Patients › Rehabilitation
Distal Triceps Tendon Repair
A protected recovery plan after repair of the distal triceps tendon at the elbow, resting the arm in a simple sling at 90 degrees and freeing movement, then active straightening, then strength in careful stages.
This protocol guides your recovery after surgical repair of the distal triceps tendon (the tendon that anchors the triceps muscle, which straightens your elbow, to the point of the elbow), with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your physiotherapist or hand therapist; bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
A distal triceps repair re-attaches the torn tendon back onto the bone at the point of the elbow (the olecranon). At the end of the operation, Dr Hirpara checks that the repair is safe and intact with the elbow bent to a right angle (90°). Because of that, your elbow is rested in a simple sling at about 90°, a comfortable, standard position. There is no hinged brace, and the elbow is not held out near straight. The sling comes off for your exercises and for washing.
The tendon is loaded (put under strain) in two ways, and the early plan is built around protecting against both:
- Bending the elbow stretches the repair. So for about the first six weeks, bending is capped at 90° (a right angle). Straightening, on the other hand, relaxes the tendon, so straightening out fully is free and encouraged within comfort.
- Actively straightening the elbow works the triceps, which pulls on the repair. So for about the first six weeks you do not actively straighten the elbow under its own power; movement in that direction is done gently and with help, not by the triceps itself.
Movement is then opened up in careful stages: fuller bending from about six weeks, active straightening from about six weeks, and resisted (loaded) strengthening from about twelve weeks. The repair keeps maturing for several months, which is why heavier loading and return to sport are built back gradually rather than all at once.
Precautions and limitations¶
- Do NOT bend your elbow past a right angle (90°) for about the first six weeks, as bending stretches and strains the repair. Straightening out fully is fine and encouraged.
- Do NOT actively straighten the elbow under its own muscle power for about the first six weeks; let it be straightened gently with help, not by working the triceps.
- Do NOT do any resisted straightening or push/press through the arm until about twelve weeks: no triceps kickbacks, no bench or overhead press, and no pushing up from a chair or bed with the operated arm.
- Wear your sling at 90° as directed (not a brace, not held straight), and do NOT drive while you are in it or while your arm cannot safely control the wheel.
- Keep your hand, wrist and shoulder moving from the start, and use the hand for light everyday tasks within comfort, as long as it does not involve pushing, lifting or forced bending of the elbow.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises¶

Kieran Hirpara 4.0
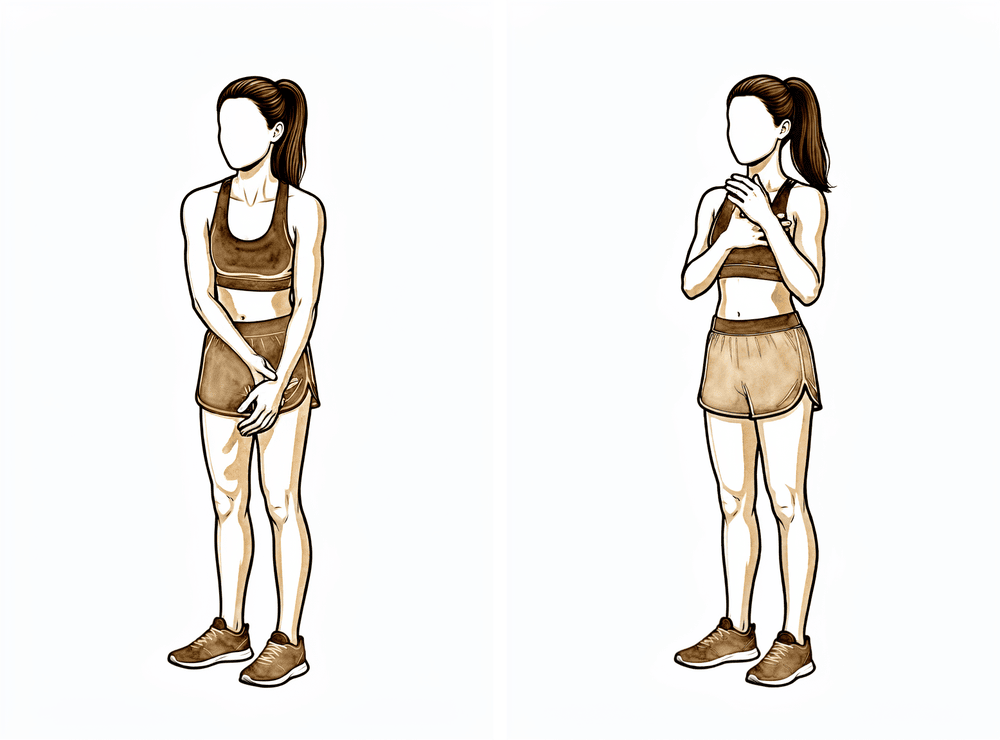
Protected elbow movement (0–90° arc)
Out of the sling, gently move the elbow within its safe range: you may straighten it fully (extension is free, to comfort), but do NOT bend it past a right angle (90°) — about as far as holding a phone to your ear. Move slowly and stay within that arc. Bending past 90° pulls on the healing tendon, so it is held back for about the first six weeks.
10 times, 2–3 times a day, within the 0–90° arc
Kieran Hirpara 4.0
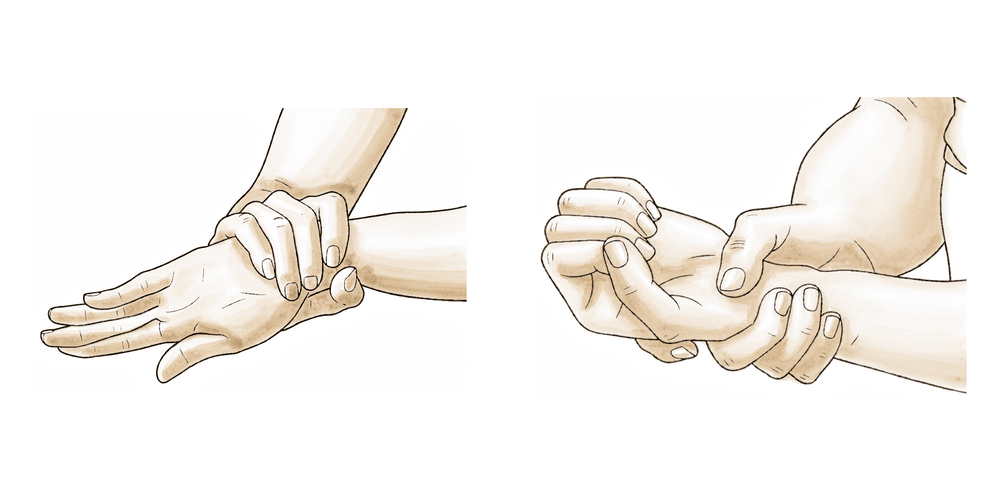
Assisted (passive) elbow bend
Use your other hand to gently bend the operated elbow up towards your shoulder, keeping the triceps completely relaxed — you are not pulling with the operated arm. Stop at your set limit (about 90° early on). This keeps the elbow supple without working the triceps.
10 times, 2–3 times a day, to your set limit only
Kieran Hirpara 4.0
Forearm rotation (palm up / palm down)
With your elbow tucked at your side and bent comfortably, gently turn your palm up towards the ceiling, then down towards the floor. Keep it slow and easy. This keeps the forearm supple and does not load the triceps repair, so it can begin early.
10 times each direction, 2–3 times a day

Kieran Hirpara 4.0
Triceps muscle-set (gentle, no movement)
A LATER exercise — only once your physiotherapist starts it (commonly from around 8 weeks). With the elbow supported, gently tighten the muscle on the BACK of your upper arm (the triceps) as if to straighten the elbow, but WITHOUT letting it actually move — a light press, hold, then relax. Do not do this in the first six weeks.
Hold ~5 seconds, 5–10 times, as guided (later phase)
Kieran Hirpara 4.0
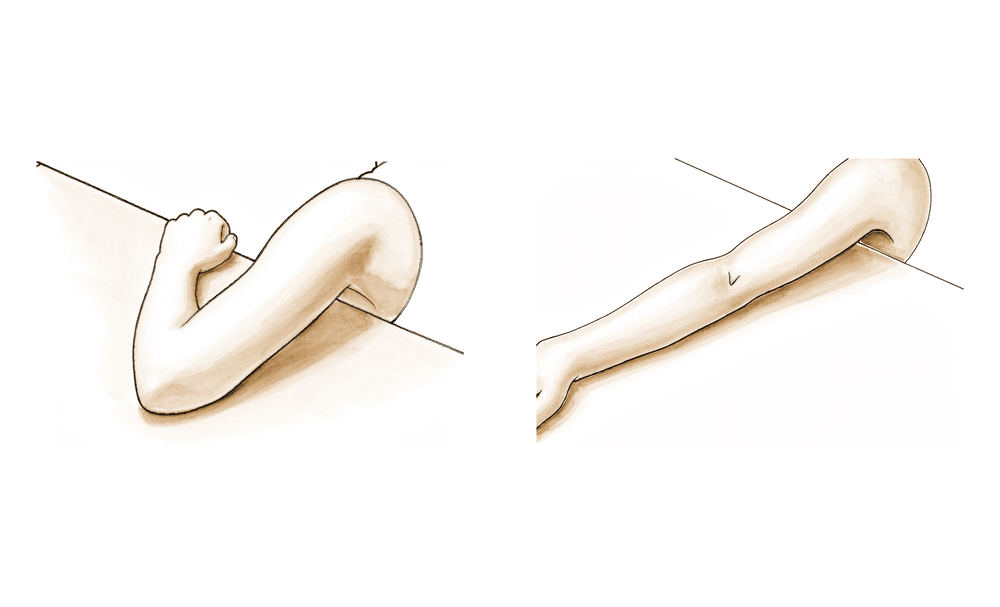
Active elbow straightening (no resistance)
A LATER exercise — begins from around 6 weeks, once cleared. Gently straighten the elbow under its own power with NO weight in the hand, then use your other hand to help lower it back down (so the triceps does not have to control the downward phase yet). Stay pain-free. There is NO active straightening in the first six weeks.
10 times, as guided (from ~6 weeks, no resistance)
Kieran Hirpara 4.0
Triceps muscle-set against light hold (isometric extension)
A LATER exercise — from around 8 weeks, as guided. Press the forearm gently against your other hand or a fixed surface as if to straighten the elbow, building the effort up only to a light, comfortable level, holding without the elbow moving. This wakes the triceps up before resisted work is allowed.
Hold ~5 seconds, 5–10 times, as guided (later phase)
Kieran Hirpara 4.0
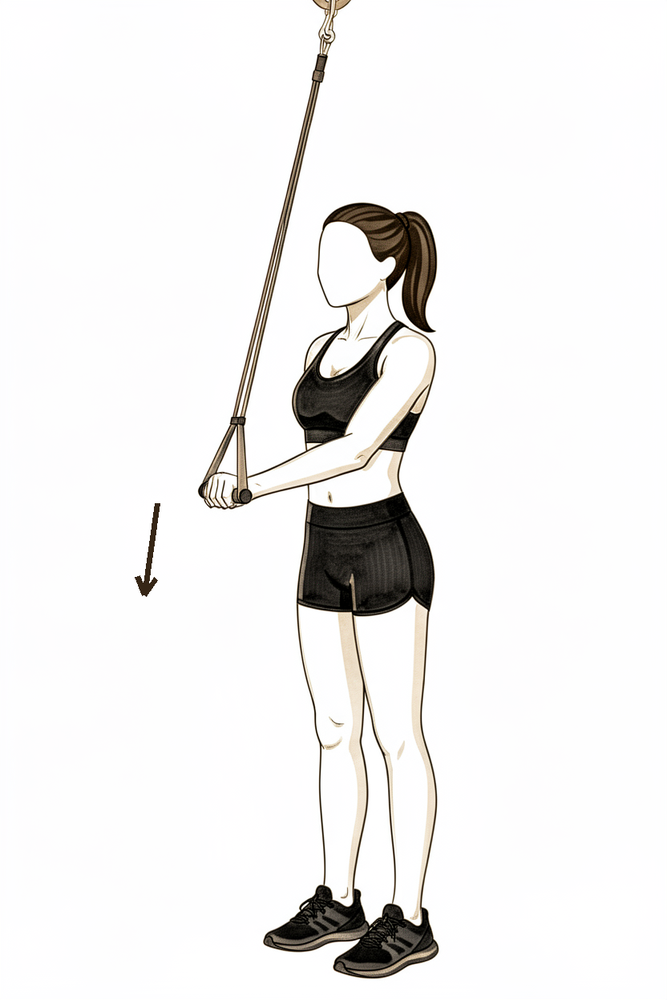
Resisted elbow straightening with a band (late strengthening)
A LATE exercise — only once resisted work is cleared, commonly from around 12 weeks. Straighten the elbow against a light resistance band, then control it slowly back. Build the resistance up gradually over several weeks. This directly loads the repaired tendon, so it is the last thing to start — never rush it, and stop if it is painful.
As guided by your physiotherapist (from ~12 weeks only)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your physiotherapist, staying within whatever range and limits you have been given. The early exercises keep the elbow and forearm moving without working or stretching the repair: gentle movement within the protected 0–90° arc, assisted bending, and forearm rotation. The triceps muscle-sets, active straightening and band work belong to later phases and should not be started until you are specifically cleared. Stop anything that causes sharp pain at the back of the elbow.
Your clinical protocol¶
The rest of this page is the staged clinical protocol for rehabilitation after distal triceps tendon repair. This section is to be provided to your physiotherapist or hand therapist, and each phase opens with a plain-English explanation of what is happening. The repair is loaded by elbow flexion (which stretches it) and by active or resisted extension (which contracts the triceps onto it), so the protocol protects both while restoring motion, then active extension, then resisted strength.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the fixation (transosseous tunnels vs suture-anchor footprint), tissue quality, and the protected arc. Dr Hirpara's repair is checked intra-operatively to be safe at 90° of flexion and is rested in a simple sling at 90° (no hinged brace, not held in extension); the protected arc is 0–90° with extension free to comfort and flexion capped at 90°.
Phase I — protected motion in a 90° sling (weeks 0 to 6)¶
The first six weeks protect the repair while keeping the elbow from stiffening. The arm rests in a simple sling at 90°, off for exercises and hygiene. The elbow moves only within the protected 0–90° arc, straightening out fully to comfort but not bending past a right angle, and never under active triceps power.
For your physiotherapist:
Education and precautions - Immobilise in a simple sling at 90° (no hinged brace, NOT held near extension); off for exercises and washing - Protected arc 0–90° only: extension free to full/comfort; flexion not past 90° - No active or resisted elbow extension (active triceps contraction loads the repair) - No weight-bearing or pushing through the operated arm; light unloaded hand use within comfort - Keep shoulder PROM gentle early (protects the long head crossing the shoulder)
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle hand pump, ice as needed - Exercises: AAROM/PROM elbow within 0–90° (extension to comfort, flexion capped at 90°); active wrist, hand and grip ROM; gentle shoulder ROM; gentle forearm rotation; no active extension
Criteria to progress - Wound healed; comfortable, controlled 0–90° arc at around six weeks
Phase II — advancing flexion and starting active extension (weeks 6 to 12)¶
From about six weeks the flexion cap is released and bending is progressed past 90° towards full. Active straightening (extension) is introduced without resistance, and the triceps is gently re-activated with isometrics. Resisted extension and weight-bearing are still withheld.
For your physiotherapist:
Assessments - Active and passive range of motion (flexion now progressing past 90°, extension); pain and swelling; wound/scar review
Education and precautions - Progress flexion past 90° toward full gradually from around six weeks - No resisted extension and no weight-bearing through the arm until 12 weeks
Management - Exercises: weeks 6–8 begin active concentric extension with NO resistance, pain-free range (assist the lowering/eccentric phase with the other arm); week 8 light submaximal triceps isometrics; continue full-arc mobility and forearm rotation; commence scar management once healed
Criteria to progress - Full painless ROM; full active extension with good control; pain ≤3/10
Phase III — strengthening and return (weeks 12 to 16 and beyond)¶
Once movement is restored and resisted work is cleared (around twelve weeks), strengthening begins and is built up gradually: resisted triceps work (concentric then eccentric), then light closed-chain weight-bearing, then limited-range pressing. Return to sport is criterion-based, at the earliest around five to six months.
For your physiotherapist:
Assessments - Triceps strength versus the other side; pain/swelling response to loading; functional and sport-/work-specific testing as appropriate
Education and precautions - Begin resisted triceps strengthening (concentric → eccentric) from around 12 weeks; build load gradually - Closed-chain weight-bearing from around 12 weeks (start light, small range); light pressing (push-ups, limited range) from around 14 weeks
Management - Exercises: progressive resisted elbow extension (band → light weights); graded closed-chain loading; limited-range pressing; continue any residual mobility work - Consider discharge once strength is near-symmetrical and a suitable return of function is achieved - Consider referral back to the treating doctor if recovery plateaus or there is a poor outcome
Criteria for return to sport - 5/5 triceps strength; pain-free high-velocity and sport-specific control
Getting back to work and activity¶
Light everyday hand use (eating, writing and light self-care) is encouraged from the start, within comfort, as long as it does not involve pushing, lifting or bending the elbow past its limit. Because you must not drive while the arm is in the sling or unable to safely control the wheel, plan for help with transport in the early weeks; driving resumes once you are out of the sling and can control the car, as confirmed at your review.
Resisted loading and weight-bearing through the arm (pushing, pressing, lifting and pulling) waits until about twelve weeks, and are then built up gradually. Return to sport is at the earliest around five to six months, and is based on regaining full pain-free movement and adequate, symmetrical triceps strength, judged by Dr Hirpara and your physiotherapist, not by the calendar alone. Heavier manual work follows the same criterion-based progression.
After your protocol¶
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and returning to sport. The phased plan above reflects published rehabilitation guidance after distal triceps tendon repair, and your ongoing recovery is guided individually by Dr Hirpara and your physiotherapist according to how your elbow progresses.
Evidence & references
Distal Triceps Tendon Repair — Post-operative Rehabilitation (Evidence Brief)¶
Topic scope: post-operative rehabilitation after surgical reattachment of the avulsed distal triceps tendon to the olecranon (transosseous bone tunnels or suture-anchor footprint repair; best performed within ~3 weeks of injury). The extension mechanism is loaded by elbow flexion (passive stretch of the repair) and by active/resisted extension (triceps contraction), so the rehab cadence is built around protecting both, then restoring motion, then active extension, then resisted strength.
Defining principle: the repair is loaded in flexion and by triceps contraction, so early rehab limits flexion and blocks active/resisted extension while motion is restored, then releases active extension (~6 wk) and resisted extension (~12 wk) in steps, with return to sport at ~5–6 months. Dr Hirpara's stance: the repair is checked intra-operatively to be safe at 90° of flexion, so the elbow is rested in a simple sling at 90° (a standard, comfortable position — no hinged brace, and NOT held near extension) with a protected 0–90° arc (extension free to comfort, flexion capped at 90°) for ~6 weeks. This is deliberately less restrictive on early flexion than the published near-extension / 20°-flexion-lock guidelines, while keeping the key loading rules identical (no active extension to 6 wk, no resisted extension to 12 wk).
Evidence base and corpus note¶
No RCT and no large prospective cohort defines the rehab cadence for distal triceps repair. The phased timeline rests on a published institutional clinical-care guideline (Ohio State Sports Medicine, 2021), which itself cites the core review literature, corroborated by several surgeon and physiotherapy phased protocols. The local RAG corpus is thin on triceps-specific phased rehab (rotator-cuff and biceps content dominates), but it does contain the key biomechanical repair-strength papers, which inform how early and how aggressively one can mobilise. The week-by-week timeline is therefore carried by the published clinical-care guideline, with the corpus supplying the repair-strength evidence that justifies the cadence.
Key principles and controversies¶
- Early motion vs prolonged immobilisation. Classic teaching favours protective immobilisation (splint 2–6 wk, flexion-limited brace) because the triceps insertion is loaded in flexion. A counter-trend pushes accelerated early ROM where fixation is strong — a cadaveric study comparing dynamic-tape with standard suture fixation under an intense early-rehab protocol found the novel construct biomechanically superior, i.e. fixation strength is the rate-limiter for how early one can mobilise.
- Suture-anchor vs transosseous (bone-tunnel) repair strength. Carpenter et al. (JSES 2018) found no difference in tendon displacement between transosseous cruciate tunnels and suture-anchor repair when the number of sutures is equalised; the technique by Sarokhan & Leung (Arthrosc Tech 2019) cites Clark et al. (2014) finding anatomic (knotless) footprint repair superior to transosseous cruciate repair. Stronger anatomic footprint fixation is the lever that justifies earlier/more aggressive flexion and earlier resisted extension.
- Flexion-limit progression. No consensus on the exact ramp — the OSU guideline locks at 20° then advances ~15°/5 days; others use ~10°/week or an open 0–60° arc. All converge on full passive flexion by ~6 weeks, with active extension deferred to ~6 weeks and resisted extension to ~12 weeks. KH's variant keeps the elbow at 90° in a simple sling with a free 0–90° arc — less restrictive on early flexion, same loading deferrals.
- Strength athletes / high demand. Retrospective series in strength athletes report satisfactory return to sport but underline that resisted extension and pressing loads are the highest-risk re-rupture activities, supporting the firm 12-week resisted-extension / pressing block.
Phased timeline¶
| Phase | Window | Sling / ROM ceiling | Exercises | Criteria to progress |
|---|---|---|---|---|
| I — Protected motion | Weeks 0–6 | Simple sling at 90° (no hinged brace, not near extension), off for exercises. Protected arc 0–90°: extension free to comfort, flexion capped at 90°. No active extension. | AAROM/PROM elbow within 0–90°; wrist/hand/grip AROM; gentle shoulder ROM; forearm rotation | Wound healed; comfortable, controlled 0–90° arc at ~6 wk |
| II — Advance flexion + active extension | Weeks 6–12 | Release flexion cap; progress flexion past 90° toward full. No resisted extension / weight-bearing. | Wk 6–8 active concentric extension no resistance (assist eccentric with other arm); wk 8 light submaximal triceps isometrics | Full painless ROM; full active extension with good control; pain ≤3/10 |
| III — Strengthening & return | Weeks 12–16+ | Resisted triceps strengthening (concentric → eccentric) from ~12 wk; CKC weight-bearing from ~12 wk (light, small range); limited-range pressing ~wk 14 | Progressive resisted extension; graded loading; sport-/work-specific progression | 5/5 triceps strength; pain-free high-velocity / sport-specific control |
| Return to sport | ~5–6 months | Criterion-based, at the earliest | — | Full pain-free ROM + symmetrical triceps strength |
Evidence strength flags¶
- MODERATE (protocol cadence): the phased timeline (no active extension to ~6 wk, resisted extension to ~12 wk, return to sport ~5–6 mo) — anchored to the OSU Sports Medicine clinical-care guideline and corroborating surgeon/PT protocols. No defining rehab RCT.
- MODERATE (repair-strength biomechanics): suture-anchor vs transosseous equivalence with equalised sutures (Carpenter 2018); anatomic footprint superiority (Clark, via Sarokhan & Leung); insertional footprint anatomy (Whitaker 2022) — these justify the mobilisation cadence.
- LOW–MODERATE (KH's 90°-sling / flexion-capped-at-90° variant): biomechanically sound (flexion is the repair-tensioning motion; intra-op tensioning at 90° defines the safe arc) and less restrictive on early flexion than published near-extension guidance, while preserving the key extension-loading deferrals. Consensus / expert rather than trial-derived; corpus gap — no RCT or large cohort defines this exact variant.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Keener JD, Sethi PM. Distal triceps tendon injuries. Hand Clin. 2015;31(4):641–650. DOI: 10.1016/j.hcl.2015.06.012
- Carpenter SR, Stroh DA, Melvani R, et al. Distal triceps transosseous cruciate versus suture anchor repair using equal constructs: a biomechanical comparison. J Shoulder Elbow Surg. 2018;27(11):2052–2056. DOI: 10.1016/j.jse.2018.07.005
- Sarokhan AK, Leung NL. Acute triceps tendon repair: a technique utilizing 3 curved tunnels and proximal knots. Arthrosc Tech. 2019;8(11):e1325–e1330. DOI: 10.1016/j.eats.2019.07.001
- Ng T, Rush LN, Savoie FH. Arthroscopic distal triceps repair. Arthrosc Tech. 2016;5(6):e1107–e1112. DOI: 10.1016/j.eats.2016.06.011
- Whitaker JJ, Hartke J, Hawayek BJ, et al. Histologic evaluation of the triceps brachii tendon insertion: implications for triceps-sparing surgery. J Hand Surg Am. 2022. DOI: 10.1016/j.jhsa.2022.03.020
Published rehabilitation protocols & literature (URLs)¶
- Ohio State University Sports Medicine. Distal Triceps Repair — Clinical Care Guideline (G. Hock PT DPT OCS; rev. M. Salsbery PT DPT SCS; Dec 2021). https://medicine.osu.edu/-/media/files/medicine/departments/sports-medicine/medical-professionals/shoulder-and-elbow/distaltricepsrepair.pdf (NB: its near-extension / 20°-flexion-lock immobilisation differs from Dr Hirpara's 90°-sling approach; the loading deferrals are shared.)
- Cadaveric study of dynamic-tape vs standard suture fixation in distal triceps repair under an intense early-rehab protocol. PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12423150/
- Distal triceps tendon repair in strength athletes — satisfactory return to sport (22 cases). PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11355401/
Note on corpus gap: the RAG corpus lacks a dedicated distal-triceps phased rehab article; the week-by-week timeline is carried by the OSU clinical-care guideline (and corroborating surgeon protocols), with the corpus papers supplying the repair-strength evidence that justifies the cadence. Flagged accordingly.