Patients › Rehabilitation
Lateral Epicondylitis (Tennis Elbow)
A loading-based rehabilitation program for tennis elbow — settling pain then progressively strengthening the tendon — covering both non-operative care and recovery after ECRB tendon debridement.

This page explains how tennis elbow is managed and how to rehabilitate it, whether you are treating it without surgery (which is the case for almost everyone) or recovering after an operation to clean up the tendon. It is overseen by Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your physiotherapist or hand therapist; bring this page or its PDF to your therapy visits so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
What to expect¶
Tennis elbow (lateral epicondylitis) is a problem with the tendon on the outside of the elbow, specifically the common extensor tendon and in particular a small muscle called the ECRB. Despite the "-itis" in the name, it is not an inflammation that you can rest away. It is a wear-and-tear change in the tendon (a tendinosis), where the tendon fibres have become disorganised and have not healed properly.
This matters because it completely changes the treatment. You do not get better by resting and protecting the elbow; in fact, prolonged rest tends to make the tendon weaker and slower to settle. You get better by gradually loading the tendon so that it remodels and rebuilds its tolerance for work and gripping. The pattern is: first settle the pain down, then progressively strengthen, starting with gentle held (isometric) exercises and building up to controlled, slow strengthening such as the Tyler twist.
The good news is that tennis elbow usually settles on its own with the right loading program. Around 80–90% of people are better within a year, though it can occasionally take 12–18 months to fully resolve. Surgery is only considered after at least six months of good-quality, consistent rehabilitation has failed, and only a small minority (roughly 4–11%) ever reach that point.
Precautions and limitations¶
Do:
- Keep using the arm: load the tendon, do not rest it.
- Use pain as your guide: a mild ache during and after exercise is fine and expected; sharp or escalating pain means ease back.
- Lift with the palm facing up (like carrying a bowl of soup) to take load off the sore tendon.
- Use a counterforce brace over the forearm muscle during gripping and lifting tasks.
Do not:
- Do not immobilise the elbow in a cast or sling for tennis elbow; that is the wrong treatment for a tendinosis.
- Do not do heavy provocative gripping with the elbow straight and the wrist bent (for example, lifting a heavy object palm-down).
- Do not rush to a steroid injection. Cortisone can feel good for a few weeks, but the evidence shows it leads to worse results and more recurrences at 6–12 months than physiotherapy or simply waiting. It is not a first-line treatment.
Your exercises¶
Kieran Hirpara 4.0
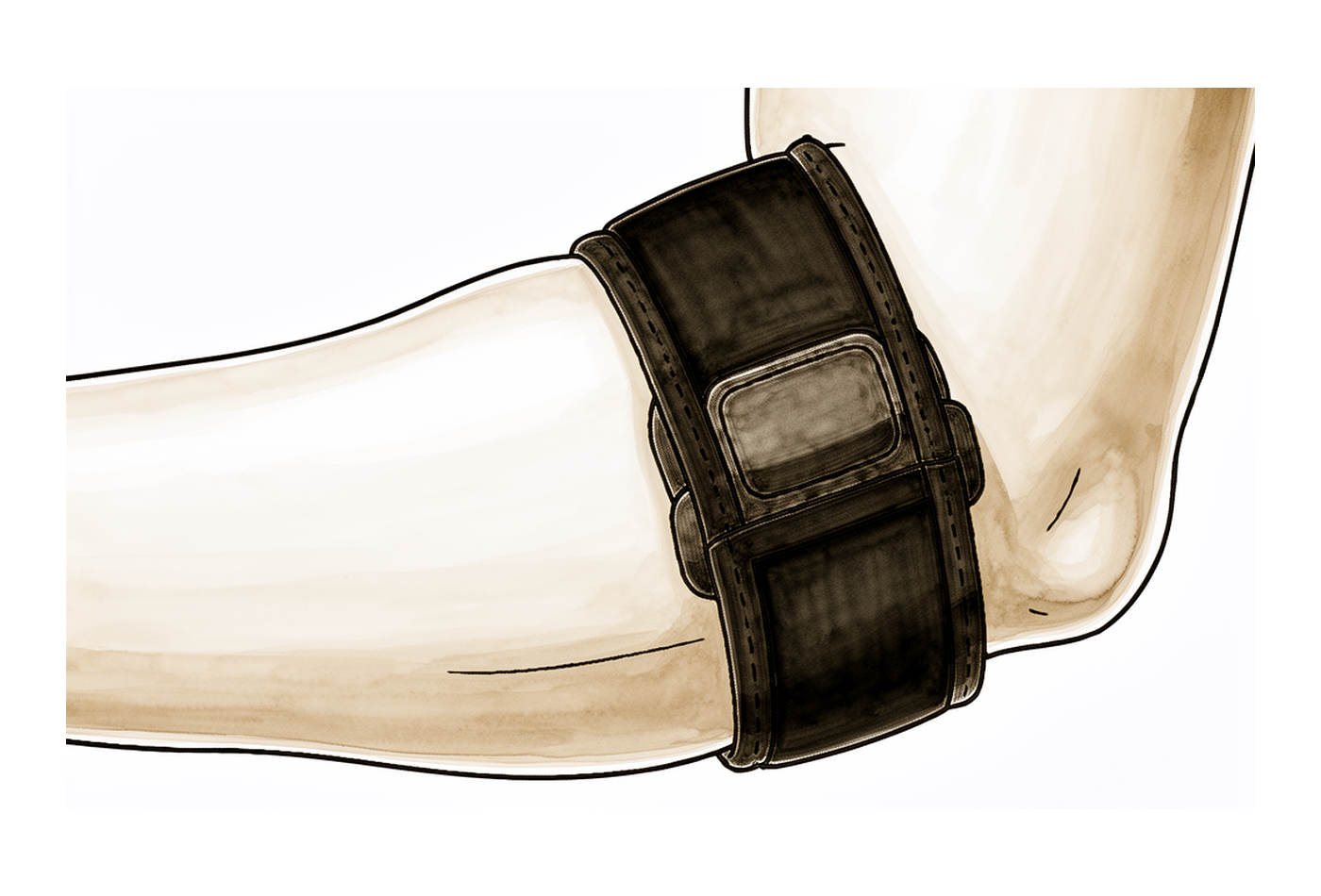
Counterforce brace
Wear the counterforce strap around your forearm, a couple of finger-widths below the elbow, over the bulk of the muscle (not on the bony point itself). It should be firm but not tight enough to make your hand tingle. Use it during gripping and lifting tasks to take load off the sore tendon; you do not need to wear it at rest or in bed.
During aggravating activities; loosen if your hand tingles
Kieran Hirpara 4.0
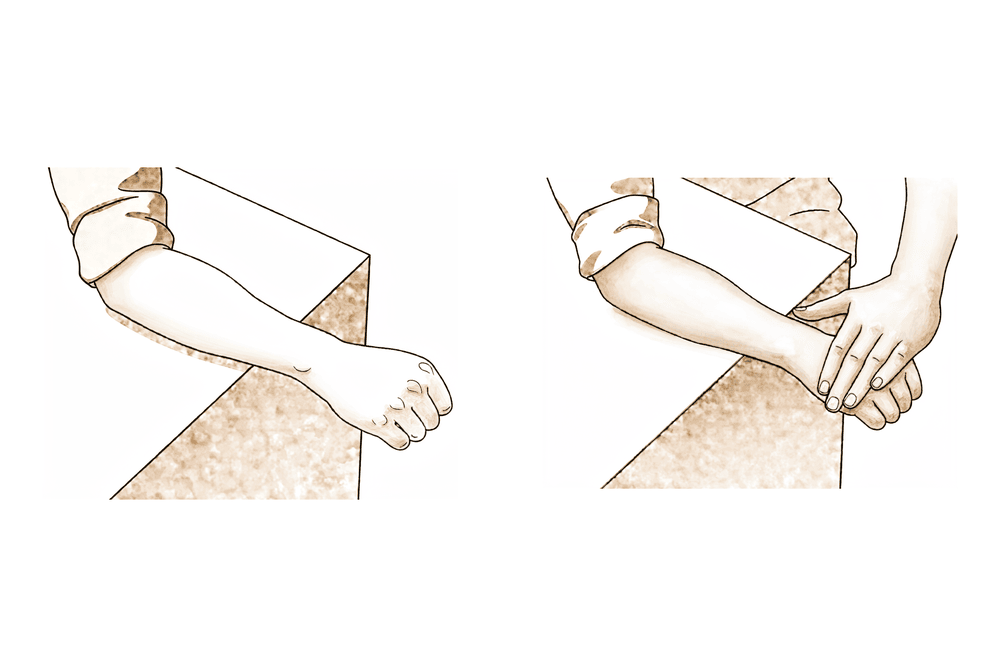
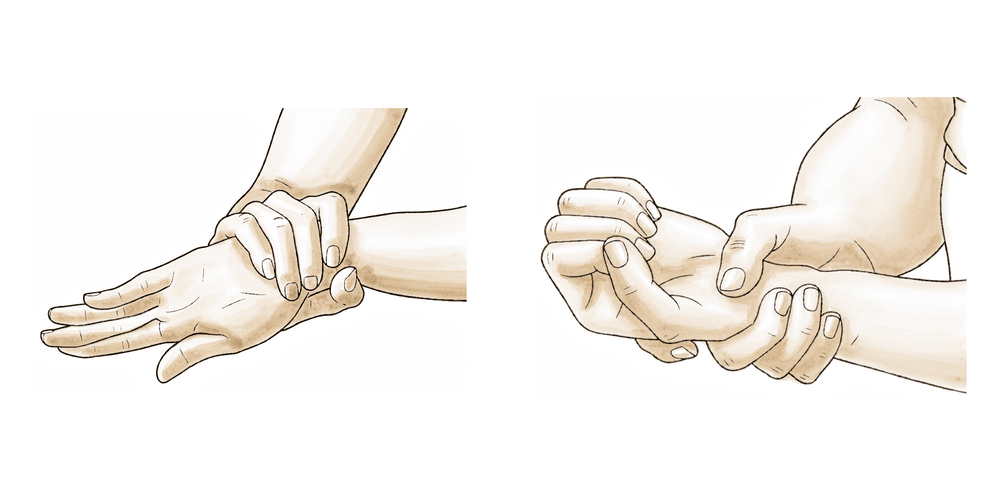
Isometric wrist extension
Rest your forearm on a table with your palm facing down and your hand over the edge. Place your other hand on the back of your sore hand. Try to lift the back of your hand towards the ceiling while your other hand holds it still, so nothing actually moves — this is a held, push-against-resistance exercise. It should feel like firm effort but should not sharply hurt. Hold the push, then relax.
Hold 30–45 seconds, 5 times, 1–2 times daily
Kieran Hirpara 4.0
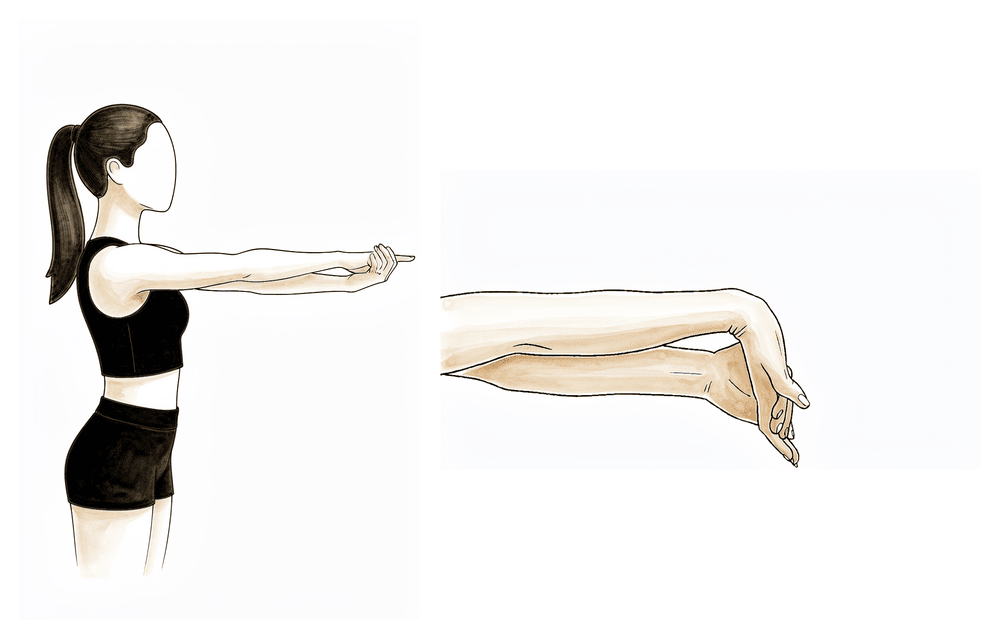
Wrist extensor stretch
Hold your sore arm out in front of you with the elbow straight and the palm facing down. With your other hand, gently bend the wrist down so the fingers point towards the floor, until you feel a comfortable pull along the top of your forearm. Keep the elbow straight. Start with the elbow slightly bent if straightening it is too sharp, and progress to a fully straight elbow as it eases.
Hold 30 seconds, 3 times, 2–3 times daily
Kieran Hirpara 4.0
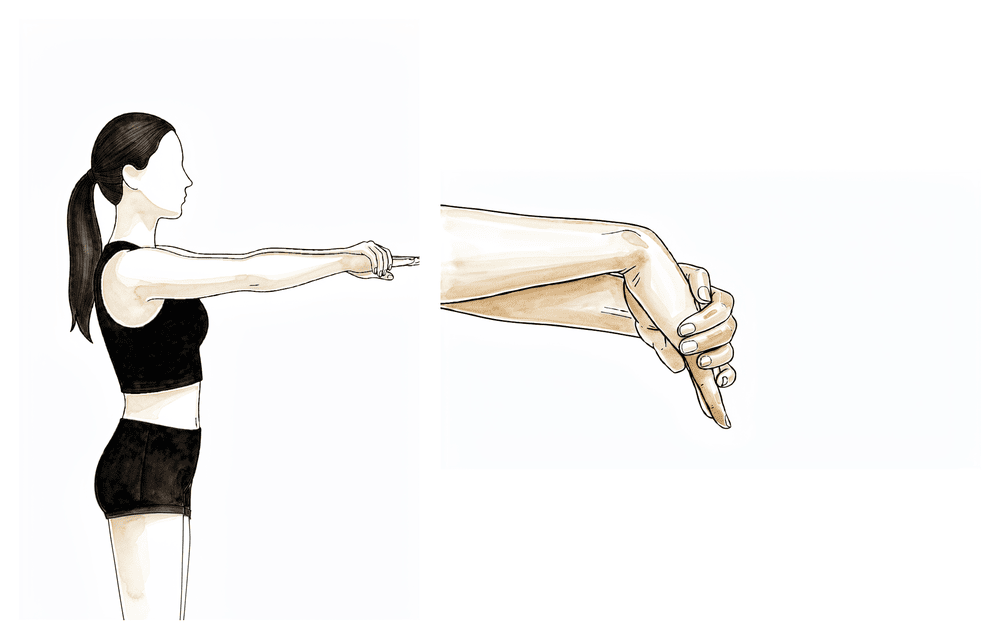
Wrist flexor stretch
Hold your arm out in front of you with the elbow straight and the palm facing up. With your other hand, gently pull the fingers and wrist back and down until you feel a comfortable pull along the underside of your forearm. Keep the elbow straight.
Hold 30 seconds, 3 times, 2–3 times daily
Kieran Hirpara 4.0
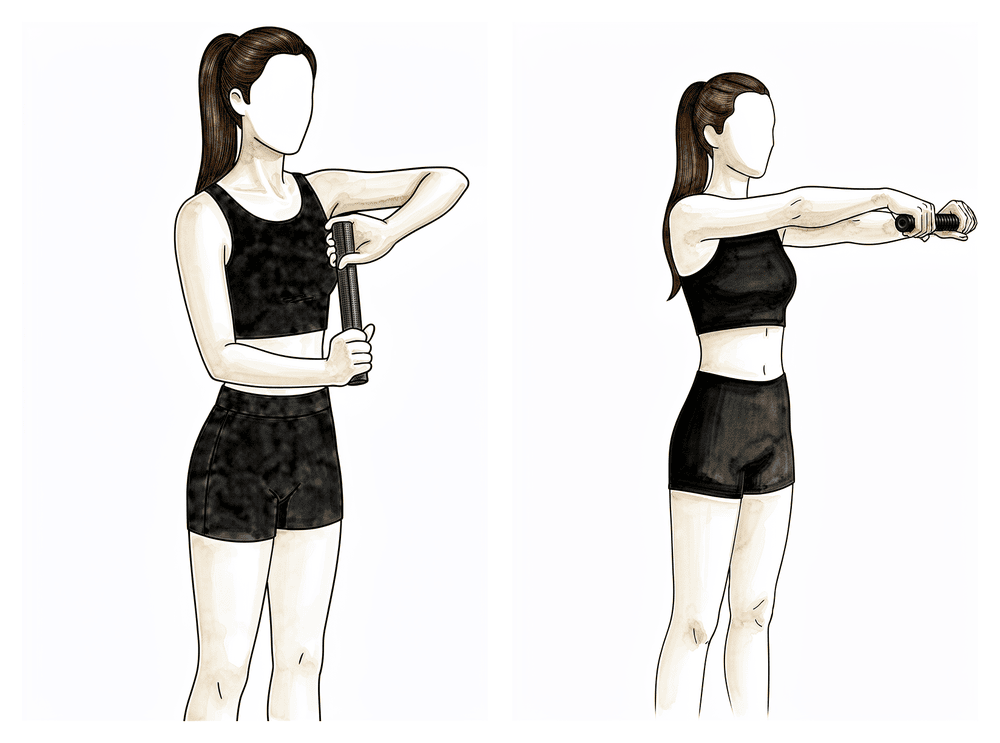
Tyler twist (eccentric wrist extension)
Hold a flexible rubber bar (FlexBar) vertically in your sore hand with the wrist bent back. Grip the top of the bar with your other hand and twist it. Now bring the bar in front of you, keeping the twist, and slowly let your sore wrist uncurl under control over 3–4 seconds — this slow, controlled lowering is the part that builds the tendon. The unwinding should feel like work, but not sharp pain. Mild ache during and a little afterwards is expected and is fine.
3 sets of 15, once daily (the core strengthening exercise)
Kieran Hirpara 4.0
Forearm rotation
Tuck your elbow into your side and bend it to a right angle. Slowly rotate your forearm so the palm faces up, then turn it so the palm faces down, keeping the elbow tucked in. As it gets easier, hold a light weight such as a hammer or a tin to add load.
10 each direction, 2–3 times daily; add light weight as able

Kieran Hirpara 4.0
Grip strengthening
Squeeze a soft ball or therapy putty in your hand, hold the squeeze briefly, then relax. Build up the firmness of the squeeze gradually as your tendon tolerates more. If gripping is still very sore, start later and lighter — grip work belongs in the strengthening phase, once the early irritation has settled.
10–15 squeezes, 2–3 times daily; progress firmness as tolerated
These are the exercises from your handout. They follow the recovery in order: the counterforce brace and isometric holds help settle pain early, the stretches keep the forearm supple, and the Tyler twist, forearm rotation and grip work build the tendon back up. Start them as guided by Dr Hirpara and your therapist, and do not feel you must do all of them from day one; your therapist will tell you which to begin with and when to add the strengthening exercises.
Your clinical protocol¶
The rest of this page is the clinical rehabilitation protocol for lateral epicondylitis (tennis elbow). This section is to be provided to your physiotherapist or hand therapist, and each phase opens with a plain-English explanation of what is happening.
The protocol has two arms: a non-operative pathway (first-line for essentially everyone) and a post-operative pathway for the small number who undergo ECRB debridement after failing six or more months of quality conservative care.
Non-operative pathway¶
The core principle is progressive tendon loading, guided by pain. The aim is to shorten the symptomatic course and restore load tolerance, not to rest the tendon.
Phase I — Acute / pain control (0–2 weeks)¶
The focus here is settling pain and restoring unloaded movement. There is no immobilisation; this is relative rest, not casting.
For your physiotherapist:
- Goals: settle pain; restore full unloaded active range of motion (AROM).
- Management: activity modification, joint protection and ergonomic advice. Optional counterforce brace over the common extensor mass to offload the ECRB origin during grip; a wrist (cock-up) splint may be used if acutely painful with extension activities. Adjuncts to settle pain: ice, soft-tissue / instrument-assisted soft-tissue mobilisation (IASTM), gentle pain-free AROM, optional dry needling, nerve glides.
- Criteria to progress: full unloaded AROM without pain; independent with the home program.
Phase II — Sub-acute / early loading (2–4 weeks)¶
Tendon loading begins gently, and the proximal chain (shoulder blade and rotator cuff) is addressed, because weakness higher up the arm drives overload at the elbow.
For your physiotherapist:
- Goals: begin tendon loading; address the proximal kinetic chain.
- Exercises: isometric wrist extensor and flexor loading (light load; isometrics are well tolerated and analgesic in reactive tendinopathy); progressive stretching of the wrist flexors and extensors with the elbow at 90°; proximal work: serratus anterior, middle/lower trapezius, rotator cuff and scapular stabilisers.
- Criteria to progress: full ROM maintained; tolerates the stretch at 90° elbow flexion; approximately 70% of contralateral grip/strength.
Phase III — Strengthening / return (4–6+ weeks, often running to 12 weeks)¶
This is where the tendon is rebuilt and load tolerance for work and sport is restored. Eccentric–concentric loading is the core therapeutic driver.
For your physiotherapist:
- Goals: restore load tolerance and sport/work capacity.
- Exercises: eccentric–concentric loading of wrist extension and forearm pronation/supination; the Tyler twist (FlexBar) is the prototypical home eccentric tool. Progress stretching to the elbow-extended position; mobilisation-with-movement (Mulligan). Grip strengthening and task-/sport-specific loading; plyometrics for athletes. Gradually wean the counterforce brace as the patient becomes asymptomatic. Equipment modification for athletes (grip size, string tension, technique).
- Criteria to progress (return to sport): approximately 90% of contralateral strength, pain-free function, and self-management competence.
Post-operative pathway (ECRB debridement ± release)¶
Surgery is reserved for the ~4–11% who fail ≥6 months of quality conservative care. Open Nirschl-type debridement and arthroscopic ECRB debridement give comparable results. The timeline below follows the Brigham & Women's Standard of Care for lateral epicondyle debridement.
Phase 1 — Protect (Days 1–7)¶
A sling is used for comfort only in the first week.
For your physiotherapist:
- Sling for comfort; ice 20 minutes, 2–3 times daily; an elbow pad over the incision.
- Gentle pain-free hand, wrist and elbow AROM; active shoulder ROM; periscapular exercises.
- Minimise ADLs that stress the extensor mechanism (lifting, combined full-elbow-extension with wrist flexion); lift palm-up to offload the extensors; optional wrist splint if acutely painful.
Phase 2 — Early motion (Weeks 2–4)¶
For your physiotherapist:
- Discontinue the sling. Begin PROM and active-assisted motion within pain tolerance.
- Gentle strengthening: active motion and sub-maximal isometrics. Commence scar management.
Phase 3 — Strengthening (Weeks 5–7)¶
For your physiotherapist:
- Advance resistive strengthening (weights / Theraband), emphasising wrist-extensor endurance (light load, higher reps). Restore full active and passive ROM.
- Introduce counterforce bracing to the common extensor tendon (with education to avoid nerve compression); gentle cross-fibre massage; begin functional preparation.
Phase 4 — Functional / return (Weeks 8–12)¶
For your physiotherapist:
- Task-specific functional training; return to higher-level work and recreational activity.
- Continue the counterforce brace as needed for pain-free ADLs and strengthening.
Getting back to work and activity¶
If you are treating tennis elbow without surgery, there is no fixed "off work" period; you can keep using the arm throughout, modifying the heaviest gripping and lifting tasks and using a counterforce brace to get through them. The realistic expectation is that the elbow settles over 6–12 months, with most people (80–90%) better within a year. It is a slow tendon problem, so progress is measured over weeks and months, not days. Sticking with the loading program is what gets you there; flare-ups along the way are normal and are not a setback as long as a mild ache settles by the next day.
If you have had surgery, the sling is for comfort only in the first week and is discarded as the elbow settles. Strengthening builds through weeks 5–7, and most people make a functional return to work and recreation around weeks 8–12. Heavier and sport-specific demands are reintroduced gradually within that window, guided by how the tendon tolerates load.
Return to sport (for both pathways) is guided by reaching roughly 90% of the strength of your other arm, with pain-free function and confidence to self-manage, rather than by the calendar alone.
After your protocol¶
This protocol works alongside the practice's general recovery advice; see managing post-operative pain and, if you have had surgery, wound care and hand therapy basics. The phased plan above reflects current best evidence for tennis elbow (progressive tendon loading rather than rest), and your ongoing recovery is guided individually by your physiotherapist or hand therapist according to how your elbow progresses.
Evidence & references
Lateral Epicondylitis (Tennis Elbow) — Non-operative & Post-operative Rehabilitation¶
Topic scope: (A) the natural history and stepped non-operative management of lateral epicondylitis (relative rest → progressive tendon loading: isometric → eccentric–concentric; counterforce bracing; controversies around corticosteroid and PRP injection), and (B) post-operative rehabilitation after open or arthroscopic ECRB debridement ± release, reserved for the minority who fail ≥6 months of quality conservative care.
Defining principle: despite the "-itis" suffix, lateral epicondylitis is a degenerative tendinopathy (tendinosis) of the extensor carpi radialis brevis (ECRB) origin, not an inflammatory condition. This reframes treatment away from rest and anti-inflammatory measures and toward progressive tendon loading — settle pain with isometrics, then rebuild load tolerance with eccentric–concentric loading (the Tyler twist / FlexBar). KH's stance: load the tendon, do not immobilise it; corticosteroid injection is avoided as first line because it is better short-term but worse at 6–12 months; surgery is a last resort after ≥6 months of genuine conservative care.
A. NATURAL HISTORY & NON-OPERATIVE MANAGEMENT¶
Natural history (self-limiting in most)¶
Lateral epicondylitis is self-limiting in the majority: roughly 80–90% resolve within about one year regardless of treatment, with the conservative literature ranging out to 12–18 months [Coonrad & Hooper 1973; Nirschl 1999]. This high spontaneous-resolution rate is the central methodological challenge of the field — any intervention must beat natural history, a high bar most fail to clear. The goal of therapy is therefore to shorten the symptomatic course and restore load tolerance, not to "cure" a condition that largely settles on its own.
Phased non-operative rehabilitation¶
First-line for essentially all comers. The therapeutic core is progressive tendon loading guided by pain.
Phase I — Acute / pain control (~0–2 weeks). Relative rest, NOT immobilisation — avoid full wrist/elbow casting (Nirschl). Activity modification, joint protection, ergonomics. Optional counterforce brace over the common extensor mass (offloads the ECRB origin during grip) ± a wrist cock-up splint if acutely painful. Adjuncts: ice, soft-tissue/IASTM, pain-free AROM, optional dry needling, nerve glides. Criterion to progress: full unloaded AROM without pain; independent with home program. Consensus / institutional protocol.
Phase II — Sub-acute / early loading (~2–4 weeks). Begin isometric wrist flexor/extensor loading (minimal load; isometrics are well tolerated and analgesic in reactive tendinopathy). Progressive stretching of wrist flexors/extensors with the elbow at 90°. Add proximal kinetic-chain work (serratus anterior, mid/lower trapezius, rotator cuff, scapular stabilisers — proximal deficits drive distal overload). Criteria to progress: full ROM maintained; tolerates stretch at 90° elbow flexion; ~70% contralateral grip/strength. Moderate (strengthening trials) / Consensus (timeline).
Phase III — Late / strengthening & return (~4–6+ weeks, often to 12 weeks). Eccentric–concentric loading of wrist extension and forearm pronation/supination is the core driver; the Tyler twist (FlexBar eccentric wrist-extension) is the prototypical home tool. Progress stretching to the elbow-extended position; add mobilisation-with-movement (Mulligan). Grip strengthening and task-/sport-specific loading; plyometrics for athletes. Gradually wean the counterforce brace as the patient becomes asymptomatic. Return-to-sport criteria: ~90% contralateral strength, pain-free function, self-management competence. Moderate–High (RCT/SR for exercise & loading) / Consensus (phase timings).
B. POST-OPERATIVE REHABILITATION (open or arthroscopic ECRB debridement ± release/repair)¶
Surgery is reserved for the ~4–11% who fail ≥6 months (commonly 6–12 months) of quality conservative care. Open Nirschl-type debridement and arthroscopic ECRB debridement give comparable complication and reoperation rates (national database, Arthroscopy 2022); arthroscopy additionally allows intra-articular inspection. The phased timeline below is the Brigham & Women's Standard of Care for lateral epicondyle debridement, cross-checked against community ECRB-release protocols.
| Phase | Window | Sling / support | Motion & strengthening | Notes |
|---|---|---|---|---|
| 1 — Protect | Days 1–7 | Sling for comfort; optional wrist splint if painful | Pain-free hand/wrist/elbow AROM; active shoulder ROM; periscapular work | Ice 20 min 2–3×/day; elbow pad over incision; lift palm-up to offload extensors |
| 2 — Early motion | Weeks 2–4 | Discontinue sling | PROM + active-assisted motion within pain tolerance; sub-maximal isometrics | Begin scar management |
| 3 — Strengthening | Weeks 5–7 | Introduce counterforce brace | Advance resistive strengthening (weights/Theraband); wrist-extensor endurance (light load, high rep); restore full A/PROM | Education to avoid nerve compression; cross-fibre massage |
| 4 — Functional / return | Weeks 8–12 | Counterforce brace as needed | Task-specific functional training; return to work/recreation | Functional return wk 8–12 |
Alternative published timelines (community ECRB-release protocols): wrist splint full-time 0–2 wk with no strengthening; full ROM goal by 4–6 wk; strengthening + transition to counterforce brace
6 wk; full activity ~8–10+ wk. Note: one comparative series found post-op bracing/immobilisation delayed symptom resolution versus PRP (mean time to full ROM 96 days surgery vs 42 days PRP) — reinforcing that early controlled motion, not protection, is the goal.
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Corticosteroid injection: better short-term, WORSE long-term. The Bisset/Smidt body of work (and the BMJ 2006 mobilisation-with-movement RCT) shows steroid gives early relief but higher recurrence and worse 6–12-month outcomes than physiotherapy or wait-and-see. Some authors now call it "always inadvisable" for lateral elbow (Orthop Trauma Surg Res 2019). Prior injection is associated with eventual surgery (a proxy for severity). Strong (Level-1 RCT).
- PRP / autologous blood: contested. Some Level-1 RCTs (Peerbooms 2010; Gosens 2-yr) show PRP superior to corticosteroid with ongoing 2-year benefit; others (Krogh 2013) found PRP ≈ glucocorticoid ≈ saline (no benefit over placebo). Meta-analyses are heterogeneous. Net: a reasonable second-line for refractory cases, but evidence is inconsistent. Conflicting (Level-1).
- Eccentric vs concentric vs isometric. Pure eccentric (Alfredson-style) is effective but not clearly superior; current view favours eccentric–concentric combined loading, with isometrics for early analgesia. Grip/isometric demands of the elbow differ from the Achilles, so blanket extrapolation of eccentric-only protocols is questioned. Moderate.
- Surgical indication/timing & technique. Reserve for failure of ≥6 months conservative care. Open vs arthroscopic debridement: no significant difference in complication or reoperation rates (national database, Arthroscopy 2022); choice is surgeon-/training-dependent. Repair after debridement vs debridement alone remains unsettled. Surgical incidence is declining, attributed to eccentric-exercise protocols and injections. Moderate.
- Self-limiting nature complicates all evidence: ~80–90% resolve within a year regardless of treatment, so any intervention must beat natural history. Strong (natural-history signal).
D. EVIDENCE STRENGTH FLAGS (summary)¶
- MODERATE–HIGH (RCT / SR): progressive loading (eccentric / eccentric–concentric) and exercise therapy for non-operative lateral epicondylitis; mobilisation-with-movement (BMJ 2006); the natural-history signal (~80–90% resolve within ~1 year).
- MODERATE (cohorts / database): post-operative ECRB debridement outcomes; equivalence of open vs arthroscopic debridement (no difference in complication/reoperation rates).
- CONSENSUS / institutional (Level-5): the phase timelines themselves derive from Standard-of-Care protocols (Brigham & Women's, Mass General Brigham, Campbell's/Nirschl) — broadly concordant across sources but not trial-derived.
- STRONG (against, Level-1): corticosteroid injection as first-line — better short-term, worse at 6–12 months.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Bisset L et al. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ. 2006. DOI: 10.1136/bmj.38961.584653.AE
- Krogh TP et al. Treatment of lateral epicondylitis with platelet-rich plasma, glucocorticoid, or saline: a randomized, double-blind, placebo-controlled trial. Am J Sports Med. 2013. DOI: 10.1177/0363546512472975
- Peerbooms JC et al. Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial. Am J Sports Med. 2010. DOI: 10.1177/0363546509355445
- Gosens T et al. Ongoing positive effect of platelet-rich plasma versus corticosteroid injection in lateral epicondylitis: a double-blind randomized controlled trial with 2-year follow-up. Am J Sports Med. 2011. DOI: 10.1177/0363546510397173
- Ortega-Castillo M, Medina-Porqueres I. Effectiveness of the eccentric exercise therapy in physically active adults with symptomatic shoulder impingement or lateral epicondylar tendinopathy: a systematic review. J Sci Med Sport. 2016. DOI: 10.1016/j.jsams.2015.05.010
- Nirschl RP, Ashman ES. Elbow tendinopathy: tennis elbow. Clin Sports Med. 2003. (Current Concepts — Tendinosis of the Elbow, J Bone Joint Surg Am. 1999. DOI: 10.2106/00004623-199902000-00016)
- Coonrad RW, Hooper WR. Tennis elbow: its course, natural history, conservative and surgical management. J Bone Joint Surg Am. 1973. DOI: 10.2106/00004623-197355060-00002
- Lattermann C et al. Arthroscopic debridement of the extensor carpi radialis brevis for recalcitrant lateral epicondylitis. J Shoulder Elbow Surg. 2010. DOI: 10.1016/j.jse.2010.02.008
Lateral epicondylitis literature (URLs)¶
- Comparative efficacy and safety of nonsurgical treatment options for enthesopathy of the ECRB: a systematic review and meta-analysis of randomized trials. Am J Sports Med. 2018. https://pubmed.ncbi.nlm.nih.gov/29268037/
- Eccentric, eccentric–concentric, and eccentric–concentric + isometric training in lateral elbow tendinopathy. J Hand Ther. 2017. https://pubmed.ncbi.nlm.nih.gov/28732560/
- Role of strengthening during nonoperative treatment of lateral epicondyle tendinopathy. J Hand Ther. 2021. https://pubmed.ncbi.nlm.nih.gov/33041157/
- Chronic lateral elbow tendinopathy managed with a supervised graded exercise protocol. J Hand Ther. 2023. https://pubmed.ncbi.nlm.nih.gov/36127241/
- Management of lateral epicondylitis. Orthop Traumatol Surg Res. 2019. https://pubmed.ncbi.nlm.nih.gov/30414784/
- No difference in complication or reoperation rates between arthroscopic and open debridement for lateral epicondylitis: a national database study. Arthroscopy. 2022. https://pubmed.ncbi.nlm.nih.gov/34838651/
- Wang D et al. Trends in surgical practices for lateral epicondylitis among newly trained orthopaedic surgeons. Orthop J Sports Med. 2017. https://pubmed.ncbi.nlm.nih.gov/28840148/
- Factors associated with failure of nonoperative treatment in lateral epicondylitis. Am J Sports Med. 2015. https://pubmed.ncbi.nlm.nih.gov/26015443/
Published rehab protocols (patient-guidance — basis for the phase structure)¶
- Brigham & Women's Hospital — Post-Op Protocol for Lateral Epicondyle Debridement. https://www.brighamandwomens.org/assets/bwh/patients-and-families/rehabilitation-services/pdfs/elbow-lateral-epicondyle-debridement-postoperative-bwh.pdf
- Mass General Brigham Sports Medicine — Rehabilitation Protocol for Medial/Lateral Epicondylitis (non-operative), rev. April 2021. https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-medial-lateral-epicondylitis.pdf
- Beacon Orthopaedics — Lateral Epicondylitis ECRB Surgical Release Protocol. https://www.beaconortho.com/wp-content/uploads/Lateral-Epicondylitis-Release.pdf