How Bone Heals and Remodels PDF¶
Bone feels solid and permanent — but it is living tissue, laced with cells and blood vessels, and it is being taken apart and rebuilt every day of your life. That is exactly why a broken bone can knit back together into something as strong as it was before. Healing follows a predictable sequence, and it takes longer than most people expect, so knowing the pattern makes the wait far less worrying. This page explains, in plain language, what bone is and how it mends — and then, for the curious, goes a good deal deeper into the biology, including how bone constantly remodels itself and what happens when that machinery is turned against the bone.
What bone is and what it does¶
Bone does several jobs at once. It is the body's scaffolding — the frame that holds you up and that muscles pull against to move you. It is armour, protecting the brain, heart and lungs. And it is a storehouse for minerals, especially calcium, which the rest of the body draws on constantly.
To do all that, bone is a composite material — a bit like reinforced concrete. A flexible protein mesh (mostly collagen) gives it the toughness to bend slightly without snapping, and a hard mineral (a calcium-phosphate crystal) packed into that mesh gives it stiffness and compressive strength. Take the mineral away and bone is rubbery; take the collagen away and it is brittle as chalk. You need both.
Crucially, bone is not inert. It is full of living cells and threaded with blood vessels, which is why it bleeds when it breaks, why a good blood supply matters so much for healing, and why bone — unlike a scratched table — can repair itself.
How a broken bone heals¶
When a bone breaks, it heals in overlapping stages that turn a gap into solid bone again.
- The clot (first days). The break tears blood vessels in and around the bone, and the blood forms a clot at the fracture. This is not just a plug — it is the scaffold and the signal centre that summons the repair cells. This is also why the area is swollen, bruised and sore early on.
- The soft callus (first weeks). Repair cells move in and lay down a soft, rubbery bridge of cartilage and immature tissue across the gap. The bone is joined now, but only loosely — this is why a fresh fracture needs protecting in a cast, splint or with surgery while the bridge is weak.
- The hard callus (weeks to a couple of months). The soft bridge is gradually replaced by hard, mineralised bone, forming a bulky cuff (the callus) around the break. By the end of this stage the bone is usually solid enough for ordinary use.
- Remodelling (months to years). The lumpy callus is slowly carved back and reshaped along the lines of stress until the bone looks — and works — much like it did before. In children this reshaping is so good that a slightly crooked break can straighten out over time.
Healing is genuinely slow, and that is normal. As a rough guide many adult fractures take around six to twelve weeks to become solid, and longer to regain full strength; the remodelling that perfects the shape can run on for a year or more. The timeline depends on the bone, the person and the injury — so treat these as guides, not promises.
What helps it heal¶
A few things make a real difference, and most are in your control:
- Blood supply and a settled break. Bone heals best when the broken ends have a good blood supply and are held reasonably still — which is the whole point of a cast or an operation. Too much movement, or a poor blood supply, is the commonest reason a break is slow to unite.
- Not smoking. Smoking and nicotine narrow blood vessels and meaningfully slow bone healing — stopping, even around the time of an injury or operation, helps.
- Nutrition. Bone is built from protein and mineral, so adequate protein, calcium and vitamin D support healing. Most people don't need megadoses — they need to not be deficient.
- Sensible loading. Bone responds to use. Following the weight-bearing and exercise advice you're given — not too much, not too little — guides the healing bone to rebuild in the right places.
- Time and review. Most breaks heal on their own timeline. If one that should be improving isn't, that's worth reviewing — some need a helping hand from surgery.
In more depth¶
This section steps up to a more detailed, student-level explanation of the biology behind everything above. It isn't needed to understand a fracture or its treatment — but if you're curious about how bone actually works, and how the very same machinery that heals a break can also be turned against the skeleton, read on.
Bone as living tissue¶
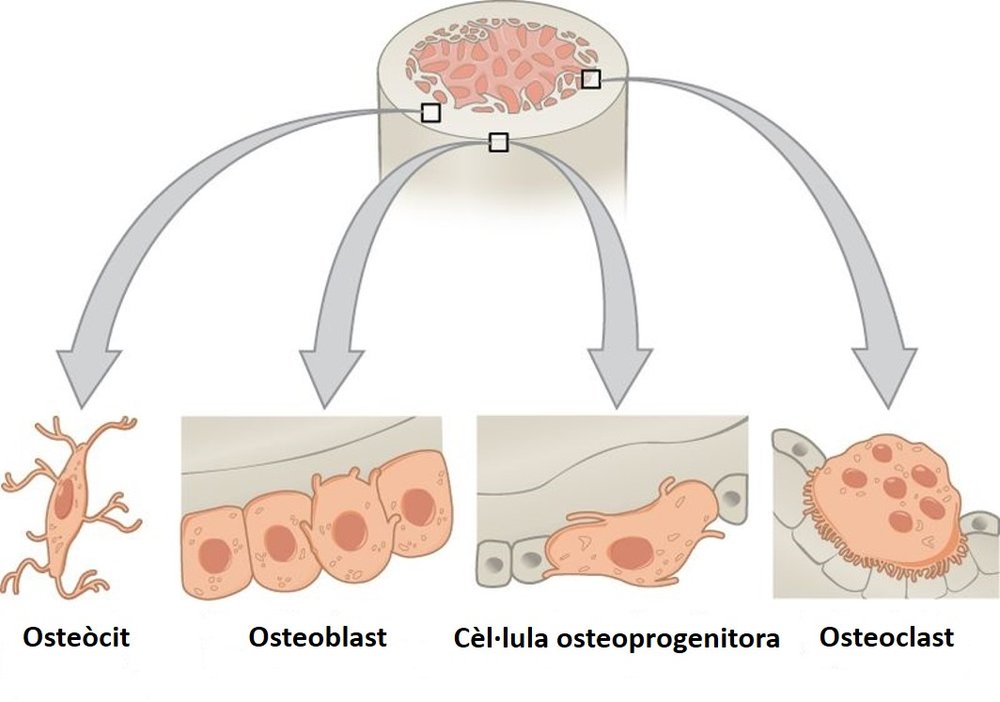
Bone is built and maintained by three main cell types, and it helps to meet them by name because almost everything that follows is a story about the balance between them:
- Osteoblasts are the builders. They lay down new bone — first the soft collagen framework (osteoid), which they then mineralise into hard bone.
- Osteoclasts are the demolition crew. They are large, multi-nucleated cells that dissolve bone, etching the mineral with acid and digesting the collagen with enzymes.
- Osteocytes are former osteoblasts that became trapped in the bone they built. They sit in tiny chambers connected by a vast network of channels, wired together like a sensor grid throughout the bone — and, as we'll see, they are the cells that feel mechanical load and direct the other two.
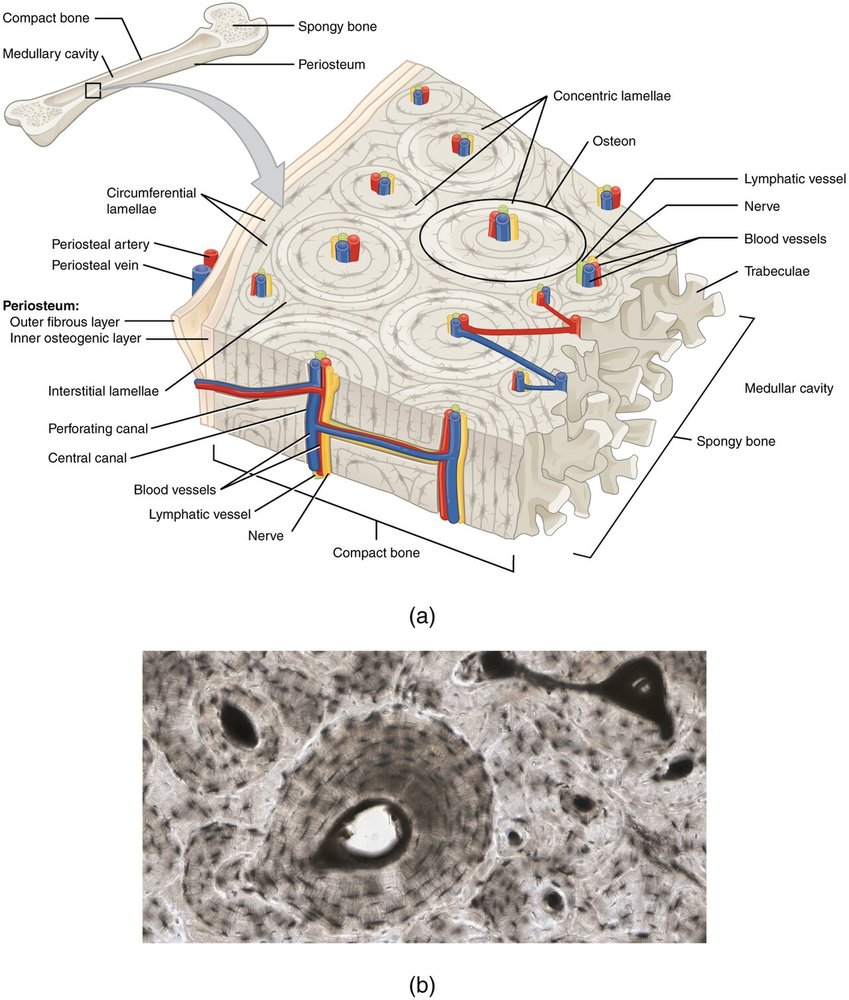
The hard matrix these cells live in is type I collagen stiffened by crystals of hydroxyapatite (a calcium-phosphate mineral). Bone comes in two architectures: dense cortical (compact) bone in the shafts of long bones, and spongy trabecular (cancellous) bone — an open lattice — at the ends of bones and inside the spine.
The healing cascade¶
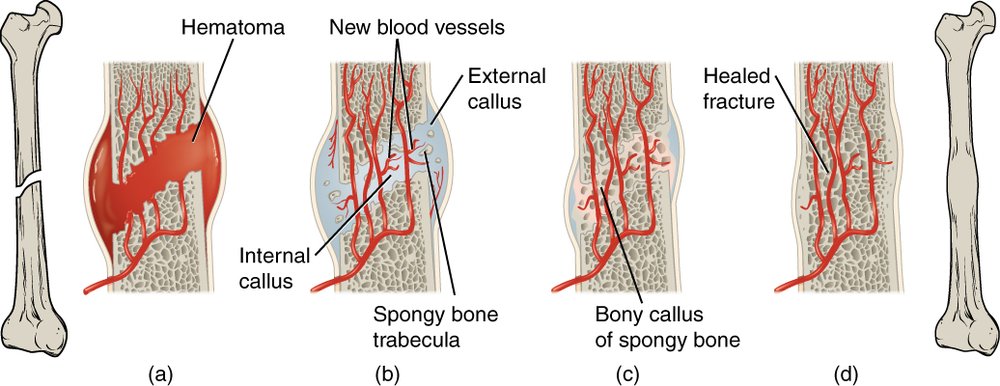
The four plain-language stages above map onto a precise biological sequence. The fracture haematoma (clot) releases a flood of inflammatory signals and growth factors that recruit stem cells. Those cells first form a soft (cartilaginous) callus — bone is built on a cartilage template in a process called endochondral ossification, the same process by which much of the skeleton grows in childhood. The cartilage is then invaded by blood vessels and replaced by woven bone — the hard callus — which is finally remodelled into mature, organised lamellar bone.
That is secondary (indirect) healing — healing through a callus — and it is what happens when a break has a little movement, as in a cast. There is also primary (direct) healing, which happens only when the bone ends are held rigidly together with no gap and no movement (for example, compressed under a metal plate). Then there is no callus at all: bone simply remodels straight across the join. Neither is "better" — they are the bone's two answers to different mechanical conditions, which is why surgeons choose fixation to suit the fracture.
Remodelling and the cutting cone¶
Even unbroken bone is rebuilt continuously — you replace roughly a tenth of your skeleton every year. This lifelong renewal is remodelling, and it is carried out by teams of cells called Basic Multicellular Units (BMUs).
In dense cortical bone you can watch a BMU at work as a microscopic tunnelling machine. At its leading edge, a pack of osteoclasts bores a tunnel straight through the bone, dissolving it as they advance — this resorbing tip is the cutting cone. Following close behind, in the closing cone, osteoblasts line the fresh tunnel and refill it from the walls inward, laying down concentric rings of new bone around a central channel that carries a blood vessel. The finished cylinder — rings of bone around a central canal — is an osteon, the basic structural unit of compact bone. So remodelling is not random: it is a coordinated convoy of demolition followed by reconstruction, threading new, well-aligned bone through the old.
This is also why healthy bone needs both cell types working in step. The osteoclasts that lead the cutting cone are the very same cells that, dysregulated, drive the bone-loss diseases described below.
The coupling switch: RANK, RANKL and OPG¶
How does the builder control the demolition crew? Through a molecular switch that is worth knowing because it is the lever behind both normal remodelling and several diseases (and several drugs).
Osteoblast-lineage cells display a signal called RANKL. When RANKL plugs into its receptor, RANK, on the surface of osteoclast precursors, it tells them to mature into active, bone-dissolving osteoclasts. So the builders hold the remote control for the demolition crew. To apply the brake, the same osteoblasts secrete a decoy called OPG (osteoprotegerin), which mops up RANKL before it can reach RANK. The RANKL-to-OPG ratio therefore sets the pace of bone resorption: more RANKL tips the balance toward bone loss, more OPG toward bone preservation.
Almost every signal that affects bone — hormones, inflammation, drugs — ultimately pulls on this lever. It is, for instance, exactly where the osteoporosis drug denosumab acts: it is a man-made antibody that works like OPG, soaking up RANKL to switch off osteoclasts. Hold onto this switch — the next two sections are both stories about RANKL being pushed the wrong way.
Mechanotransduction and Wolff's law¶
Bone famously adapts to the loads placed on it — "bone is laid down where it is needed and resorbed where it is not." This is Wolff's law, and it is why a tennis player's racket arm has denser bone, why astronauts and bed-bound patients lose bone, and why sensible loading helps a fracture rebuild in the right places.
The cells that sense the load are the osteocytes buried in the bone. As bone is loaded, fluid is squeezed through the tiny channels around them, and the osteocytes feel that flow — a process called mechanotransduction (turning a mechanical signal into a biological one). Loaded osteocytes dial down a braking molecule called sclerostin, which releases the osteoblasts to build; unloaded bone does the reverse, and is given over to resorption. So "use it or lose it" is not just a slogan — it is osteocytes adjusting the RANKL/OPG balance in response to what you do.
When remodelling goes wrong: osteolysis and sonic hedgehog¶
Osteolysis simply means bone being dissolved away — osteoclasts running unchecked, usually because something is jamming the RANKL switch in the "on" position. It is what makes a tumour eat into bone, what loosens an implant (next section), and what hollows out bone in some inflammatory diseases.
One of the more surprising controllers here is sonic hedgehog (Shh) — a signalling molecule best known for sculpting the body plan of the embryo (it helps lay out the limbs and digits). The same pathway is reused in the adult skeleton, and it cuts both ways. In a healing fracture, Shh signalling actually helps — it supports osteoblasts and bone formation. But in osteolysis it does the opposite: Shh, acting through its downstream messenger Gli, prompts the supporting stromal cells to make more RANKL — and more RANKL means more osteoclasts and more bone dissolved. Tellingly, Shh on its own doesn't resorb bone; it works by amplifying the RANKL pathway, which is exactly why it shows up as an aggravator in conditions like cancer-associated bone destruction. It is a neat illustration of a theme running through this whole page: most bone disease is the normal remodelling machinery — the cutting cone, the RANKL switch — pushed too far in one direction.
Polyethylene wear and implant loosening¶
This is where the biology becomes very practical, because it explains how joint replacements eventually fail. A hip or knee replacement has a smooth bearing surface, classically a hard ball or metal component moving against a polyethylene (medical-grade plastic) liner. Over years of use, friction sheds astronomically small wear particles of polyethylene — far too small to see, and shed in their billions.
The body treats these particles as intruders. Scavenger immune cells (macrophages) around the implant try to engulf them, but the plastic is indigestible, so the frustrated macrophages instead pour out inflammatory signals. Those signals — predictably — drive RANKL up, recruiting osteoclasts that resorb the bone around the implant. This particle-induced (or wear) osteolysis quietly eats away the bony anchorage, and eventually the implant loosens — a leading cause of joint replacements wearing out and needing revision, often a decade or more after surgery. It is the same final common pathway as everything above: an outside trigger, funnelled through RANKL, ending in osteoclasts dissolving bone. Understanding it is exactly why so much engineering goes into better bearing materials (such as cross-linked polyethylene) that shed fewer, less troublesome particles.
What helps and harms healing¶
Finally, the practical factors, now with the biology to explain them:
- Blood supply delivers the cells, oxygen and signals healing needs; a stripped or crushed soft-tissue envelope, or a break in a poorly-supplied bone, heals slowly. This is the single biggest factor.
- Stability lets the callus mature; excessive movement keeps breaking the fragile early bridge, and is a common road to a non-union (a break that fails to heal).
- Smoking and nicotine constrict blood vessels and impair the repair cells — a well-established brake on bone healing.
- Diabetes and some medications (long courses of steroids, and some anti-inflammatories around the time of a fresh fracture) can slow healing.
- Nutrition — adequate protein, calcium and vitamin D — supplies the raw materials; deficiency, not abundance, is the problem to avoid.
- Age slows the cellular machinery, but bone retains a remarkable capacity to heal throughout life.
See also¶
- Bone health and osteoporosis — when the remodelling balance tips toward bone loss across the whole skeleton
- Smoking and musculoskeletal healing — why smoking slows the healing described here
- Vitamin D and musculoskeletal health — the mineral side of building bone