of The Shoulder. 5.7 Classification of the extent of rotator cuff tears according to Patte [107]. [32] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Rotator Cuff Tears > Role of the Biceps Tendon. [33] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > MINI-OPEN ROTATOR CUFF REPAIR.