Patients › Rehabilitation
Olecranon Fracture (ORIF)
Recovery after surgical fixation of an olecranon (point-of-elbow) fracture, protecting the triceps repair while restoring movement, with a simple sling and a staged return of active extension.

This protocol guides your recovery after surgical fixation of a fracture of the olecranon (the bony point of your elbow) with open reduction and internal fixation (ORIF), performed by Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your physiotherapist or hand therapist. Bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
The olecranon is the bony point of your elbow. The large triceps muscle at the back of your arm attaches to it, and it forms part of the hinge joint inside the elbow. When the olecranon breaks, the pull of the triceps tends to drag the broken piece apart, so the fracture is fixed surgically, either with a wire-and-pin "tension band" (for a clean, straight break) or with a plate and screws (for a more shattered or angled break). The fixation is built to hold the bone together firmly enough that you can start moving the elbow early.
The whole aim of this rehabilitation is a balancing act. An elbow that is held still for too long becomes stiff very quickly, so we want to get it moving early. But the same triceps muscle that pulls the fracture apart is the muscle that straightens your elbow, so for the first six weeks we protect the repair by avoiding active straightening, while freely working on bending the elbow and rotating the forearm. Once the bone has had time to knit, straightening is reintroduced gradually: first using just the weight of your arm, and only much later against resistance.
For wound, swelling and scar management, see the practice's wound care guidance.
It is worth knowing from the outset that even after a well-fixed olecranon fracture, most people are left with a small permanent loss of the last 10–15 degrees of full straightening. This is normal, rarely noticeable in everyday life, and not a sign that anything has gone wrong.
Precautions and limitations¶
Do
- Wear your simple sling for comfort and support, taking it off for your exercises. You do not need a rigid splint or brace.
- Work on bending the elbow and rotating the forearm (palm up / palm down) from early on, within comfortable limits.
- Keep your hand, wrist and shoulder moving freely, and squeeze a ball to keep your grip strong.
Do not
- Do not actively straighten your elbow under its own muscle power for the first 6 weeks; let it straighten with gravity only. Active straightening pulls on the triceps and can distract the fracture.
- Do not do any resisted or weighted straightening until about 3 months, when your therapist clears it.
- Do not lift, push or pull with the operated arm, and do not bear weight through it, in the early weeks.
These are the exercises from your handout, for regaining movement of your elbow and forearm. Take your sling off for your exercises. Start them as guided by Dr Hirpara and your therapist.
Your exercises¶
Kieran Hirpara 4.0
Passive elbow flexion
Rest your operated arm with the palm facing up. Use your other hand to gently bend the operated elbow as far as is comfortable, helping it move rather than using the operated arm's own muscles. Hold for a few seconds at the end of the comfortable range, then slowly let it straighten back. This builds your bend (flexion) without loading the repair.
10 times, 3–4 times a day

Kieran Hirpara 4.0
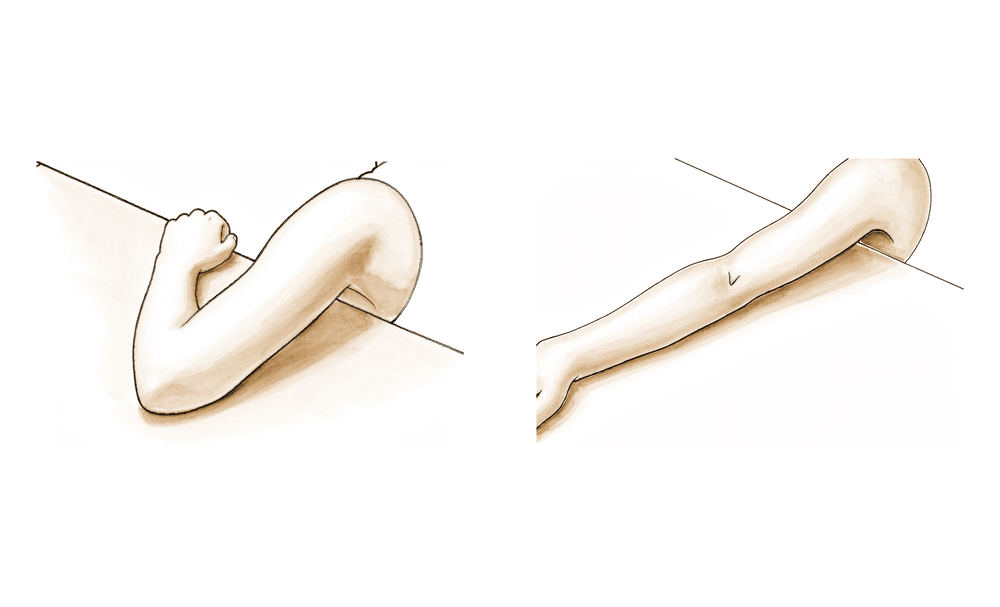
Active elbow bends
With your palm facing up and your upper arm tucked at your side, gently bend your elbow as far as you can, then let it straighten back under control. In the first six weeks, let the elbow straighten with gravity — do NOT push it straight using your own muscles.
10–15 times, 3–4 times a day
Kieran Hirpara 4.0
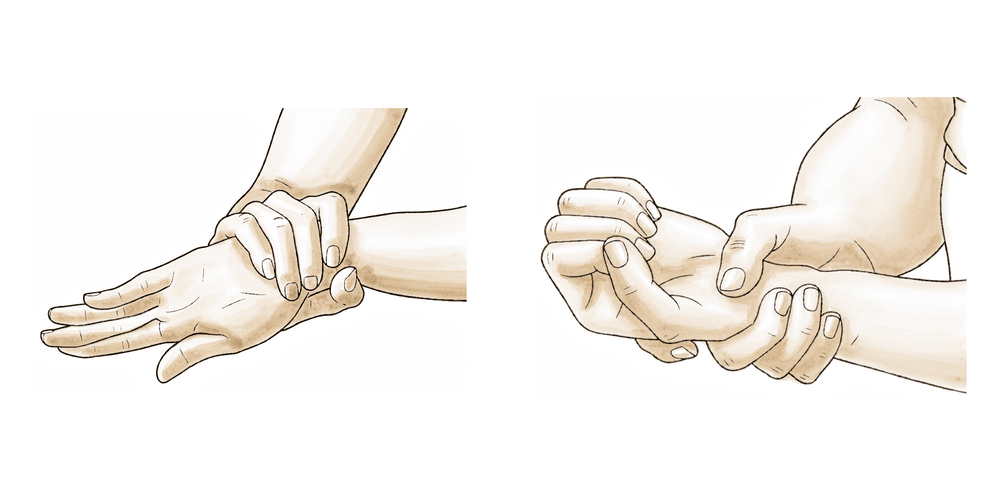
Forearm rotation
Keep your elbow tucked at your side and bent to about a right angle. Slowly turn your palm up towards the ceiling, hold for 3–5 seconds, then turn it down towards the floor. Keep the elbow still and against your body throughout. You may gently assist the movement with your other hand.
10 times each direction, 3–4 times a day

Kieran Hirpara 4.0
Grip strengthening
Squeeze a soft ball or a roll of putty in your hand, hold for a few seconds, then release. This keeps your hand and forearm strong while your elbow is protected. It does not load the elbow repair.
10–15 squeezes, 2–3 times a day

Kieran Hirpara 4.0
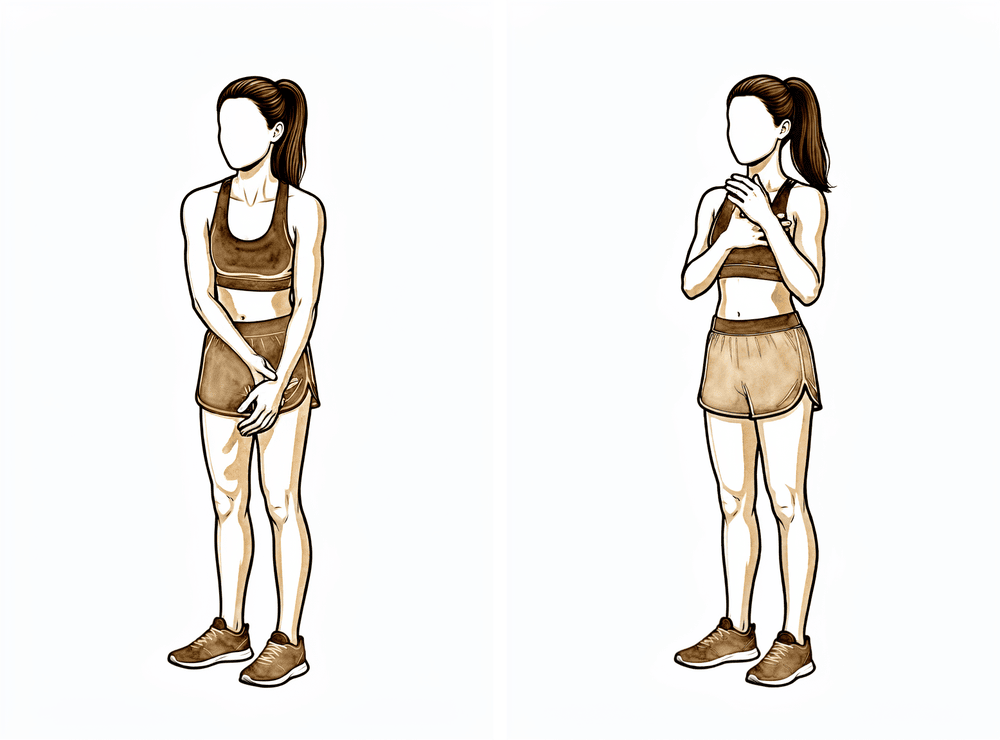
Isometric elbow-bend hold
With your elbow bent and your palm up, place your other hand under your forearm. Gently try to bend the elbow further while your other hand holds it still, so the muscle works but the arm does not move. Hold gently, then relax. This is a muscle-activation (isometric) drill — it works the bending muscles only and does NOT load the triceps or the repair.
Hold 5 seconds, 5–10 times, 2–3 times a day
Kieran Hirpara 4.0
Active elbow extension (against gravity)
Only begin this once your surgeon or therapist clears it, usually from six weeks. With your upper arm supported, slowly straighten your elbow using your own muscle power, then bend it back under control. Work against gravity only — do NOT add any weight or resistance until your therapist advances you (usually around three months).
10 times, 2–3 times a day — from week 6 only
Kieran Hirpara 4.0
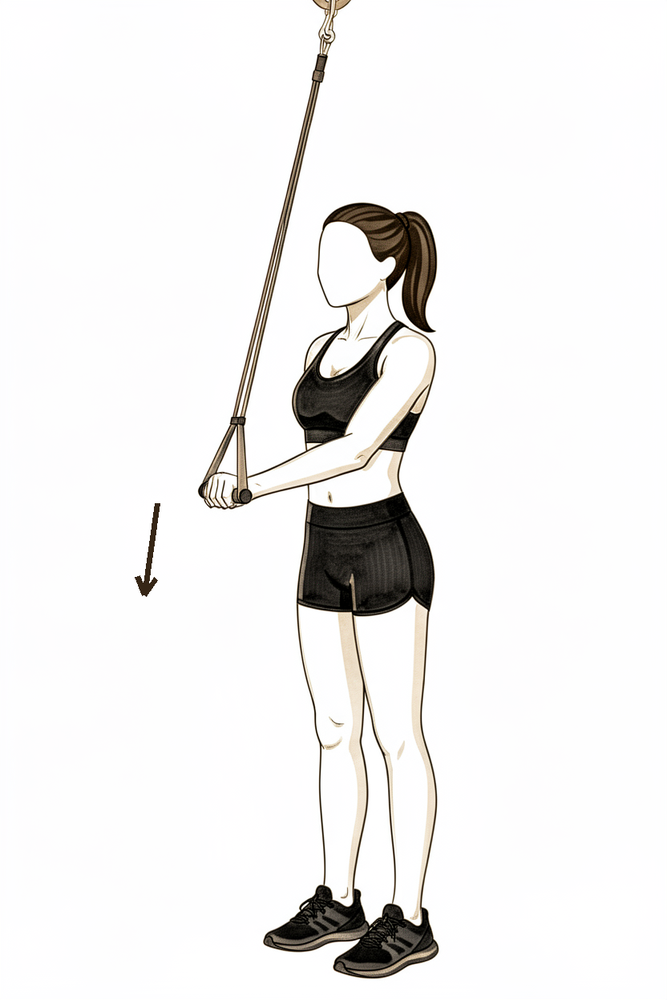
Resisted band extension
This is a late-stage exercise, started only from about three months when your therapist clears it. Anchor a light resistance band and straighten your elbow against its pull, then return slowly. Begin with the lightest band and progress to light weights (around 0.5–2 kg) only as guided. Resisted straightening directly loads the triceps and the repair, which is why it is delayed.
10–15 times, 3 times a week — from ~3 months only
Your clinical protocol¶
The rest of this page is the clinical protocol for an olecranon fracture treated with open reduction and internal fixation. This section is to be provided to your physiotherapist or hand therapist, and each phase below opens with a plain-English explanation of what is happening. The single most important rule that distinguishes this protocol from a generic elbow fracture is triceps protection: active extension is deferred to ~6 weeks and resisted extension to ~3 months, because the triceps inserts on the olecranon and loads the fixation.
Prior to treatment, check the patient's x-ray, operation report and past medical history, and liaise with the treating surgeon regarding the fixation construct (tension-band wiring vs plate), its stability, and the likely prognosis.
Weeks 0–1: immobilisation¶
In the first week the focus is on resting the soft tissues, settling swelling, and keeping everything else moving. The elbow rests in a simple sling at about 90°, taken off for exercises. There is no rigid posterior splint or brace.
For your physiotherapist:
- Immobilisation: simple sling, elbow at ~90°, removed for exercises (KH override: no posterior splint or brace).
- Goals: soft-tissue rest; oedema control (elevation, gentle compression, cold).
- Exercises: active hand, wrist and shoulder range of motion; gentle active elbow and forearm range of motion may begin from day 2–3 if the construct is stable.
- Precautions: non-weight-bearing upper limb; no lifting, pushing or pulling; no active elbow extension.
- Criteria to progress: wound and swelling settling.
Weeks 1–6: protected motion (extension restricted)¶
This is the triceps-protection phase. Bending is advanced steadily while straightening is done passively or by gravity only, never under the elbow's own straightening power. The sling is weaned from about week 4.
For your physiotherapist:
- ROM ceiling: flexion advanced approximately 10° per week within a tension-free range; goal full passive extension, tension-free flexion to 120°, and full forearm rotation by 6 weeks. Passive extension only: NO active extension.
- Exercises: active and active-assisted flexion plus pronation/supination; passive range of motion may begin ~week 4. Cuff, periscapular and forearm isometrics only, not elbow extension.
- Orthosis: wean the sling at week 4 (worn out-of-house and at night thereafter for comfort).
- Criteria to progress: full passive extension, flexion to ~120°, full rotation; pain ≤3/10.
Weeks 6–12: active extension introduced¶
Once the bone has had six weeks to knit, active straightening is reintroduced, against gravity only and with no added weight. Bending is advanced towards a full arc, and weight-bearing through the arm is progressed gently.
For your physiotherapist:
- Goals: complete the motion arc; introduce gentle active extension.
- Exercises: active elbow extension against gravity only from week 6; advance flexion to full (goal full tension-free arc by ~week 9). Progress weight-bearing tabletop → wall → quadruped as tolerated. Progressive resistive exercise to flexion/rotation may begin, but still NO resisted extension: this is held to 3 months.
- Criteria to progress: full active arc; no worsening extension lag; radiographic union.
3–6 months: resisted extension and return¶
Resisted straightening (the step that directly loads the triceps and the repair) begins only now, once the fracture has united.
For your physiotherapist:
- Resisted elbow extension begins at ~3 months (bands progressing to light weights, ~0.5–2 kg / 1–5 lb, 3×/week).
- Sport- and job-specific exercises from ~4.5 months.
- Lifting and heavy labour return once full strength and union are achieved, usually by around 6 months.
- Hardware removal is common after olecranon fixation (especially tension-band wires, the most frequently removed implant in the body) and is usually done after union, for relief of prominent or irritating hardware, not as a routine step.
Getting back to work and activity¶
Light, hands-on-lap use of the arm for self-care is fine from early on within the precautions above, but anything that loads the elbow waits its turn. Bending and forearm rotation usually feel comfortable by about six weeks; active straightening returns from six weeks and steadily improves over the following weeks.
Heavier demands are staged: no resisted or weighted straightening until about three months, sport- and job-specific training from around four and a half months, and a return to lifting and heavy manual work usually by about six months, once your strength and the healing of the bone allow it. Desk-based and light duties can typically resume much sooner; discuss the timing with Dr Hirpara at your review, as it depends on your job and which arm was operated on. Driving resumes once you are out of the sling and can safely control the vehicle with both arms, as confirmed at your review.
Remember to expect a small permanent loss of the last 10–15 degrees of straightening; this is normal and usually has no effect on everyday function.
After your protocol¶
This protocol works alongside the practice's general recovery advice: see managing post-operative pain and wound care. For the injury itself, see olecranon fracture. The phased plan above is consistent with published rehabilitation protocols after olecranon ORIF, and your ongoing recovery is guided individually by your physiotherapist or hand therapist according to how your elbow progresses.
Evidence & references
Olecranon Fracture — Open Reduction Internal Fixation (ORIF) — Post-operative Rehabilitation¶
Topic scope: Post-operative rehabilitation after ORIF of a displaced olecranon fracture — tension-band wiring (TBW) for simple transverse patterns, or plate-and-screw fixation for comminuted / oblique / Monteggia-type / proximal-ulna patterns. The olecranon fracture is an intra-articular fracture of the extensor mechanism: the fixation construct must resist the triceps pull that distracts the fragment, and the rehabilitation is built around protecting that construct while preventing the stiffness to which the elbow is highly prone.
Defining principle (the inverse of an arthrolysis): unlike a stiff-elbow release, here there is a fixation construct to protect, and the deforming force is the triceps. So active and resisted elbow EXTENSION — and lifting / pushing — are restricted early, while flexion and forearm rotation are advanced relatively freely to prevent stiffness. Dr Hirpara's practice override: the operated elbow is rested in a simple sling, not a posterior splint or brace; active extension is withheld for 0–6 weeks (protecting the tension band / triceps insertion), resisted extension is delayed to ~3 months, flexion is advanced ~10°/week, and the patient is counselled to expect a permanent 10–15° loss of terminal extension.
Evidence-strength flag: MODERATE-to-STRONG. Two concordant institutional physiotherapy protocols (Brigham & Women's Hospital; The Christ Hospital / Rao) give explicit phase timelines, and the biomechanical rationale — anatomic reduction plus stable fixation to permit early motion of an intra-articular fracture — is universally agreed. Consensus is strong on early protected motion + delayed active / resisted extension and triceps loading. The evidence is weaker (equipoise-level) on TBW vs plate, and on operative vs non-operative management in the elderly.
Phased rehabilitation timeline¶
| Phase | Window | Sling / immobilisation | ROM / use | Strengthening | Criteria to progress |
|---|---|---|---|---|---|
| I — Immobilisation | Weeks 0–1 | Simple sling at ~90° (KH — no posterior splint/brace), off for exercises | Active hand/wrist/shoulder ROM; gentle active elbow + forearm ROM from day 2–3 if stable; NO active extension | — (oedema control) | Wound and swelling settling |
| II — Protected motion, extension restricted | Weeks 1–6 | Wean sling at week 4 (out-of-house + night thereafter) | Flexion advanced ~10°/week in a tension-free zone; passive extension only; PROM may begin ~wk 4; goal full passive extension + flexion to 120° + full rotation by 6 wk | Cuff / periscapular / forearm isometrics only | Full passive extension, flexion ~120°, full rotation; pain ≤3/10 |
| III — Active extension introduced | Weeks 6–12 | Discontinued | Active extension against gravity only from wk 6; advance flexion to full (full tension-free arc by ~wk 9); progress weight-bearing tabletop → wall → quadruped | PRE to flexion/rotation; still NO resisted extension | Full active arc; no worsening extension lag; radiographic union |
| IV — Resisted extension + return | 3–6 months | — | Return to lifting/loading staged | Resisted extension from ~3 months (bands → light weights 1–5 lb, 3×/wk); sport/job-specific ~4.5 mo | Full strength + union; lifting/heavy labour ~6 mo |
Evidence by theme¶
The triceps-pull rule (the rehab-defining constraint) — Consensus, strong biomechanical rationale¶
The triceps inserts on the olecranon; active and resisted extension distract the fracture and load the tension band. Active extension against gravity is therefore deferred to ~6 weeks and resisted extension to ~3 months. This is the single most important rule distinguishing olecranon ORIF from a generic elbow-fracture rehabilitation, and both published protocols enforce it (The Christ Hospital / Rao explicitly prohibit active extension for the first six weeks).
Early protected motion to prevent stiffness — Strong consensus¶
There is universal agreement that an intra-articular extensor-mechanism fracture needs early motion to prevent stiffness; how early depends on construct stability and surgeon confidence. Brigham permits active ROM from day 2–3; the more conservative Christ / Rao protocol protects the first weeks with no active extension. The tension throughout is "prevent stiffness" versus "protect the triceps repair," resolved by advancing flexion and rotation freely while restricting extension.
Construct choice — TBW vs plate — Moderate / equipoise¶
Both constructs aim to be stable enough for early motion. TBW is simpler and adequate for simple transverse fractures but carries the highest symptomatic-hardware / removal rate and can lose compression in comminuted or osteoporotic bone. Plate fixation better controls comminution, oblique and diaphyseal-extension patterns; Hume & Wiss's randomized study favoured plate over TBW for comminuted patterns, while Anderson et al. reported a mean ~13.5° flexion contracture after plating. Rehabilitation phases are broadly the same — a more stable construct simply allows the surgeon to liberalise motion sooner.
Operative vs non-operative in the elderly — Moderate (RCT, equipoise)¶
A prospective RCT of displaced olecranon fractures in elderly patients was stopped early for a high operative complication rate, with comparable patient-reported outcomes — shifting practice toward non-operative management and earlier free mobilisation in low-demand older patients. Geriatric locking plates reduce fixation failure in osteoporotic bone but still carry meaningful complication and implant-failure rates.
Expected residual deficit — Moderate (corpus, observational)¶
Even with stable fixation and early motion, isolated olecranon fractures lose ~10–15° of terminal extension on average. Patients should be counselled that this is the expected norm, not a complication.
Hardware removal — Moderate (observational)¶
Olecranon hardware — especially TBW K-wires / wires — is the most commonly removed implant in the body; prominent subcutaneous hardware drives a high secondary-removal rate (up to roughly half of TBW cases in some series). Removal is typically performed after union (often ≥4–6 months) and largely for symptom relief, not as a routine staged step. Plate fixation has fewer wire-irritation issues but a non-trivial removal rate.
Evidence strength flags (summary)¶
- STRONG / CONSENSUS: early protected motion to prevent stiffness; the triceps-pull rule deferring active extension to ~6 weeks and resisted extension to ~3 months (biomechanical rationale
- two concordant institutional protocols).
- MODERATE: TBW vs plate construct choice (Hume & Wiss; Anderson ~13.5° contracture after plating); operative vs non-operative in the elderly (RCT stopped early for operative complications); expected 10–15° terminal-extension loss; high TBW hardware-removal rate.
- CONSENSUS / EXPERT: the precise phase timings (drawn from surgeon patient-guidance protocols rather than a rehabilitation RCT); the simple-sling immobilisation (KH practice override).
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Chalidis BE, Sachinis NC, Samoladas EP, Dimitriou CG, Pournaras JD. Is tension band wiring technique the "gold standard" for the treatment of olecranon fractures? A long-term functional outcome study. J Orthop Surg Res. 2008;3:9. DOI: 10.1186/1749-799X-3-9
- Hume MC, Wiss DA. Olecranon fractures: a clinical and radiographic comparison of tension band wiring and plate fixation (randomized comparison; plate favoured for comminuted patterns). (Cited in retrieved corpus text.)
- Anderson et al. — mean ~13.5° flexion contracture after olecranon plate fixation (retrieved corpus text).
- Prospective RCT, operative vs non-operative management of displaced olecranon fractures in the elderly — stopped early for a high rate of complications in the operative group, comparable patient-reported outcomes (retrieved corpus text).
- Geriatric olecranon locking-plate case series — major/minor complication and implant-failure rates (J Shoulder Elbow Surg, retrieved corpus text).
- Retrieved corpus text: isolated olecranon fractures lose an average of ~10–15° of terminal extension despite stable fixation and early ROM; anatomic reduction and early range of motion to restore functional elbow motion and strength; high re-operation / hardware-removal rate after TBW.
Published rehabilitation protocols (URLs)¶
- The Christ Hospital / Rao — "Olecranon ORIF Physical Therapy Protocol." https://www.thechristhospital.com/landingpages/Documents/Rao%20PT%20Protocols/Operative/Elbow/Rao%20Olecranon%20ORIF%20r1.pdf
- Brigham & Women's Hospital, Department of Rehabilitation Services — "Elbow Fracture Post-Op (Radial Head / Olecranon ORIF) Hand Therapy Guideline" (2021). https://www.brighamandwomens.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/elbow-fracture-orif-hand-therapy-protocol.pdf
- Physiopedia — "Olecranon Fracture" (general background). https://www.physio-pedia.com/Olecranon_Fracture