Clinicians › Shoulder
Rotator cuff repair
Surgeon-side topic for rotator cuff repair. Backed by 410 articles from the corpus, retrieved via combined MeSH + title-text matching.
For patients: a plain-language version of this topic is available. See the patient guide.
Overview¶
Rotator cuff repair is indicated for patients with partial-thickness or massive tears, with arthroscopic in situ repair of partial-thickness tears producing excellent functional outcomes in more than 80% of patients during long-term follow-up and low revision rates [9]. Arthroscopic repair is recommended for massive tears due to functional gain at midterm follow-up, despite a high rate of healing failures [18]. Partial rotator cuff repair provides respectable outcomes and comparable clinical results to complete repair for large to massive tears, particularly when complete repair is not possible or cost limitations prohibit augmentation [86]. Initial reports of graft augmentation demonstrate clinical improvements that could significantly change treatment approaches for arthroscopic rotator cuff repair [8].
Patient age, expectations, and the extent of the rotator cuff tear influence outcomes following rotator cuff repair [5]. Patients 75 years or older achieve similar early outcomes after arthroscopic rotator cuff repair compared to patients under age 75 years, provided proper patient selection is used [32]. Most patients achieve clinically significant outcomes for the PROMIS-UE within 12 months of rotator cuff repair [25]. One-year follow-up appears clinically sufficient for rotator cuff repair outcomes, as 1-year and 2-year outcomes are clinically similar [1]. Both patient-reported outcomes and achievement of clinically significant outcomes show small differences at 1 and 2 years after arthroscopic rotator cuff repair [11]. The widely accepted 2-year benchmark for rotator cuff repair outcomes may be arbitrary and does not add clinical relevance [1].
At long-term follow-up (≥15 years), patient-reported outcomes of all-arthroscopic rotator cuff repair show significant improvement from baseline preoperative function and remain durable over 15 years [3]. One-year follow-up is not the last word for rotator cuff repair outcomes, as patients must live with long-term outcomes and authors are obliged to evaluate them [4]. Patients achieve significant and comparable improvements in functional outcomes at 2 years postoperatively without augmentation, regardless of their predicted risk of repair failure based on the RoHI score [34]. Predicted healing rates do not correlate with patient outcomes following rotator cuff repair at a minimum 2-year follow-up [34].
Anatomy & Pathophysiology¶
Osseous and Tendinous Architecture¶
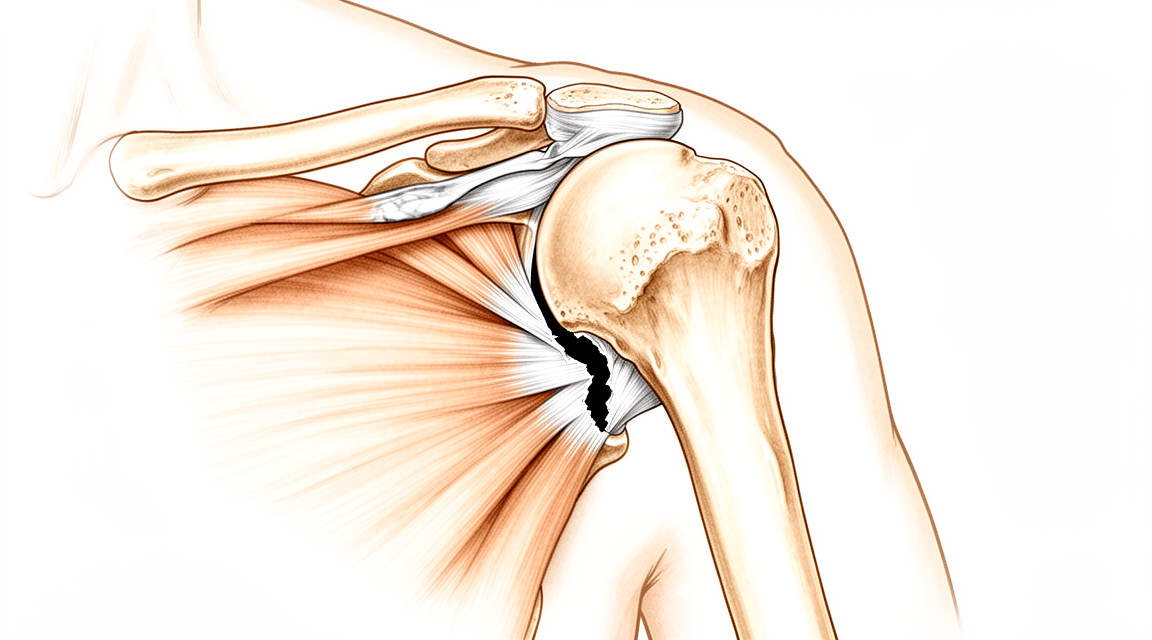
The rotator cuff comprises four muscles arising from the scapula whose tendons blend with the subjacent capsule to attach to the humeral tuberosities [44]. The subscapularis arises from the anterior scapula, attaches to the lesser tuberosity, and is innervated by the upper and lower subscapular nerves [44]. The supraspinatus arises from the fossa superior to the scapular spine, passes beneath the acromion and acromioclavicular joint, attaches to the superior greater tuberosity, and is innervated by the suprascapular nerve after it passes through the suprascapular notch [44]. The infraspinatus arises from the fossa below the scapular spine, attaches to the posterolateral greater tuberosity, and is innervated by the suprascapular nerve after it passes through the spinoglenoid notch [44]. The teres minor arises from the lower lateral scapula, attaches to the lower greater tuberosity, and is innervated by a branch of the axillary nerve [44].
Rotator cuff tendons consist of five distinct layers: superficial coracohumeral ligament fibers, large parallel tendon bundles, smaller obliquely oriented tendon fascicles, loose connective tissue with thick collagen bands, and the superior joint capsule [44]. There is significant interdigitation and overlap of rotator cuff tendons near the footprint, with the infraspinatus insertion occupying the preponderance of the greater tuberosity footprint [44]. The supraspinatus footprint measures 13 mm in medial-lateral width and 20 mm in anterior-posterior depth [45]. The infraspinatus footprint measures 14 mm in width and 20 mm in superoinferior height [45]. The rotator cable is a thick bundle of fibers running perpendicular to the supraspinatus tendon fibers, connecting the supraspinatus and infraspinatus tendons [45]. The rotator cable is divided into anterior, middle, and posterior segments, with the middle segment forming a laterally based arch or suspension bridge visible on ultrasound [46].
Biceps and Coracoacromial Complex¶
The long head of the biceps tendon attaches to the supraglenoid tubercle, runs between the subscapularis and supraspinatus tendons, and exits through the bicipital groove under the transverse humeral ligament [44]. The long head of the biceps tendon serves as a passive restraint during shoulder motion, contributes to anterior stability in abduction and external rotation, and guides humeral head elevation [44]. The coracoacromial arch is formed by the acromion process, coracoid process, and coracoacromial ligament, with the subacromial bursa separating the tendons from this fibro-osseous canopy [19].
Ligamentous Stabilizers¶
The primary passive stabilizers of the glenohumeral joint are the capsule and scapulohumeral ligaments, which act as checkreins at the extremes of motion [48]. The glenohumeral capsule is thickest in the inferior pouch (2.8 mm), with anterior (2.4 mm) and posterior (2.2 mm) portions, ranging from 1.3 to 4.5 mm in cadaveric specimens [48]. The superior glenohumeral ligament crosses the rotator interval capsule between the supraspinatus and subscapularis tendons [48]. The coracohumeral ligament originates at the coracoid base, blends into the cuff tendons, and inserts into the greater and lesser tuberosities [48]. The superior glenohumeral ligament and coracohumeral ligament come under tension with glenohumeral flexion, extension, external rotation, and adduction to resist posterior and inferior humeral head displacement [48]. The middle glenohumeral ligament originates anterosuperiorly on the glenoid and inserts midway along the anterior humeral articular surface adjacent to the lesser tuberosity [48]. The middle glenohumeral ligament is tensioned by external rotation when the humerus is abducted to 45 degrees [48].
Vascular and Neural Considerations¶
The suprascapular nerve is at risk of compression from paralgenoid cysts at both the suprascapular and spinoglenoid notches [44]. The hypovascular critical zone is located on the articular side of the rotator cuff close to the insertion on the greater tuberosity [45].
Epidemiology and Risk Factors¶
The prevalence of rotator cuff tears increases with age, affecting 28% of patients under 50 years and 65% of patients over 70 years [45]. Full-thickness rotator cuff tear prevalence ranges from 7% to 40%, while partial-thickness tears have a 50% higher prevalence [45]. Tear prevalence ranges from 13% in patients in their fifties to 50% in patients aged 80 years or older [69]. Small full-thickness and painful partial-thickness tears increase in size by 25% to 50% within 3 to 4 years, with larger lesions progressing faster [45]. Risk factors for rotator cuff tears include age, smoking, female sex, family history, diabetes, and high cholesterol [45]. Known risk factors for rotator cuff tear development include male sex, manual labor, and history of trauma [69]. Genetic variations and inherited predispositions contribute to the risk for rotator cuff disease [14, 15]. Genome-wide association studies have identified two significant single-nucleotide polymorphisms associated with full-thickness rotator cuff tears [15]. There is a sixfold increase in rotator cuff abnormalities between the fifth and ninth decades of life attributable to age-related degenerative changes and decreased host healing potential [67].
Pathogenesis of Degeneration and Impingement¶
Rotator cuff tendinopathy represents a spectrum progressing from tendinitis (20–35 years) to tendinosis (35–45 years), full-thickness tears (>45 years), and cuff arthropathy (>65 years) [45]. Intrinsic degeneration involves age-related changes in collagen, proteoglycan, water content, and vascularity (tendinosis), typically starting on the articular side of the supraspinatus and infraspinatus [45]. Extrinsic impingement involves chronic compression on the coracoacromial arch, typically starting on the bursal side of the tendon and potentially associated with a hook-shaped acromion [45]. Acute traumatic tears occur after falls or dislocations, typically in patients under 40 years old [45]. Rotator cuff pathology is associated with acromioclavicular arthritis, proximal biceps tendinitis, and adhesive capsulitis [45].
Calcific Tendinitis¶
The prevalence of calcific tendinitis in a working population is 2.7%, with 35% of cases being symptomatic [67]. Calcific tendinitis typically affects patients aged 30 to 60 years and women more commonly than men [67]. Endocrine disorders are associated with earlier symptom onset, longer duration, and higher surgery rates in calcific tendinitis [67]. The supraspinatus tendon is the most commonly involved tendon in calcific tendinitis [67]. Calcific tendinitis pathogenesis involves an active cell-mediated process with three stages: precalcific (fibrocartilaginous metaplasia), calcific (calcium hydroxyapatite deposit formation), and postcalcific (resorption) [67]. The resorptive phase of calcific tendinitis is exquisitely painful due to an inflammatory response correlated with macrophage activity [67]. Calcific tendinitis is generally self-limited and resolves spontaneously [67].
Natural History and Cuff Tear Arthropathy¶
The natural history of asymptomatic rotator cuff tears shows that symptoms improve over the first year but then plateau, representing a regression to the mean [13]. Natural history data links symptom emergence in asymptomatic shoulders to tear progression from partial to full thickness, worsening tear size, muscle atrophy/fatty infiltration, and new biceps pathology [69]. Symptoms in rotator cuff disease usually wax and wane periodically while physiological decline occurs over time [69]. Untreated rotator cuff tears can eventually result in cuff tear arthropathy [69]. Cuff tear arthropathy is the final stage of the shoulder impingement syndrome spectrum, affecting patients with long-term massive rotator cuff tears [49]. Cuff tear arthropathy is characterized by superior humeral head migration, subchondral osteoporosis, humeral head collapse, and painful arthritis [49]. Cuff tear arthropathy was initially known as Milwaukee shoulder syndrome due to rapidly progressive cartilage and bone destruction and calcium hydroxyapatite crystal deposition [49]. Cuff tear arthropathy affects women three times more often than men, typically over age 70, and more commonly on the dominant shoulder [49]. Risk factors for cuff tear arthropathy include chronic rotator cuff tears, hemorrhagic shoulder conditions, rheumatic disease, and crystal-induced arthropathy [49]. Pathogenesis of cuff tear arthropathy involves mechanical factors (superior migration, instability), nutritional factors (hypomobility-induced cartilage atrophy), and crystalline-induced arthropathy [49]. Radiographic signs of cuff tear arthropathy include acetabularization of the acromion, femoralization of the humeral head, eccentric superior glenoid wear, and loss of the coracoacromial arch [49].
Biomechanics and Clinical Correlates¶
Glenohumeral decentering is significantly associated with diminished shoulder function and active range of motion in all planes [52]. Increased glenohumeral joint loads due to a full-thickness supraspinatus tear can be reversed with rotator cuff repair [55]. Infraspinatus muscle contractility is the most important factor for better postoperative outcomes and preserving the acromion-humeral distance [100]. Shoulder stiffness at 3 months post-arthroscopic rotator cuff repair predicts 12-month stiffness but indicates better tendon integrity [88]. Shoulder stiffness after rotator cuff repair correlates with a higher likelihood of an intact repair at 6 months [89]. Preoperative restriction of range of motion for the hand behind the back best predicts shoulder stiffness at 6 weeks postoperatively [95]. Higher baseline grip strength predicts more favorable postoperative shoulder function following arthroscopic rotator cuff repair [106]. Shoulder function correlates negatively with fatty degeneration index at baseline and at last follow-up in patients with intact repairs [108]. Tendon properties, including mechanics, collagen organization, and histology, remain altered in chronic rotator cuff tears [103]. The critical shoulder angle is higher in patients with rotator cuff tears compared to asymptomatic individuals but is a static measure that does not change over time [13]. Patients with a critical shoulder angle greater than 38 degrees and an acromial index greater than 0.7 have higher retear rates but similar functional rates compared to controls [13]. The critical shoulder angle and acromial index do not influence 24-month functional outcomes after arthroscopic rotator cuff repair [13].
Classification¶
Rotator cuff disease is conceptualized as a continuum [10].
Ellman Classification: This system grades partial-thickness rotator cuff tears by depth [17]. Grade 1 involves 3 mm or less, Grade 2 involves 3 to 6 mm, and Grade 3 involves more than 6 mm of tendon [17]. In this classification, Grade 3 tears represent tears of more than 50% of tendon width [17].
MRI Evaluation: This modality classifies partial-thickness rotator cuff tears based on tendon width involvement [17]. Tears are classified as low grade if they involve less than 50% of tendon width and high grade if they involve more than 50% [17].
Partial-Thickness Tear Morphology: Partial-thickness rotator cuff tears are classified as articular-sided (A), bursal-sided (B), or intratendinous (C) [17].
Hamada Classification: This scheme uses a mechanistic approach to explain radiographic changes seen with chronic massive rotator cuff tears [28]. It highlights the progressive nature of massive rotator cuff tears leading to cuff tear arthropathy (CTA) [28].
Modified Patte Classification: This system is used to classify rotator cuff tendon retraction [58]. It has excellent diagnostic performance for predicting reparability and acceptable performance for predicting healing [58]. The modified Patte classification system has high measurement reliability [58].
Clinical Presentation¶
Rotator cuff syndrome is the commonest cause of pain and weakness around the shoulder [19]. The most frequent causes of shoulder pain include disorders of the rotator cuff, chiefly rotator cuff syndrome, calcific tendinitis, and adhesive capsulitis [19]. Rotator cuff syndrome comprises four conditions: supraspinatus impingement and tendinitis (subacute and chronic), tears of the rotator cuff, acute calcific tendinitis, and biceps tendinitis and/or rupture [19]. Patients typically complain of pain over the front and lateral aspect of the shoulder [19]. Weakness on abduction is present in supraspinatus involvement, tears of the cuff, and tendinitis [19]. Pain over the front of the shoulder is associated with biceps pathology [19]. If the cuff or biceps has ruptured, there will be weakness [19].
Patients may present with a clear history of trauma resulting in acute pain and weakness, strongly suggesting acute rotator cuff tear (RCT) [71]. In cases of chronic rotator cuff disease, patients often describe an insidious onset of lateral and/or anterior shoulder pain associated with overhead activities [71]. Night pain is a common presenting symptom of rotator cuff disease [71]. A family or personal history of rotator cuff disease makes the diagnosis more likely [71].
The most advanced stage of rotator cuff disorder is progressive fibrosis and disruption of the cuff, resulting in either a partial or full-thickness tear [75]. Patients with advanced rotator cuff tears are usually aged over 45 and give a history of refractory shoulder pain with increasing stiffness and weakness [75]. Partial tears may occur within the substance or on the deep surface of the cuff [75]. In partial tears, the remaining cuff fibers permit active abduction with a painful arc [75]. A full-thickness tear may follow a long period of chronic tendinitis or occur spontaneously after a sprain or jerking injury [75]. A full-thickness tear presents with sudden pain and inability to abduct the arm [75]. Injection of local anesthetic into the subacromial space can help differentiate partial from complete tears; if active abduction becomes possible, the tear is partial, whereas if it remains impossible, a complete tear is likely [75]. With time after a full-thickness tear, there may be some recovery of active abduction, though power in abduction and external rotation remains weaker than normal [75]. Long-standing partial or complete rupture may lead to wasting of the supraspinatus and infraspinatus [75]. In long-standing cases of partial or complete rupture, secondary osteoarthritis of the shoulder may supervene, severely restricting movements [75].
Symptoms of pain do not correlate with rotator cuff tear severity in patients with symptomatic atraumatic full-thickness tears [15]. Pain and duration of symptoms are not associated with the severity of rotator cuff tears in atraumatic, full-thickness tears [80]. The etiology of the rotator cuff tear (traumatic versus non-traumatic) did not significantly affect postoperative outcomes or healing rates [22]. Patient age influences outcomes following rotator cuff repair [5]. Patient expectations influence outcomes following rotator cuff repair [5]. The extent of the rotator cuff tear influences outcomes following rotator cuff repair [5]. Greater preoperative rotator cuff disease severity was associated with failure to achieve clinically significant outcomes at mid-term follow-up [53]. Age was an important factor in the progression of symptomatic rotator cuff tears, with progression in 54% of tears in patients over 60 years versus 17% in patients under 60 years [80]. Full-thickness tears were more likely to progress than partial-thickness tears [80]. Approximately 50% of asymptomatic tears have a significant increase in size at a median time of 2.8 years [80]. Full-thickness tears are more likely to enlarge, become painful, and progress to muscle degeneration compared with partial-thickness tears [92]. An increase in tear size was associated with symptoms in asymptomatic shoulders [80]. Tears that became symptomatic over time significantly increased in size, while tears that did not become symptomatic did not increase in size [80].
Degenerative rotator cuff tears initiate approximately 13 to 17 mm posterior to the long head of the biceps tendon [92]. The area around 15 mm posterior to the biceps tendon is the most frequently involved location for degenerative rotator cuff tear initiation [92]. This initiation area is within the "rotator crescent" tissue, which is thinner and more avascular than the "rotator cable" [92]. Tears involving the anterior portion of the supraspinatus may need earlier surgical intervention due to greater rates of fatty infiltration [80]. Tears not involving but close to the anterior cable may need to be more closely monitored if treated nonoperatively [80]. Larger, symptomatic tears involving the infraspinatus had increased superior migration compared with asymptomatic, smaller tears [80]. A critical tear area of 175 mm² (approximately 15 mm × 12 mm) was associated with proximal humeral migration [80]. Normal glenohumeral kinematics may be disrupted by larger rotator cuff tears, leading to proximal humeral migration [80].
The empty can test has a sensitivity of 71.7% and a specificity of 64.6% for full-thickness supraspinatus tears [71]. The lift-off and belly-press tests have high specificity but low sensitivity for full-thickness subscapularis tears [71]. Patients with an external rotation lag sign at the side likely have a large posterosuperior tear involving the infraspinatus [71]. A positive hornblower sign suggests a massive posterosuperior cuff tear that prohibits the active positioning of the hand in space [71]. The painful arc test has a sensitivity of 71% (95% CI 60-83) and specificity of 81% (95% CI 68-93) for rotator cuff disease [71]. The cross-body adduction test has a sensitivity of 75% (95% CI 64-85) and specificity of 61% (95% CI 46-76) for rotator cuff disease [71]. The Hawkins test has a sensitivity of 76% (95% CI 56-89) and specificity of 48% (95% CI 23-74) for rotator cuff disease [71]. The Neer test has a sensitivity of 64-68% and specificity of 30-61% for rotator cuff disease [71]. The Yocum test has a sensitivity of 79% (95% CI 61-97) and specificity of 40% (95% CI 10-70) for rotator cuff disease [71]. Passive abduction has a sensitivity of 74% (95% CI 54-93) and specificity of 10% (95% CI 0-29) for rotator cuff disease [71]. The external rotation lag test has a sensitivity of 47% (95% CI 21-71) and specificity of 94% (95% CI 85-100) for full-thickness rotator cuff tears [71]. The internal rotation lag test has a sensitivity of 97% (95% CI 88-100) and specificity of 83% (95% CI 70-96) for full-thickness rotator cuff tears [71]. The drop arm test has a sensitivity of 24% (95% CI 13-34) and specificity of 93% (95% CI 85-100) for rotator cuff disease [71]. The dropping sign has a sensitivity of 73% (95% CI 51-95) and specificity of 77% (95% CI 62-92) for full-thickness rotator cuff tears [71]. The Gerber (lift-off test) has a sensitivity of 34-68% and specificity of 50-77% for rotator cuff disease [71]. External rotation resistance has a sensitivity of 63% (95% CI 49-77) and specificity of 75% (95% CI 69-82) for rotator cuff disease [71]. The full can test has a sensitivity of 75% (95% CI 64-85) and specificity of 68% (95% CI 54-83) for rotator cuff disease [71]. The Patte test has a sensitivity of 58% (95% CI 36-80) and specificity of 60% (95% CI 30-90) for rotator cuff disease [71]. The empty can (Jobe) test has a sensitivity of 71% (95% CI 49-86) and specificity of 49% (95% CI 42-56) for rotator cuff disease [71]. Resisted abduction has a sensitivity of 58% (95% CI 36-80) and specificity of 20% (95% CI 0-45) for rotator cuff disease [71]. The combination of Hawkins and Neer tests (both positive) has a sensitivity of 78% (95% CI 66-90) and specificity of 50% (95% CI 22-78) for rotator cuff disease [71].
The long head of the biceps tendon (LHBT) has been implicated in intra-articular shoulder pathology [96]. Painful LHBT tendinitis may ensue from tears about the rotator interval or with any chronic inflammatory pathology of the glenohumeral joint [96]. Clinical tests for LHBT pathology, including O’Brien, Yergason, Speed, and direct palpation tests, have limited specificity [96]. A history of radiating anterior shoulder pain may inform the examiner of pain generation from the LHBT [96]. MRI and ultrasonography are tools to evaluate biceps pathology [96]. Arthroscopic examination is limited to the intra-articular LHBT and proximal groove, missing less common distal biceps groove lesions [96]. Isolated traumatic LHBT tears are generally treated nonsurgically [96]. Arthroscopic tenotomy is acceptable for less physically demanding individuals who may tolerate deformity [96]. Tenotomy results in cosmetic deformity (Popeye) about 30% of the time [96]. Vigorous activity may result in cramping pain of the biceps muscle belly after tenotomy [96]. Arthroscopic suprapectoral tenodesis may be performed for SLAP tears or in conjunction with rotator cuff repair in patients needing full supination strength and endurance [96]. Open or arthroscopic-assisted subpectoral tenodesis are options if biceps groove pathology is a concern [96].
Imaging plays an important role in the workup of a patient with suspected rotator cuff abnormality [24]. The goal of diagnostic imaging is to determine the presence, size, and orientation of the rotator cuff tear [71]. Diagnostic imaging is used to evaluate the healing capacity of the tendon [71]. Diagnostic imaging is used to assess associated pathology such as long head biceps tendinitis, acromioclavicular joint pathology, and arthrosis [71]. Ultrasonography approaches the sensitivity and specificity of MRI for detecting the presence of a full-thickness rotator cuff tear with an experienced practitioner [71]. Ultrasonography is relatively inexpensive, allows for dynamic testing, guided injections, and immediate feedback [71]. MRI accurately assesses muscle, bone, and cartilage, which has advantages for surgical planning [71]. MRI continues to be the imaging modality of choice for most providers, with ultrasonography becoming common in certain centers [71]. Ultrasonography is more accurate for full-thickness rotator cuff tears and is comparable to MRI [22]. Ultrasonography has diagnostic performance and reliability for fatty degeneration of the rotator cuff muscles [23].
Patients can generally be divided into three main categories for rotator cuff tear management: those needing urgent or early operative repair, those benefiting from a trial of conservative treatment, and those best suited for nonoperative treatment [6]. Clinical decision-making for the management of rotator cuff tears is complex and lacks consensus among orthopedic surgeons [6]. The American Academy of Orthopaedic Surgeons clinical practice guidelines do not provide guidance on the management of rotator cuff tears [6]. Cochrane systematic reviews do not provide guidance on the management of rotator cuff tears [6].
Investigations¶
Imaging plays an important role in the workup of a patient with suspected rotator cuff abnormality [24].
Plain radiography: Radiographic views of the subacromial space, such as the supraspinatus outlet view, may show spurring on the undersurface of the acromion causing narrowing of the subacromial space [51]. Chronic rotator cuff disease may demonstrate superior migration of the humeral head with extensive degenerative change on imaging [59, 60]. Classic changes within the acromion or coracoacromial ligament, including spurring and calcification, may be demonstrated on imaging [59, 60]. Cystic changes within the greater tuberosity may be present on imaging [59, 60]. The Hamada classification is a commonly used scheme that uses a mechanistic approach to explain radiographic changes seen with chronic massive rotator cuff tears, highlighting progressive nature leading to cuff tear arthropathy [28]. Irreparable tears are more likely to occur when the acromiohumeral distance appears shorter than 7 mm on AP radiograph [59, 60]. Cuff repair should be performed before acromiohumeral interval narrowing [129].
MRI: MRI is used to define the extent of tear, degree of tear retraction, and presence of muscular atrophy [59, 60]. MRI allows characterization of the location, size, and amount of retraction of the rotator cuff tear, as well as the degree of atrophy and fatty infiltration of the rotator cuff musculature [57]. MRI is key for evaluating fatty infiltration, although the Goutallier classification was originally based on CT [59, 60]. The Goutallier classification for fatty infiltration grades muscle from 0 (normal) to 4 (more fat than muscle), with grades 3 and 4 indicating long-term chronic tears with higher potential for surgical failure [57]. MR imaging-derived rotator cuff muscle proton density fat-fraction (PDFF) is associated with isometric strength independent of muscle atrophy and tendon rupture in shoulders with early and advanced degenerative changes [36]. Routine MRI assessment of the upper subscapularis muscle and coracohumeral distance can contribute to the diagnostic accuracy of subscapularis tears [118]. Higher upper subscapularis Goutallier grade and coracohumeral distance narrowing are predictive of subscapularis tears in patients undergoing arthroscopic rotator cuff repair [118]. The tangent sign is defined as failure of the supraspinatus muscle belly to cross a line from the superior border of the coracoid to the superior border of the scapular spine [59, 60]. The tangent sign correlates with muscle atrophy and fatty infiltration of the supraspinatus [59, 60]. Patients with a positive tangent sign are more likely to have an irreparable rotator cuff tear [21, 59, 60]. A positive tangent sign predicts the repairability of rotator cuff tears [21].
Ultrasonography: Ultrasonography is more accurate for full-thickness rotator cuff tears and is comparable to MRI [22]. Diagnostic accuracy of ultrasound for rotator cuff tears has been reviewed, comparing sensitivities and specificities with MRI [22]. Ultrasonography is increasing in popularity as a tool for diagnosis of rotator cuff disease and for confirmation of intraarticular or subacromial location of injections [59, 60]. Ultrasonography is used to assess the structural status of rotator cuff tendons after arthroscopic repair at 6 months postoperatively [39]. Ultrasonography is used to assess diagnostic performance and reliability for fatty degeneration of the rotator cuff muscles [23].
Other Considerations: Large critical shoulder angle (CSA greater than 38°) and acromial index (AI greater than 0.7) are associated with higher retear rates after arthroscopic rotator cuff repair [11]. The critical shoulder angle (CSA) is a static measure that does not change over time, though differences are small and depend on excellent radiographic technique [12]. Critical shoulder angle and acromial index do not influence 24-month functional outcome after arthroscopic rotator cuff repair [13]. Clinical assessment of physical examination maneuvers for rotator cuff lesions includes evaluation of tear repairability [20]. The societal and economic value of rotator cuff repair is a recognized consideration in the workup and treatment planning [13]. Prevalence and risk factors of a rotator cuff tear in the general population are relevant to the epidemiology of the disease [13]. The demographic and morphological features of rotator cuff disease differ between asymptomatic and symptomatic shoulders [13]. The natural history of asymptomatic rotator cuff tears involves potential progression, with symptomatic progression rates studied via clinical and sonographic variables [13]. The natural history of full-thickness rotator cuff tears shows that symptoms improve over the first year after treatment but then plateau, representing a regression to the mean [13]. Tear progression of symptomatic full-thickness and partial-thickness rotator cuff tears correlates with presenting tear size [15]. Abnormal findings on magnetic resonance images are common in asymptomatic shoulders [15]. Evidence for genetic variations and inherited predisposition contributes to the risk for rotator cuff disease [14, 15]. Genome-wide association studies have identified single-nucleotide polymorphisms associated with full-thickness rotator cuff tears [15]. Individual scapular anatomy, measured by the critical shoulder angle, shows statistically significant differences between asymptomatic individuals, those with osteoarthritis, and patients with full-thickness rotator cuff tears [15]. Symptoms of pain do not correlate with rotator cuff tear severity in patients with symptomatic atraumatic full-thickness tears [15]. Patient-reported outcomes and pain are not correlated with rotator cuff healing on ultrasonography or MRI [61]. Postoperative strength is better in individuals with healed rotator cuffs versus those with defects after repair [61]. Poor interobserver agreement regarding postoperative graft and rotator cuff integrity by MRI was found in studies of superior capsular reconstruction [115].
Treatment¶
Non-Operative¶
Non-surgical treatment is the preferred initial approach for patients with non-traumatic rotator cuff injuries [78]. Most partial-thickness rotator cuff tears are also best managed initially with nonoperative treatment, reserving surgical intervention (repair or debridement) for cases where conservative measures fail [17]. For patients with massive irreparable rotator cuff tears, clinicians should assess across all identified domains and target modifiable factors with interventions [2]. While one-year follow-up appears clinically sufficient for short-term outcomes, as 1-year and 2-year results are similar [1], it does not determine long-term success; long-term outcomes must be evaluated separately [4].
Operative¶
Indications: Patient-specific risk factors influencing outcomes include age, expectations, and tear extent [5]. Patients aged 75 years or older achieve early outcomes after arthroscopic repair similar to younger patients when proper indications are met [32]. Severely obese patients achieve excellent overall outcomes and noninferior clinical differences compared to healthy-weight patients [23]. Stiff shoulders undergoing one-stage repair show comparable range of motion, clinical outcomes, and retear rates to non-stiff shoulders [99].
Contraindications to reverse total shoulder arthroplasty (RTSA) include severely impaired deltoid function, isolated supraspinatus tears, and the presence of full active shoulder elevation despite a massive rotator cuff tear and arthritis [101]. Patients with previous rotator cuff repair are considered high-risk for reverse shoulder arthroplasty due to an increased risk of periprosthetic joint infection [43].
Surgical Approach / Technique: Arthroscopic repair is the preferred method for many surgeons due to advantages over open techniques, including more thorough visualization, diagnosis, and treatment of intra-articular lesions [84]. It allows comprehensive assessment of pathology and tear configuration from multiple angles and facilitates tendon mobilization via precise adhesion releases [84]. Arthroscopic repair minimizes deltoid injury, preserves the acromial deltoid origin, eliminates deltoid dehiscence risk, and reduces postoperative pain through less soft tissue trauma [84]. Anatomic footprint restoration is achievable with suture anchors, approximating open transosseous repairs [84].
The double-row technique uses two rows of anchors (medial and lateral) for additional fixation and footprint coverage [84]. Newer techniques use a medial row with sutures passed to a lateral row to compress the tendon to bone [84]. Biomechanical studies show double-row repair outperforms single-row in failure strength [84]. Controlled laboratory studies confirm double-row superiority in initial and ultimate failure strength, decreased gap formation, decreased strain/suture cut-through, and improved vascularity in transosseous-equivalent repairs [31]. However, imaging shows no significant difference in cuff integrity between single-row and double-row groups at 6-month and minimum 2-year follow-up for any tear size [41].
Rip-stop fixation constructs for large/massive tears yield a 53% healing rate versus 11% for single-row repair [29]. Knotted and knotless double-row transosseous equivalent techniques demonstrate comparable postoperative outcomes, making both knotted suture bridge (KSB) and knotless suture bridge (KTB) viable options [65]. The repair construct does not appear to influence re-tear pattern [37]. Intraoperative bone channeling did not demonstrate superiority over standard repair at 24 months [64]. Routine arthroscopic suprascapular nerve release is not recommended for rotator cuff tears [72]. Traditional and modified anterolateral acromioplasty during arthroscopic repair significantly improves shoulder joint function in total tears [70].
Arthroscopic repair yields similar outcomes and failure rates to open or mini-open repair, with decreased short-term pain and faster return to activity [31]. In patients >50 years with degenerative tears, there is no difference in clinical or cost-effectiveness between open and arthroscopic repair at 2 years [16]. Re-tear rates were not significantly different between arthroscopic (46.4%) and open (38.6%) groups in this population [16]. A level I trial found no clinically important differences in Constant score, VAS pain, or satisfaction among physiotherapy only, acromioplasty plus physiotherapy, and arthroscopic repair groups at 2 years [16].
Mini-open repair allows direct assessment of tear nature, tissue quality, and ease of restoration to the insertion site [104]. The transosseous technique is simple, expeditious, avoids suture anchor issues, and enables finding strong bone for suture hold [104]. Creating a trough for tendon insertion increases surface area, stimulates stem cells/growth factors, excludes joint fluid, and places sutures laterally to avoid coracoacromial arch impingement [104]. Achieving a biomechanically stable construct is critical for biologic healing in arthroscopic transosseous repair [30].
Implant Selection: MgF2-coated biodegradable magnesium alloy suture anchors are feasible for rotator cuff repair [122].
Adjuncts: Intra-articular tranexamic acid (TXA) during arthroscopic repair provides superior visual clarity, significantly shortened operative duration, and superior pain management at 8 and 24 hours postoperatively compared with placebo [113].
Graft Augmentation and Biologics: Initial graft augmentation reports show clinical improvements that may change treatment approaches [8]. Augmentation provides mechanical stability and improved biology for large-to-massive or chronic tears with poor tissue quality [126]. Arthroscopic replacement of massive, irreparable tears using GraftJacket allograft may decrease pain and increase function [112]. PRP use remains controversial; long-term evidence is needed to justify its use [87]. At minimum 2-year follow-up, primary arthroscopic repair with bovine collagen implant augmentation resulted in greater reoperation rates for inflammation/stiffness without benefit in patient-reported outcomes compared to no implant [124].
Pain Management: Multimodal analgesia should be individualized based on surgical location, complexity, and comorbidities [74]. Interscalene block is preferred for complex anterior procedures unless respiratory comorbidities exist, in which case periarticular infiltration with pharmacologic therapies is recommended [74]. Strategies like ISBPB-plus can reduce opioid requirements [93]. Gabapentin is supported as an adjunct for pain management in open repair [97]. Buprenorphine patches showed no clinically important advantages in pain or function after arthroscopic repair [111].
Postoperative Management: There was a slightly higher healing rate in the delayed physical therapy group (91%) versus early therapy (85%), suggesting potential benefit in avoiding early passive range of motion [114]. Eight weeks of immobilization did not yield higher healing rates for medium-sized tears compared to four weeks [128]. Surgeons must provide detailed postoperative instructions to patients [7]. Appreciating the multifactorial nature of repair is imperative for success, reducing failure, and optimizing function [33].
Revision: Revision rotator cuff repair provides significant pain relief and functional improvement at long-term follow-up (minimum 10 years) [121].
Long-Term Outcomes: At long-term follow-up (≥15 years), all-arthroscopic repair shows significant improvement from baseline preoperative function, with outcomes remaining durable over 15 years [3]. Long-term outcomes from primary tendon repair remained superior to physiotherapy up to 15 years for small-to-medium tears [27].
Complications¶
Long-term Outcomes and Structural Integrity: One-year follow-up is insufficient to determine long-term outcomes of rotator cuff repair, as patients must live with long-term surgical outcomes [4]. Patient-reported outcomes show degradation of improvement after 1-year follow-up, with no clinically significant increase in SANE scores after 1 year postoperatively [35]. Long-term follow-up (≥15 years) for all-arthroscopic rotator cuff repair shows significant improvement from baseline preoperative function that remains durable over 15 years [3]. Long-term outcomes of arthroscopic and open/mini-open rotator cuff repairs demonstrate sustained improvement in shoulder scores and pain, but with a substantial retear rate associated with inferior shoulder function [130]. The highest retear rate after arthroscopic rotator cuff repair occurs from 6 weeks to 3 months after surgery, with equivalent rates within 6 weeks and from 3 months to 6 months after surgery [133].
Specific Repair Scenarios: Arthroscopic in situ repair of partial-thickness rotator cuff tears produces excellent functional outcomes in more than 80% of patients with low revision rates during long-term follow-up [9]. Arthroscopic repair of massive rotator cuff tears has a high rate of healing failures but provides functional gain at midterm follow-up [18]. Arthroscopic partial repair of irreparable rotator cuff tears is effective for improving shoulder function and decreasing pain, despite a high repair failure rate of 41.6% [132]. Arthroscopic revision rotator cuff repair for failed open or arthroscopic repair improves shoulder function, although retears are frequent but usually smaller [141].
Timing and Risk Factors: Delaying rotator cuff surgery for 3 to 6 months does not lead to higher retear rates or inferior patient-reported outcomes compared with earlier surgery, but delaying for 1 year or more results in higher retear rates [138]. Bacterial contamination from sutures may contribute to impaired healing or retear after rotator cuff repair, even with arthroscopic techniques [139]. Lower socioeconomic status is correlated with worse outcomes after arthroscopic rotator cuff repair, although no differences were appreciated between cohorts regarding reoperation or complications [136].
Other Considerations: Patients with previous rotator cuff repair are at increased risk of revision surgery for periprosthetic joint infection after reverse shoulder arthroplasty [43]. Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears in patients younger than 65 years old has a high complication rate, although most can be treated successfully without compromising clinical outcome [142]. Venous thromboembolism is a possible risk associated with routine, elective arthroscopic surgeries in the setting of COVID-19 [135].
Recovery¶
Light activity (weeks): Patients can safely return to driving at 2 weeks postoperatively, with no clinically important negative impact on driving fitness observed [77]. Desk work and light activities of daily living are typically resumed within this early postoperative window, as pain, range of motion, muscle strength, and function significantly improve regardless of early rehabilitation protocols [68].
Full activity (months): The majority of injured workers return to previous work at approximately 8 months after surgery [12]. As much as 88.5% of patients return to activities with a mean duration of 6.59 months [79]. Most golf players return to golf at 1 year after arthroscopic rotator cuff repair [125]. Patients who continued to work after injury but presurgery are the most likely to return to work at any level [81]. Patients with less strenuous preinjury levels of work are the most likely to return to their preinjury levels at six months post-repair [81].
Complete recovery / outcome plateau (months): The plateau of maximum recovery following arthroscopic rotator cuff repair occurred at 1 year, with high satisfaction rates at all time points [63]. One-year follow-up appears clinically sufficient for rotator cuff repair outcomes, as 1-year and 2-year outcomes are clinically similar [1]. Both patient-reported outcomes and achievement of clinically significant outcomes show small differences at 1 and 2 years after arthroscopic rotator cuff repair [11]. There is no clinically significant increase in SANE scores after 1 year postoperatively, with degradation of outcome improvement observed after the 1-year follow-up [35]. The widely accepted 2-year benchmark for rotator cuff repair outcomes may be arbitrary and does not add clinical relevance [1]. However, one-year follow-up does not determine rotator cuff repair long-term outcomes, and authors are obliged to evaluate long-term outcomes because patients live with them [4]. At long-term follow-up (≥15 years), patient-reported outcomes of all-arthroscopic rotator cuff repair show significant improvement from baseline preoperative function and remain durable [3]. Long-term outcomes from primary tendon repair remained superior to physiotherapy up to 15 years of follow-up for small-to-medium-sized rotator cuff tears [27]. At 10 years, differences in outcome between primary tendon repair and physiotherapy for small and medium-sized rotator cuff tears had increased, with better results for primary tendon repair [56]. Early high functional scores after primary rotator cuff repair or reconstruction did not persist at 16 years; function was lost as ROM and strength decreased to less than preoperative values [91].
Rehabilitation protocol: Early strength assessment was significantly associated with clinical recovery in patients undergoing rotator cuff repair [76]. The implementation of an accelerated, independent, exercise protocol reduced physical therapy utilization to levels below national best-practices benchmarks without negatively affecting impairment or disability rates in Workers' Compensation patients undergoing mini-open rotator cuff repair [82]. Consideration of the multifactorial nature of rotator cuff repair is imperative for a successful outcome, including reducing the rate of failure and optimizing return to function [33].
Functional milestones: Arthroscopic in situ repair of partial-thickness rotator cuff tears produces excellent functional outcomes in more than 80% of patients during long-term follow-up, with low revision rates [9].
Key Evidence¶
- [L5] The widely accepted 2-year benchmark for rotator cuff repair outcomes may be arbitrary and does not add clinical relevance, as 1-year follow-up appears clinically sufficient. [1] (10.1016/j.arthro.2023.11.002)
- [L5] Clinicians assessing patients with massive irreparable rotator cuff tears should assess across all identified domains and target modifiable factors with interventions. [2] (10.1186/s12891-024-07872-6)
- [L4] At long-term follow-up (≥15 years), the patient-reported outcomes of all-arthroscopic rotator cuff repair show significant improvement from baseline preoperative function and remain durable over a period of 15 years. [3] (10.1016/j.jse.2022.01.116)
- [L5] One-year follow-up is not the last word for rotator cuff repair outcomes; patients must live with the long-term outcomes of surgical procedures, and authors are obliged to evaluate these long-term outcomes. [4] (10.1016/j.arthro.2024.12.040)
- [L1] Evidence synthesized in this review underscores the importance of patient age, expectations, and the extent of the rotator cuff tear in influencing outcomes following rotator cuff repair. [5] (10.1186/s12891-025-08608-w)
- [L4] These results emphasize the need for orthopedic surgeons to provide detailed and informative instructions to patients undergoing rotator cuff repair, especially in the postoperative setting. [7] (10.1016/j.jse.2023.04.021)
- [L5] Despite little evidence of drastic outcome improvements in arthroscopic rotator cuff repair over the last 30 years, initial reports of graft augmentation demonstrate clinical improvements that could significantly change treatment approaches. [8] (10.1016/j.arthro.2021.11.035)
- [L4] During long-term follow-up, arthroscopic in situ repair of partial-thickness rotator cuff tears produces excellent functional outcomes in more than 80% of patients, and revision rates are low. [9] (10.1016/j.arthro.2018.09.026)
- [Paper] This issue reinforces the concept that rotator cuff disease is a continuum and brings readers up to date on rotator cuff disease, covering epidemiology, imaging, techniques, and outcomes. [10] (10.1016/j.csm.2012.08.001)
- [L4] Both patient-reported outcomes and achievement of clinically significant outcomes show small differences at 1 and 2 years after rotator cuff repair. [11] (10.1016/j.arthro.2023.09.024)
- [L4] The majority of injured workers undergoing rotator cuff repair return to previous work at approximately 8 months after surgery. [12] (10.1177/0363546520975426)
- [L4] Arthroscopic rotator cuff repair demonstrates significant improvement in clinical outcomes and good rate of healing by postoperative ultrasound. [14] (10.1016/j.jse.2008.11.018)
- [L4] Despite a high rate of healing failures, arthroscopic repair can be recommended in patients with massive rotator cuff tears because of the functional gain at midterm follow-up. [18] (10.1177/0363546513485719)
- [L4] Understanding predisposing factors assists in predicting the prognosis of the repaired rotator cuff. [20] (10.1016/j.jse.2014.06.050)
- [L3] The etiology of the rotator cuff tear did not significantly affect postoperative outcomes or healing rates. [22] (10.1186/s12891-023-06174-7)
- [L3] Severely obese patients and their associated comorbid conditions pose unique challenges in rotator cuff tear management, but they still achieve overall excellent outcomes after repair and noninferior clinical differences when compared to healthy weight patients. [23] (10.1016/j.arthro.2022.02.026)
- [Paper] Imaging plays an important role in the workup of a patient with suspected rotator cuff abnormality. [24] (10.1016/j.csm.2012.07.010)
- [L3] Most patients achieved clinically significant outcomes for the PROMIS-UE within 12 months of rotator cuff repair. [25] (10.1177/23259671231157038)
- [L1] Long-term outcomes from primary tendon repair remained superior to physiotherapy up to 15 years of follow-up, supporting its use as the primary treatment for small-to-medium-sized rotator cuff tears. [27] (10.2106/jbjs.24.00065)
- [L5] The Hamada classification is a commonly used classification scheme that uses a mechanistic approach to explain the radiographic changes seen with chronic massive rotator cuff tears, highlighting the progressive nature of massive rotator cuff tears leading to CTA. [28] (10.1007/s11999-017-5340-7)
- [L5] The technique has been associated with a 53% healing rate of large and massive rotator cuff tears, compared with only 11% healing when using single-row repair. [29] (10.1016/j.arthro.2023.06.013)
- [L5] Achieving a biomechanically stable construct is critical to biologic healing, and experienced arthroscopic surgeons are reporting results equal to those of open rotator cuff repair. [30] (10.5435/jaaos-d-22-00057)
- [L5] Recent research shows that similar early outcomes can be expected after arthroscopic rotator cuff repair in patients 75 years or older compared to a propensity-matched group under age 75 years, with proper patient selection being vital. [32] (10.1016/j.arthro.2023.12.023)
- [L5] The purpose of this review is to explore the evidence that suggests consideration and appreciation of a rotator cuff repair's multifactorial nature is imperative for a successful outcome; this includes reducing the rate of failure and optimizing return to function. [33] (10.1016/j.xrrt.2021.04.009)
- [L4] Patients achieve significant and comparable improvements in functional outcomes following rotator cuff repair at 2 years postoperatively without the use of augmentation, regardless of their predicted risk of repair failure based on the RoHI score. [34] (10.1016/j.jisako.2025.101026)
- [L3] The study aims to demonstrate degradation of outcome improvement in patient-reported outcomes after 1-year follow-up of rotator cuff repair, hypothesizing no clinically significant increase in SANE scores after 1 year postoperatively. [35] (10.1177/2325967124s00116)
- [L3] MR imaging–derived RC muscle PDFF is associated with isometric strength independent of muscle atrophy and tendon rupture in shoulders with early and advanced degenerative changes. [36] (10.1177/0363546517703086)
- [L3] Repair construct used during rotator cuff repair does not appear to influence re-tear pattern. [37] (10.1016/j.jseint.2024.06.007)
- [L4] The structural status of rotator cuff tendons after arthroscopic repair can be assessed at 6 months postoperatively. [39] (10.1016/j.jse.2011.05.027)
- [L2] However, the imaging results showed no significant difference in cuff integrity in both groups in patients with any tear size at 6-month and minimum 2-year follow-up. [41] (10.1016/j.arthro.2011.07.003)
- [L3] Patients with previous rotator cuff repair should be regarded as high-risk patients when considering reverse shoulder arthroplasty. [43] (10.1016/j.jse.2022.07.001)
- [L3] Glenohumeral decentering is significantly associated with diminished shoulder function and active range of motion in all planes. [52] (10.1016/j.jse.2025.03.038)
- [L4] At mid-term follow-up, greater preoperative rotator cuff disease severity was associated with failure to achieve clinically significant outcomes. [53] (10.1016/j.arthro.2023.06.031)
- [L5] In a dynamic biomechanical cadaveric model, increased glenohumeral joint loads due to a full-thickness SSP tear can be reversed with RCR. [55] (10.1016/j.arthro.2021.10.036)
- [L1] At 10 years, the differences in outcome between primary tendon repair and physiotherapy for small and medium-sized rotator cuff tears had increased, with better results for primary tendon repair. [56] (10.2106/jbjs.18.01373)
- [L3] Diagnostic performance of the modified Patte classification system was excellent for reparability and acceptable for rotator cuff healing, with high measurement reliability. [58] (10.1002/ksa.12162)
- [L4] The plateau of maximum recovery following rotator cuff repair occurred at 1 year with high satisfaction rates at all time points. [63] (10.1016/j.arthro.2017.04.033)
- [L1] This trial did not demonstrate the superiority of intraoperative bone channeling in rotator cuff repair over standard rotator cuff repair at 24 months postoperatively. [64] (10.1177/03635465221138562)
- [L3] Both KSB and KTB techniques are viable options for achieving a successful rotator cuff repair. [65] (10.1007/s00167-022-07121-0)
- [L2] Pain, range of motion, muscle strength, and function all significantly improved after arthroscopic rotator cuff repair, regardless of early postoperative rehabilitation protocols. [68] (10.1016/j.arthro.2011.07.012)
- [L3] Traditional and modified anterolateral acromioplasty while treating total rotator cuff tears using arthroscopic rotator cuff repair significantly improves shoulder joint function. [70] (10.1186/s12891-024-07619-3)
- [L1] Routine arthroscopic SSNR is not recommended when treating patients with rotator cuff tear. [72] (10.1007/s00167-022-07066-4)
- [L5] Multimodal analgesia for rotator cuff repair should be individualized based on surgical location, complexity, and patient comorbidity, with interscalene block preferred for complex anterior procedures unless respiratory comorbidities are present, in which case periarticular infiltration combined with pharmacologic therapies is recommended. [74] (10.1016/j.arthro.2024.06.010)
- [L2] Early strength assessment was significantly associated with clinical recovery in patients undergoing rotator cuff repair. [76] (10.1016/j.jse.2025.07.010)
- [L2] Patients showed no clinically important negative impact on driving fitness as early as 2 weeks after rotator cuff repair. [77] (10.2106/jbjs.21.01436)
- [L3] Additionally, non-surgical treatment is recommended as the preferred approach for patients with non-traumatic rotator cuff injuries. [78] (10.1186/s13018-024-04858-x)
- [L1] As much as 88.5% of patients were able to return to activities after arthroscopic rotator cuff repair with a mean duration of 6.59 months. [79] (10.1177/2325967121s00867)
- [L3] Six months after rotator cuff repair, patients who continued to work after injury but presurgery were the most likely to return to work at any level, and patients who had less strenuous preinjury levels of work were the most likely to return to their preinjury levels of work. [81] (10.1177/03635465231152479)
- [L4] The implementation of an accelerated, independent, exercise protocol reduced physical therapy utilization to levels below national best-practices benchmarks without negatively affecting impairment or disability rates in Workers' Compensation patients undergoing mini-open rotator cuff repair. [82] (10.1016/j.jse.2012.05.022)
- [L5] Partial rotator cuff repair can provide a respectable outcome and comparable clinical results to complete repair for large to massive tears, particularly when complete repair is not possible or cost limitations prohibit augmentation. [86] (10.1016/j.arthro.2025.01.003)
- [L5] Use of PRP for augmentation of arthroscopic rotator cuff repair remains an interesting but controversial option; long-term evidence must justify its use before it can be permanently included in the armament of shoulder surgeons. [87] (10.1016/j.arthro.2021.06.035)
- [L3] Shoulder stiffness at 3 months post-ARCR predicts 12-month shoulder stiffness but indicates better tendon integrity, with limited long-term clinical impact. [88] (10.1016/j.arthro.2024.01.038)
- [L5] Recent research indicates that shoulder stiffness after rotator cuff repair is beneficial rather than detrimental, as it correlates with a higher likelihood of an intact repair at 6 months, with most stiffness eventually resolving. [89] (10.1016/j.arthro.2024.02.038)
- [L4] The early high functional scores after primary rotator cuff repair or reconstruction did not persist; function was lost as ROM and strength decreased to less than preoperative values. [91] (10.1007/s11999-010-1403-8)
- [L5] Multiple factors, including multimodal anesthesia strategies like the ISBPB-plus technique, can reduce opioid requirements after rotator cuff repair, though the optimal strategy has yet to be determined. [93] (10.1016/j.arthro.2024.09.017)
- [L2] Preoperative restriction of range of motion for the hand behind the back best predicts shoulder stiffness at 6 weeks postoperatively. [95] (10.1097/01.blo.0000137564.27841.27)
- [L1] The study supports the use of gabapentin as an adjunct for pain management in open rotator cuff repair. [97] (10.1016/j.jse.2024.08.044)
- [L4] One-stage treatment for rotator cuff tears in stiff shoulders provides comparable range of motion and patient-reported clinical outcomes as rotator cuff repair for non-stiff shoulders. [99] (10.1186/s13018-023-04104-w)
- [L2] Infraspinatus muscle contractility was the most important factor for better postoperative outcomes. [100] (10.1016/j.jisako.2025.100817)
- [L5] Severely impaired deltoid function, an isolated supraspinatus tear, and the presence of full active shoulder elevation with a massive rotator cuff tear and arthritis are contraindications to RTSA. [101] (10.1007/s11999-009-1188-9)
- [L5] Due to the ongoing changes in mechanics, collagen organization and histology in the detached supraspinatus tendon compared to control animals at 16 weeks, this model may be useful for understanding the human chronic tendon tear. [103] (10.1007/s11999-009-1206-y)
- [L3] Higher baseline grip strength predicts more favorable postoperative shoulder function following ARCR. [106] (10.1186/s13018-024-04750-8)
- [L3] Shoulder function correlated negatively with FDI at baseline and at last follow-up. [108] (10.1016/j.jse.2008.11.006)
- [L1] In this randomized trial, we found no clinically important advantages in pain or function to the use of buprenorphine patches after arthroscopic rotator cuff repair, and insufficient evidence exists to confirm whether the minor differences in transient side effects could justify the use of a new and largely untested analgesic approach in this context. [111] (10.1097/corr.0000000000003303)
- [L4] This treatment option may provide patients with decreased pain and increased function despite a previously irreparable rotator cuff tear. [112] (10.1016/j.arthro.2007.07.033)
- [L1] Intra-articular use of TXA during arthroscopic rotator cuff repair provided superior arthroscopic visual clarity, significantly shortened operative duration, and provided superior pain management in the first 8 and 24 hours postoperatively compared with placebo. [113] (10.1016/j.jse.2022.10.007)
- [L1] There was a slightly higher rotator cuff healing rate in the delayed group (91% vs 85%), suggesting a potential benefit to avoiding early passive range of motion. [114] (10.1016/j.jse.2012.01.025)
- [L4] Poor interobserver agreement regarding postoperative graft and rotator cuff integrity by MRI was found. [115] (10.1016/j.arthro.2021.11.008)
- [L3] Routine MRI assessment of the upper subscapularis muscle and coracohumeral distance can contribute to the diagnostic accuracy of subscapularis tears and offer valuable information regarding the severity of such tears. [118] (10.1016/j.arthro.2023.10.017)
- [L4] Revision rotator cuff repair provides significant pain relief and improvement in functional scores at long-term follow-up. [121] (10.1016/j.jse.2023.06.009)
- [L5] The findings indicate that MgF2-coated suture anchors are feasible for rotator cuff repair and potentially other orthopedic applications. [122] (10.1186/s12891-024-07300-9)
- [L3] At minimum 2-year follow-up, patients undergoing primary arthroscopic rotator cuff repair with bovine collagen implant augmentation had a greater proportion of reoperation due to inflammation and stiffness compared with patients who did not receive the implant, with no benefit in patient-reported outcomes. [124] (10.1097/corr.0000000000003247)
- [L3] The golfing return rate after arthroscopic rotator cuff repair was higher than expected (73.6%) and most players returned at 1 year after surgery. [125] (10.1016/j.jseint.2022.12.005)
- [L5] Augmentation can provide mechanical stability and improved biology to improve the likelihood of a successful repair in patients with large-to-massive rotator cuff tears or chronic tears with poor tissue quality. [126] (10.5435/jaaos-d-23-00101)
- [L1] Eight weeks of immobilization did not yield a higher rate of healing of medium-sized rotator cuff tears compared with four weeks of immobilization. [128] (10.2106/jbjs.l.01741)
- [L3] Cuff repair should be performed before acromiohumeral interval narrowing. [129] (10.1007/s11999-011-1896-9)
- [L4] Pooled analysis demonstrated sustained improvement in long-term shoulder scores and pain with a substantial retear rate in both groups, which was associated with inferior shoulder function. [130] (10.1177/03635465211073332)
- [L4] Arthroscopic partial repair of irreparable RCTs is an effective treatment to improve the shoulder function and decrease the pain, despite the high repair failure rate of 41.6%. [132] (10.1016/j.arthro.2017.06.047)
- [L3] The highest retear rate after arthroscopic rotator cuff repair was observed from 6 weeks to 3 months after surgery, with equivalent rates within 6 weeks and from 3 months to 6 months after surgery. [133] (10.1016/j.jse.2023.01.026)
- [L4] This case report serves to make orthopedic surgeons aware of the possible risk factors for venous thromboembolic events associated with routine, elective arthroscopic surgeries in the setting of the COVID-19 pandemic. [135] (10.1016/j.jse.2021.02.003)
- [L3] However, no differences were appreciated between cohorts regarding reoperation or complications. [136] (10.1186/s13018-024-05360-0)
- [L4] Delaying rotator cuff surgery for 3 to 6 months did not lead to higher retear rates or inferior PROMs compared with earlier surgery, but delaying surgery for 1 year or more resulted in higher retear rates. [138] (10.1177/03635465211069560)
- [L5] Bacterial contamination from sutures may contribute to impaired healing or retear after rotator cuff repair, even with arthroscopic techniques, necessitating stringent aseptic practices and tailored prophylactic measures. [139] (10.1016/j.arthro.2024.03.026)
- [L4] Although arthroscopic revision RCR improved shoulder function, retears were frequent but usually smaller. [141] (10.1177/03635465221097410)
- [L4] Although the complication rate is high, most can be treated successfully without compromise to clinical outcome. [142] (10.1016/j.jse.2012.11.016)
See Also¶
- Rotator Cuff
- Cuff Arthropathy
- Cuff Pathology
- Calcific Tendinitis
- Clinical Assessment
- Total shoulder arthroplasty
- Reverse Shoulder Arthroplasty
- Revision rotator cuff repair
References¶
[1] Editorial Commentary: One‐ and 2‐Year Outcomes Are Clinically Similar After Rotator Cuff Repair: What Are We Waiting For?. Arthroscopy. 2024. DOI: 10.1016/j.arthro.2023.11.002
[2] What are the predictors of response to physiotherapy in patients with massive irreparable rotator cuff tears? Gaining expert consensus using an international e-Delphi study. BMC Musculoskeletal Disorders. 2024. DOI: 10.1186/s12891-024-07872-6
[3] Minimum 15-year follow-up for clinical outcomes of arthroscopic rotator cuff repair. Journal of Shoulder and Elbow Surgery. 2022. DOI: 10.1016/j.jse.2022.01.116
[4] Editorial Commentary: One‐Year Follow‐Up Does Not Determine Rotator Cuff Repair Long‐Term Outcome. Arthroscopy. 2025. DOI: 10.1016/j.arthro.2024.12.040
[5] Patient-specific risk factors for repair failure and poor functional outcome after rotator cuff repair - an umbrella review. BMC Musculoskeletal Disorders. 2026. DOI: 10.1186/s12891-025-08608-w
[6] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > Indications for Rotator Cuff Repair.
[7] What are patients asking and reading online? An analysis of online patient searches for rotator cuff repair. Journal of Shoulder and Elbow Surgery. 2023. DOI: 10.1016/j.jse.2023.04.021
[8] Editorial Commentary : Rotator Cuff Repair: Graft Augmentation Provides Promising Clinical Outcomes. Arthroscopy. 2022. DOI: 10.1016/j.arthro.2021.11.035
[9] Long‐Term Outcomes After In Situ Arthroscopic Repair of Partial Rotator Cuff Tears. Arthroscopy. 2019. DOI: 10.1016/j.arthro.2018.09.026
[10] Foreword. Clinics in Sports Medicine. 2012. DOI: 10.1016/j.csm.2012.08.001
[11] One‐ and 2‐Year American Shoulder and Elbow Surgeons Scores Do Not Vary Significantly After Arthroscopic Rotator Cuff Repair: A Prospective Multicenter Analysis of 1,567 Patients. Arthroscopy. 2023. DOI: 10.1016/j.arthro.2023.09.024
[12] Return to Work After Primary Rotator Cuff Repair: A Systematic Review and Meta-analysis. The American Journal of Sports Medicine. 2021. DOI: 10.1177/0363546520975426
[13] Orthopaedic Knowledge Update Sports Medicine 6. Rotator Cuff Disease > Annotated References.
[14] Prospective analysis of arthroscopic rotator cuff repair: Subgroup analysis. Journal of Shoulder and Elbow Surgery. 2009. DOI: 10.1016/j.jse.2008.11.018
[15] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Annotated References.
[16] Rockwood And Matsen S The Shoulder. Arthroscopic Management of Prearthritic and Arthritic Conditions of the Shoulder and the Postarthroplasty Shoulder > Instability > Rotator Cuff.
[17] Campbell S Operative Orthopaedics 4 Volume Set. ARTHROSCOPIC REPAIR OF POSTERIOR HUMERAL AVULSION OF THE GLENOHUMERAL LIGAMENT > PARTIAL-THICKNESS ROTATOR CUFF TEARS.
[18] Arthroscopic Repair of Massive Rotator Cuff Tears. The American Journal of Sports Medicine. 2013. DOI: 10.1177/0363546513485719
[19] Apley And Solomon S Concise System Of Orthopaedics And Trauma. DISORDERS OF THE ROTATOR CUFF.
[20] The influence of intraoperative factors and postoperative rehabilitation compliance on the integrity of the rotator cuff after arthroscopic repair. Journal of Shoulder and Elbow Surgery. 2015. DOI: 10.1016/j.jse.2014.06.050
[21] Campbell S Operative Orthopaedics 4 Volume Set. ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION WITH BONE-PATELLAR TENDON-BONE GRAFT > OPEN REPAIR OF ROTATOR CUFF TEARS > TECHNIQUE 46.2.
[22] “Functional outcomes and MRI-based tendon healing after (antero-) superior rotator cuff repair among patients under 50 years: retrospective analysis of traumatic versus non-traumatic rotator cuff tears”. BMC Musculoskeletal Disorders. 2023. DOI: 10.1186/s12891-023-06174-7
[23] Severe Obesity Is Not Associated With Worse Functional Outcomes Following Arthroscopic Rotator Cuff Repair. Arthroscopy. 2022. DOI: 10.1016/j.arthro.2022.02.026
[24] Imaging Evaluation of the Rotator Cuff. Clinics in Sports Medicine. 2012. DOI: 10.1016/j.csm.2012.07.010
[25] Determining the Time Required to Achieve Clinically Significant Outcomes on the PROMIS Upper Extremity Questionnaire After Arthroscopic Rotator Cuff Repair. Orthopaedic Journal of Sports Medicine. 2023. DOI: 10.1177/23259671231157038
[27] Fifteen-Year Results of a Comparative Analysis of Tendon Repair Versus Physiotherapy for Small-to-Medium-Sized Rotator Cuff Tears. Journal of Bone and Joint Surgery. 2024. DOI: 10.2106/jbjs.24.00065
[28] Classifications in Brief: Hamada Classification of Massive Rotator Cuff Tears. Clinical Orthopaedics & Related Research. 2017. DOI: 10.1007/s11999-017-5340-7
[29] Rip‐Stop Fixation Constructs for Rotator Cuff Repair. Arthroscopy. 2023. DOI: 10.1016/j.arthro.2023.06.013
[30] Arthroscopic Transosseous Rotator Cuff Repair. Journal of the American Academy of Orthopaedic Surgeons. 2023. DOI: 10.5435/jaaos-d-22-00057
[31] Orthopaedic Basic Science Fifth Edition Print Ebook. Lumbar Spondylosis, Degenerative Disk Disease, and Radiculopathy > Clinical Example: Rotator Cuff Repair.
[32] Editorial Commentary: Patients 75 Years and Older Achieve Rotator Cuff Repair Outcome Similar to Younger Patients with Proper Surgical Indications. Arthroscopy. 2024. DOI: 10.1016/j.arthro.2023.12.023
[33] Rotator cuff repair rehabilitation considerations and respective guidelines: a narrative review. JSES Reviews, Reports, and Techniques. 2021. DOI: 10.1016/j.xrrt.2021.04.009
[34] Predicted healing rates do not correlate with patient outcomes following rotator cuff repair—A minimum 2-year follow-up. Journal of ISAKOS. 2026. DOI: 10.1016/j.jisako.2025.101026
[35] Poster 147: Patient-Reported and Clinical Outcomes up to 2 Years after Primary Rotator Cuff Repair: Do We Need a 2-Year Follow-Up Visit?. Orthopaedic Journal of Sports Medicine. 2024. DOI: 10.1177/2325967124s00116
[36] Proton Density Fat-Fraction of Rotator Cuff Muscles Is Associated With Isometric Strength 10 Years After Rotator Cuff Repair: A Quantitative Magnetic Resonance Imaging Study of the Shoulder. The American Journal of Sports Medicine. 2017. DOI: 10.1177/0363546517703086
[37] Patient, imaging, and surgical factors associated with supraspinatus re-tear pattern after rotator cuff repair. JSES International. 2024. DOI: 10.1016/j.jseint.2024.06.007
[39] Serial structural and functional assessments of rotator cuff repairs: do they differ at 6 and 19 months postoperatively?. Journal of Shoulder and Elbow Surgery. 2012. DOI: 10.1016/j.jse.2011.05.027
[41] Clinical Outcome and Imaging of Arthroscopic Single‐Row and Double‐Row Rotator Cuff Repair: A Prospective Randomized Trial. Arthroscopy. 2011. DOI: 10.1016/j.arthro.2011.07.003
[43] Previous rotator cuff repair increases the risk of revision surgery for periprosthetic joint infection after reverse shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2023. DOI: 10.1016/j.jse.2022.07.001
[44] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > RELEVANT SHOULDER ANATOMY > Rotator Cuff.
[45] Aaos Comprehensive Orthopaedic Review 3. Rotator Cuff Tears and Cuff Tear Arthropathy > I. Rotator Cuff Tears.
[46] Rockwood And Matsen S The Shoulder. Developmental Anatomy of the Shoulder and Anatomy of the Glenohumeral Joint > Rotator Cuff.
[48] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > Rotator Cuff > Scapulohumeral Ligaments.
[49] Aaos Comprehensive Orthopaedic Review 3. Rotator Cuff Tears and Cuff Tear Arthropathy > II. Cuff Tear Arthropathy.
[51] A Lange Medical Book Current Diagnosis Treatment In Orthopedics Fifth Edition. 3Sports Medicine > 1. Subacromial Bursitis and Rotator Cuff Tendinosis.
[52] Glenohumeral decentering in rotator cuff deficiency: relationship to rotator cuff muscle, scapula morphology, and shoulder function. Journal of Shoulder and Elbow Surgery. 2026. DOI: 10.1016/j.jse.2025.03.038
[53] Quantifying Threshold Scores for Patient Satisfaction After Massive Rotator Cuff Repair for the Interpretation of Mid‐Term Patient‐Reported Outcomes. Arthroscopy. 2023. DOI: 10.1016/j.arthro.2023.06.031
[55] Increased Glenohumeral Joint Loads Due to a Supraspinatus Tear Can Be Reversed With Rotator Cuff Repair: A Biomechanical Investigation. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2022. DOI: 10.1016/j.arthro.2021.10.036
[56] At a 10-Year Follow-up, Tendon Repair Is Superior to Physiotherapy in the Treatment of Small and Medium-Sized Rotator Cuff Tears. Journal of Bone and Joint Surgery. 2019. DOI: 10.2106/jbjs.18.01373
[57] Campbell S Operative Orthopaedics 4 Volume Set. ARTHROSCOPIC REPAIR OF POSTERIOR HUMERAL AVULSION OF THE GLENOHUMERAL LIGAMENT > FULL-THICKNESS ROTATOR CUFF TEARS.
[58] A modified Patte classification system for rotator cuff tendon retraction to predict reparability and tendon healing in arthroscopic rotator cuff repair. Knee Surgery, Sports Traumatology, Arthroscopy. 2024. DOI: 10.1002/ksa.12162
[59] Miller S Review Of Orthopaedics. ROTATOR CUFF DISEASE > 4. Imaging.
[60] Miller S Review Of Orthopaedics. SECTION 16 PATELLAR TRACKING IN TOTAL KNEE ARTHROPLASTY > ROTATOR CUFF DISEASE > 4. Imaging.
[61] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Summary.
[63] Speed of Recovery After Arthroscopic Rotator Cuff Repair. Arthroscopy. 2017. DOI: 10.1016/j.arthro.2017.04.033
[64] Intraoperative Channeling in Arthroscopic Rotator Cuff Repair: A Multicenter Randomized Controlled Trial. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465221138562
[65] Knotted and knotless double row transosseous equivalent repair techniques for arthroscopic rotator cuff repair demonstrate comparable post‐operative outcomes. Knee Surgery, Sports Traumatology, Arthroscopy. 2022. DOI: 10.1007/s00167-022-07121-0
[67] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Calcific Tendinitis > Pathophysiology.
[68] Effect of Two Rehabilitation Protocols on Range of Motion and Healing Rates After Arthroscopic Rotator Cuff Repair: Aggressive Versus Limited Early Passive Exercises. Arthroscopy. 2011. DOI: 10.1016/j.arthro.2011.07.012
[69] Orthopaedic Knowledge Update Sports Medicine 6. Rotator Cuff Disease > Natural History and Societal Impact.
[70] Clinical effect of modified anterolateral acromioarthroplasty during arthroscopic rotator cuff repair. BMC Musculoskeletal Disorders. 2024. DOI: 10.1186/s12891-024-07619-3
[71] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Rotator Cuff Tears > Evaluation.
[72] Suprascapular nerve release does not provide additional benefits in arthroscopic rotator cuff repair surgery: a systematic review and meta‐analysis. Knee Surgery, Sports Traumatology, Arthroscopy. 2022. DOI: 10.1007/s00167-022-07066-4
[74] Editorial Commentary: Multimodal Analgesia for Rotator Cuff Repair Should Be Individualized Based on Surgical Location and Complexity and Patient Comorbidity. Arthroscopy. 2024. DOI: 10.1016/j.arthro.2024.06.010
[75] Apley And Solomon S Concise System Of Orthopaedics And Trauma. SECONDARY ARTHROPATHY > TEARS OF THE ROTATOR CUFF.
[76] Prognostic value of baseline muscle strength for functional recovery after rotator cuff repair: an observational study. Journal of Shoulder and Elbow Surgery. 2026. DOI: 10.1016/j.jse.2025.07.010
[77] Patients Who Undergo Rotator Cuff Repair Can Safely Return to Driving at 2 Weeks Postoperatively. Journal of Bone and Joint Surgery. 2022. DOI: 10.2106/jbjs.21.01436
[78] Comparison of functional outcomes following early and delayed arthroscopic repair for traumatic and non-traumatic rotator cuff injuries. Journal of Orthopaedic Surgery and Research. 2024. DOI: 10.1186/s13018-024-04858-x
[79] Return to Activities after Arthroscopic Rotator Cuff Repair: A Systematic Review and Meta-analysis. Orthopaedic Journal of Sports Medicine. 2023. DOI: 10.1177/2325967121s00867
[80] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > Natural History of Symptomatic Rotator Cuff Tears.
[81] Predictors of Return to Work Following Primary Arthroscopic Rotator Cuff Repair: An Analysis of 1502 Cases. The American Journal of Sports Medicine. 2023. DOI: 10.1177/03635465231152479
[82] Limited physical therapy utilization protocol does not affect impairment and disability in Workers' Compensation patients after rotator cuff repair: a short-term follow-up study. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2012.05.022
[84] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > ARTHROSCOPIC ROTATOR CUFF REPAIR.
[86] Editorial Commentary : Partial Rotator Cuff Repair and Deltoid Retraining Shows Positive Outcomes for Large to Massive Rotator Cuff Tear. Arthroscopy. 2025. DOI: 10.1016/j.arthro.2025.01.003
[87] Editorial Commentary: Platelet‐Rich Plasma for Rotator Cuff Repairs: No Evidence for Improved Long‐Term Outcomes … Yet!. Arthroscopy. 2022. DOI: 10.1016/j.arthro.2021.06.035
[88] Early Postoperative Stiffness After Arthroscopic Rotator Cuff Repair Correlates With Improved Tendon Healing. Arthroscopy. 2024. DOI: 10.1016/j.arthro.2024.01.038
[89] Editorial Commentary: Shoulder Stiffness Enhances Repair Integrity After Rotator Cuff Repair. Arthroscopy. 2024. DOI: 10.1016/j.arthro.2024.02.038
[91] Pain Relief, Motion, and Function after Rotator Cuff Repair or Reconstruction May Not Persist after 16 Years. Clinical Orthopaedics & Related Research. 2010. DOI: 10.1007/s11999-010-1403-8
[92] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > NATURAL HISTORY OF ROTATOR CUFF PATHOLOGY AND IMPLICATIONS ON SURGICAL INDICATIONS > Natural History of Asymptomatic Rotator Cuff Tears.
[93] Editorial Commentary: Multiple Factors, Including Multimodal Anesthesia, Can Reduce Opioid Requirements After Rotator Cuff Repair. Arthroscopy. 2024. DOI: 10.1016/j.arthro.2024.09.017
[95] Prevention of Shoulder Stiffness after Rotator Cuff Repair. Clinical Orthopaedics & Related Research. 2005. DOI: 10.1097/01.blo.0000137564.27841.27
[96] Orthopaedic Knowledge Update 13 Ebook Without Multimedia. Shoulder Instability, Rotator Cuff Disorders, Muscular Ruptures, Adhesive Capsulitis, Calcific Tendinitis > Rotator Cuff Tears > Role of the Biceps Tendon.
[97] Assessment of the impact of gabapentin on postoperative pain following shoulder open rotator cuff repair: a double-blind clinical trial. Journal of Shoulder and Elbow Surgery. 2025. DOI: 10.1016/j.jse.2024.08.044
[99] One-stage rotator cuff repair in stiff shoulders shows comparable range of motion, clinical outcome and retear rates to non-stiff shoulders: a systematic review. Journal of Orthopaedic Surgery and Research. 2023. DOI: 10.1186/s13018-023-04104-w
[100] Improved Contractility of the Infraspinatus Muscle after Rotator Cuff Repair Preserves the Acromion-humeral Distance and Improves Postoperative Outcomes. Journal of ISAKOS. 2025. DOI: 10.1016/j.jisako.2025.100817
[101] Indications for Reverse Total Shoulder Arthroplasty in Rotator Cuff Disease. Clinical Orthopaedics & Related Research. 2010. DOI: 10.1007/s11999-009-1188-9
[103] Tendon Properties Remain Altered in a Chronic Rat Rotator Cuff Model. Clinical Orthopaedics & Related Research. 2010. DOI: 10.1007/s11999-009-1206-y
[104] Rockwood And Matsen S The Shoulder. Fractures, Dislocations, and Acquired Problems of the Shoulder in Children > MINI-OPEN ROTATOR CUFF REPAIR.
[106] Preoperative handgrip strength can predict early postoperative shoulder function in patients undergoing arthroscopic rotator cuff repair. Journal of Orthopaedic Surgery and Research. 2024. DOI: 10.1186/s13018-024-04750-8
[108] Long-term functional and structural outcome in patients with intact repairs 1 year after open transosseous rotator cuff repair. Journal of Shoulder and Elbow Surgery. 2009. DOI: 10.1016/j.jse.2008.11.006
[111] Is the Use of a Buprenorphine Transdermal Patch More Effective Than Oral Medications for Postoperative Analgesia After Arthroscopic Rotator Cuff Repair? A Randomized Clinical Trial. Clinical Orthopaedics & Related Research. 2024. DOI: 10.1097/corr.0000000000003303
[112] Arthroscopic Replacement of Massive, Irreparable Rotator Cuff Tears Using a GraftJacket Allograft: Technique and Preliminary Results. Arthroscopy. 2008. DOI: 10.1016/j.arthro.2007.07.033
[113] Arthroscopic rotator cuff repair performed with intra-articular tranexamic acid: could it provide improved visual clarity and less postoperative pain? A prospective, double-blind, randomized study of 63 patients. Journal of Shoulder and Elbow Surgery. 2023. DOI: 10.1016/j.jse.2022.10.007
[114] Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. Journal of Shoulder and Elbow Surgery. 2012. DOI: 10.1016/j.jse.2012.01.025
[115] Prospective 1-Year Outcomes Are Maintained at Short-Term Final Follow-Up After Superior Capsular Reconstruction Augmentation of Complete Rotator Cuff Repair. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2022. DOI: 10.1016/j.arthro.2021.11.008
[118] Higher Upper Subscapularis Goutallier Grade and Coracohumeral Distance Narrowing Are Predictive of Subscapularis Tears in Patients Undergoing Arthroscopic Rotator Cuff Repair. Arthroscopy. 2023. DOI: 10.1016/j.arthro.2023.10.017
[121] Long-term results of revision rotator cuff repair for failed cuff repair: a minimum 10-year follow-up study. Journal of Shoulder and Elbow Surgery. 2024. DOI: 10.1016/j.jse.2023.06.009
[122] Fixation technique of biodegradable magnesium alloy suture anchor in the rotator cuff repair of the shoulder in a goat model: a technical note. BMC Musculoskeletal Disorders. 2024. DOI: 10.1186/s12891-024-07300-9
[124] No Short-term Clinical Benefit to Bovine Collagen Implant Augmentation in Primary Rotator Cuff Repair: A Matched Retrospective Study. Clinical Orthopaedics & Related Research. 2024. DOI: 10.1097/corr.0000000000003247
[125] Returning to golf after rotator cuff repair. JSES International. 2023. DOI: 10.1016/j.jseint.2022.12.005
[126] Indications and Technique: Rotator Cuff Repair Augmentation. Journal of the American Academy of Orthopaedic Surgeons. 2023. DOI: 10.5435/jaaos-d-23-00101
[128] Effect of Immobilization without Passive Exercise After Rotator Cuff Repair. Journal of Bone and Joint Surgery. 2014. DOI: 10.2106/jbjs.l.01741
[129] A Radiographic Classification of Massive Rotator Cuff Tear Arthritis. Clinical Orthopaedics & Related Research. 2011. DOI: 10.1007/s11999-011-1896-9
[130] A Systematic Review of Long-term Clinical and Radiological Outcomes of Arthroscopic and Open/Mini-open Rotator Cuff Repairs. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465211073332
[132] Arthroscopic Partial Repair of Irreparable Rotator Cuff Tears: Factors Related to Greater Degree of Clinical Improvement at 2 Years of Follow‐Up. Arthroscopy. 2017. DOI: 10.1016/j.arthro.2017.06.047
[133] Timing of retears after arthroscopic rotator cuff repair and associated factors: a retrospective analysis. Journal of Shoulder and Elbow Surgery. 2023. DOI: 10.1016/j.jse.2023.01.026
[135] Venous thromboembolism after arthroscopic rotator cuff repair in a patient with a negative presurgical SARS-CoV-2 test who developed symptomatic COVID-19 three days after surgery. Journal of Shoulder and Elbow Surgery. 2021. DOI: 10.1016/j.jse.2021.02.003
[136] Lower socioeconomic status is correlated with worse outcomes after arthroscopic rotator cuff repair. Journal of Orthopaedic Surgery and Research. 2024. DOI: 10.1186/s13018-024-05360-0
[138] Role of Delay Between Injury and Surgery on the Outcomes of Rotator Cuff Repair: A Systematic Review and Meta-analysis. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465211069560
[139] Editorial Commentary : Suture Bacterial Contamination May Contribute to Impaired Healing or Retear After Rotator Cuff Repair, Even Using Arthroscopic Techniques. Arthroscopy. 2024. DOI: 10.1016/j.arthro.2024.03.026
[141] Results of Arthroscopic Revision Rotator Cuff Repair for Failed Open or Arthroscopic Repair: A Prospective Multicenter Study on 100 Cases. The American Journal of Sports Medicine. 2022. DOI: 10.1177/03635465221097410
[142] Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears in patients younger than 65 years old: results after five to fifteen years. Journal of Shoulder and Elbow Surgery. 2013. DOI: 10.1016/j.jse.2012.11.016