Patients › Rehabilitation
Total Elbow Replacement (Arthroplasty)
Recovery after a total elbow replacement: gentle assisted motion in a simple sling early, a functional movement arc as the goal, and a permanent lifelong lifting limit to protect the implant.
This protocol guides your recovery after a total elbow replacement (total elbow arthroplasty) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your physiotherapist or hand therapist: bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
A total elbow replacement removes the worn or damaged joint surfaces at the elbow and replaces them with a metal-and-plastic implant. The two halves (one anchored in your upper arm bone, the humerus, and one in your forearm bone, the ulna) are usually joined by a small hinge, which is why it is called a semi-constrained or "linked" replacement. It is most often done for severe rheumatoid arthritis, for end-stage osteoarthritis, or for certain elbow fractures in older patients where the bone cannot be repaired.
The aim of your recovery is to settle the elbow, protect the healing tissues, and restore a comfortable, pain-free functional arc of movement (enough bend and straighten to manage everyday tasks like eating, washing and dressing) rather than to make the elbow as strong as possible. For wound, swelling and scar management, see the practice's wound care guidance.
The single most important thing to understand is this: the implant is designed for comfortable daily living, not for heavy work. Its long-term enemies are wear of the plastic bearing and gradual loosening of the implant in the bone, and both are driven by heavy loading. For that reason, a vigorous strengthening program is not appropriate after a total elbow replacement, and a lifting limit stays with you for life, not just while you heal. Keeping to that limit is the single biggest thing you can do to make your new elbow last.
You will be in a simple sling for comfort after surgery, not a rigid splint or brace. Gentle assisted movement begins within the first week, and the plan builds slowly and carefully from there.
Precautions and limitations¶
Do:
- Wear your simple sling for comfort, and use it as advised.
- Begin the gentle assisted movements below within the first week, as guided by Dr Hirpara and your therapist.
- Keep your hand, wrist and shoulder moving to prevent stiffness.
- Keep to the lifelong lifting limit (below) once you have recovered.
Do not:
- Do not lift anything heavier than about a cup of tea (1 lb / 0.45 kg) with the operated arm in the first 6 weeks.
- Do not force your elbow to bend, and do not snap or push it straight.
- Do not push up out of a chair through the operated arm, carry, push or lean your weight through it, or let anyone pull or twist it.
- If your triceps muscle was lifted during surgery, do not actively straighten the elbow against resistance until your surgeon clears you (usually 6–12 weeks).
- Permanent, lifelong limits: do not repeatedly lift more than about 2 kg, and do not lift more than about 4.5–5 kg in a single effort. These limits are permanent, for life. No tennis, throwing, or impact sports, ever.
Your exercises¶
Kieran Hirpara 4.0
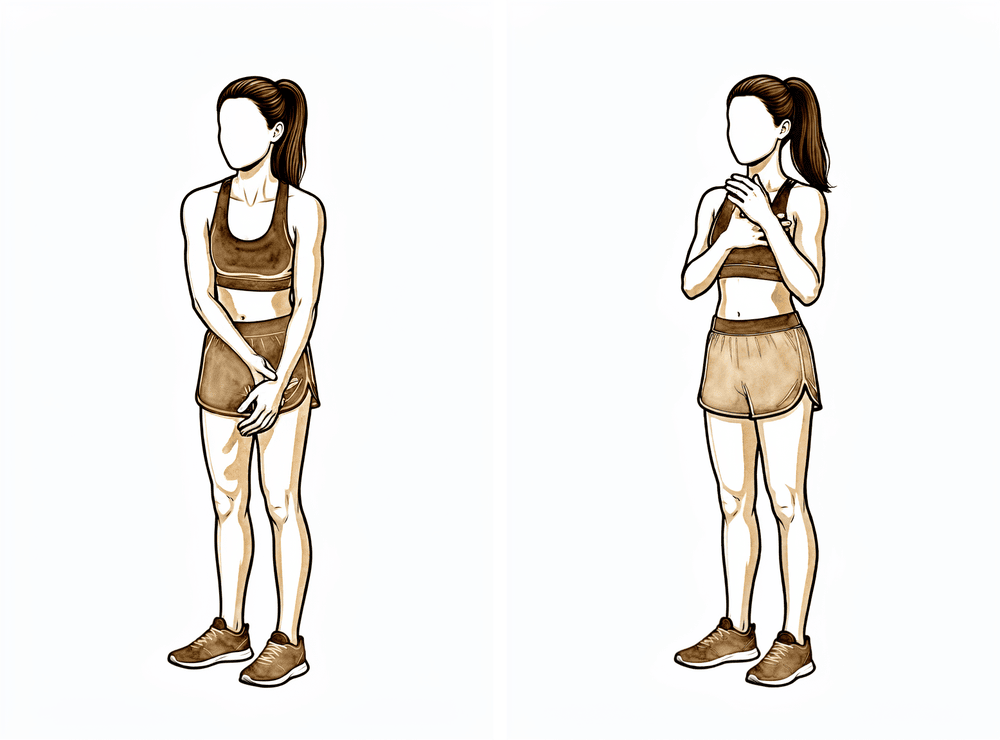
Assisted elbow bends (passive flexion)
With your upper arm tucked in at your side, use your other hand to gently help bend the operated elbow up towards your shoulder, only as far as is comfortable. Do not force it. Lower it back down slowly. Your therapist will tell you how far to go.
5–10 times, several times a day, within comfort

Kieran Hirpara 4.0
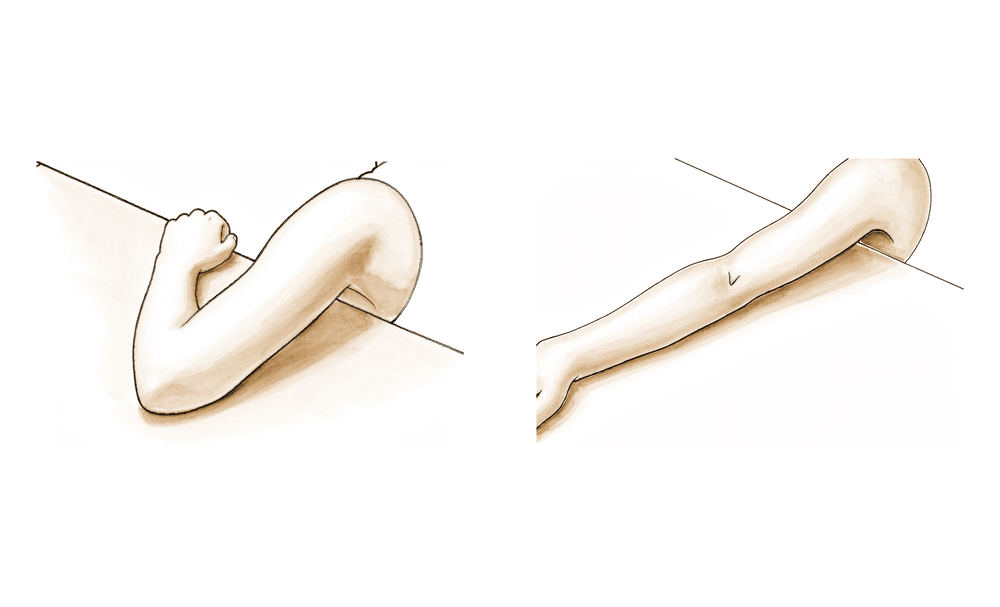
Gentle elbow bends and straightening
With your palm facing up and your upper arm tucked at your side, gently bend your elbow as far as is comfortable, then let it straighten back down with the help of gravity. Keep the movement slow and unforced — let the arm do the work, do not push hard into the ends of the range.
5–10 times, several times a day
Kieran Hirpara 4.0
Gravity-assisted elbow straightening (active extension)
Rest your upper arm supported (for example on a cushion or the arm of a chair) and let your forearm lower so the elbow gently straightens with the help of gravity. Do not snap or force the elbow straight. If your surgeon has told you your triceps muscle was lifted during surgery, keep this gentle and avoid actively pushing the elbow straight until you are cleared.
5–10 times, several times a day, within comfort
Kieran Hirpara 4.0
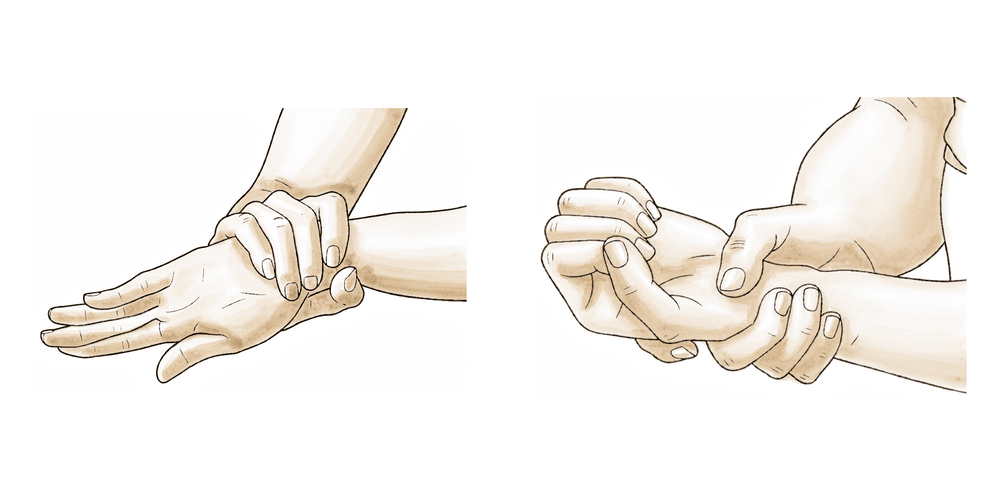
Forearm rotation (palm up / palm down)
With your elbow bent and tucked at your side, gently turn your palm up towards the ceiling, hold for a moment, then turn it down towards the floor. Keep your upper arm still so the movement comes from the forearm.
10 times each direction, a few times a day
Kieran Hirpara 4.0
Wrist movement
Gently bend your wrist forwards, then back, as far as is comfortable. This keeps your wrist and hand moving and helps prevent stiffness and swelling while your elbow heals.
10–15 times, several times a day

Kieran Hirpara 4.0
Triceps muscle tightening (isometric)
This is a later exercise — only start it once your surgeon or therapist tells you your triceps is ready, usually around 6 weeks or later. With your elbow held still at a comfortable bend, gently tighten the muscle at the back of your upper arm as if you were going to straighten the elbow, but without actually moving it. Hold gently, then relax.
Hold 5 seconds, 10 times, once cleared
These are the exercises from your handout, for gently regaining movement of your elbow, forearm, wrist and hand. Start them as guided by Dr Hirpara and your therapist. Keep every movement gentle and unforced; early on, the goal is easy, assisted motion, not effort or stretch.
Your clinical protocol¶
The rest of this page is the clinical protocol for rehabilitation after a semi-constrained total elbow replacement (posterior approach, triceps-sparing assumed). This section is to be provided to your physiotherapist or hand therapist, and each phase below opens with a plain-English explanation of what is happening.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the surgical approach, specifically whether the triceps was spared, reflected or reattached (Bryan–Morrey), as this determines the early extension restrictions and resting position.
Phase I — Immediate post-surgical, weeks 0–6¶
In the first six weeks the focus is on protecting the healing soft tissues and the triceps, settling the wound and swelling, and beginning gentle assisted motion so the elbow does not stiffen. Dr Hirpara uses a simple sling for comfort, not a posterior splint or brace. Gentle assisted (active-assisted) elbow bending and straightening begins between days 1 and 7, with the elbow held in at the side and the forearm neutral-to-pronated, using gravity to assist straightening. There is no lifting heavier than 1 lb (0.45 kg) with the operated arm, and no weight-bearing or pushing through it.
For your physiotherapist:
Immobilisation and precautions
- Simple sling for comfort (KH practice: no posterior splint or brace). If the surgeon has used a brace or splint for soft-tissue concern, follow that direction; otherwise the simple sling is worn for about six weeks, coming off for exercises and hygiene.
- Triceps-reflected / reattached cases (e.g. Bryan–Morrey): immobilise nearer extension, and avoid active and resisted elbow extension early to protect the repair (cf. distal-triceps-repair logic).
- No forced flexion (stresses the triceps repair) and no sudden or forced extension.
- No upper-limb weight-bearing, no pushing against resistance, no varus/valgus stress.
- No lifting of objects > 1 lb (0.45 kg) with the operated arm.
Exercises
- Gentle active-assisted ROM (AAROM) elbow flexion/extension from day 1–7, elbow adducted to the side, forearm neutral-to-pronated; gravity-assisted extension stretch.
- Active range of motion for the hand, wrist and shoulder to prevent stiffness.
Criteria to progress to Phase II: wound healed, pain controlled, and gentle AAROM established. Do not progress to strengthening before 6 weeks.
Phase II — Functional activity, from 6 weeks (not before)¶
This phase begins gentle muscle activation and, later, very light strengthening, but never a vigorous program. Movement is built up towards a functional arc, and resistance is introduced cautiously and kept light. The lifting restriction continues throughout.
For your physiotherapist:
Timeline within Phase II
- 6 weeks: begin submaximal, pain-free isometrics at mid-range, in all planes. If the triceps was reflected/reattached, confirm it is cleared before adding extension isometrics.
- 8 weeks: progress to multi-angle submaximal isometrics, avoiding end-range.
- 10–12 weeks: introduce light isotonic strengthening (no weights or resistance > 5 lb (2.3 kg)), single-plane first, then composite.
Range-of-motion goal
- Functional arc: 30–120/130° flexion, with 60° pronation and 60° supination.
- If flexion is < 120° by 10–12 weeks, consider a dynamic or static-progressive splint.
Precautions
- Continue to avoid heavy loading, pushing and impact.
- Strengthening philosophy (verbatim): "The need for a vigorous strengthening program is not appropriate following total elbow arthroplasty."
Criteria to progress: a pain-free functional arc is achieved and maintained.
Late Phase II and lifelong, from 12 weeks¶
From around 12 weeks the elbow moves to a maintenance home program to keep the pain-free functional arc. There is no formal heavy strengthening, ever. The lifelong activity and lifting limits below now apply permanently.
For your physiotherapist:
- Home program to maintain the pain-free functional arc.
- Reinforce the permanent activity restrictions with the patient.
- Consider discharge once a stable, comfortable functional arc and suitable return of daily function are achieved.
Getting back to work and activity¶
Your new elbow is built for comfortable everyday living, and the limits below are permanent; they are what make the implant last.
- Lifting (for life): do not repeatedly lift more than about 2 kg (a couple of full mugs), and do not lift more than about 4.5–5 kg in a single effort (around a full kettle), with the operated arm, ever. In the first 6 weeks the limit is much stricter: nothing heavier than about 1 lb (0.45 kg).
- Sport and impact: no tennis, throwing, or impact loading at any point, for life. Gentle, low-load activities are encouraged once you are cleared, but the elbow should never be loaded heavily or jarred.
- Driving: resume only once you are comfortable, out of the sling for driving, and can safely control the wheel. Confirm timing with Dr Hirpara at your review.
- Work: light desk-based and self-care tasks resume early within comfort. Any role involving lifting, carrying, pushing or repetitive arm loading needs to be discussed individually with Dr Hirpara, as the lifelong limits apply at work too.
Keeping faithfully to these limits is the single biggest thing you can do to protect your replacement and avoid loosening or wear over the years.
After your protocol¶
This protocol works alongside the practice's general recovery advice; see managing post-operative pain and wound care. Your ongoing recovery is guided individually by your physiotherapist or hand therapist according to how your elbow progresses, and your lifelong activity limits should be kept in mind at every review.
Evidence & references
Total Elbow Arthroplasty (TEA) — Rehabilitation Evidence¶
Topic scope: post-operative rehabilitation after semi-constrained (linked/hinged) total elbow replacement — most commonly for rheumatoid arthritis, end-stage osteoarthritis, or a non-reconstructable distal humerus fracture in an elderly patient. This brief covers the phased rehabilitation timeline, the early triceps-protection rationale, the functional-arc goal, and — critically — the lifelong lifting restriction that exists to protect the implant against polyethylene wear and aseptic loosening.
Defining principle: unlike most joint replacements, the goal of TEA rehabilitation is a pain-free functional arc (~30–130° flexion, 60°/60° rotation), not maximal strength. The implant's long-term enemies are polyethylene wear and aseptic loosening, both driven by load, so heavy loading is restricted permanently, not just during healing — "the need for a vigorous strengthening program is not appropriate following total elbow arthroplasty." Dr Hirpara's practice: a simple sling for comfort (not a posterior splint or brace), gentle active-assisted motion from day 1–7, isometrics from ~6 weeks, light isotonic (≤ 5 lb) from 10–12 weeks, triceps protection where the triceps was reflected or detached, and a lifelong lifting limit (no repetitive lift > ~2.3 kg; no single lift > ~4.5–5 kg; no tennis/throwing/impact ever).
Consensus phased timeline (week windows)¶
Anchored to the Brigham & Women's Hospital (BWH) Total Elbow Arthroplasty Protocol (Thornhill; semi-constrained, hinged/linked prosthesis; posterior triceps-sparing approach assumed) and cross-checked against the primary literature. Dr Hirpara's practice substitutes a simple sling for comfort in place of BWH's 60° posterior resting splint; the ROM and strengthening cadence and the lifelong limits are retained.
| Phase | Window | Sling / immobilisation | ROM and use | Strengthening | Lifting |
|---|---|---|---|---|---|
| I — Immediate post-surgical | Weeks 0–6 | Simple sling for comfort (KH — no posterior splint/brace); triceps-reflected cases immobilised nearer extension | Gentle AAROM flexion/extension from day 1–7, elbow adducted, forearm neutral-to-pronated, gravity-assisted extension; hand/wrist/shoulder AROM | None | No lifting > 1 lb (0.45 kg); no weight-bearing/pushing |
| II — Functional activity | From 6 weeks (not before) | Sling weaned | 6 wk: submaximal mid-range isometrics, all planes · 8 wk: multi-angle submaximal isometrics (avoid end-range) · target functional arc 30–120/130°, 60°/60° | 10–12 wk: light isotonic, no resistance > 5 lb (2.3 kg), single-plane → composite | Restriction continues |
| Late II / lifelong | 12 weeks onward | — | Maintain pain-free functional arc | No vigorous strengthening — ever | Lifelong limits apply (see below) |
Triceps-protection note. Where the triceps is reflected (Bryan–Morrey) rather than spared, early rehabilitation is stricter — immobilisation nearer extension and delayed/limited active and resisted extension to protect the reattachment (cf. distal-triceps-repair logic). Wiesel keeps the elbow in full extension ~24–36 h then begins active-assisted ROM, and adds no pushing/overhead for 3 months to protect the triceps; Wolfe & Ranawat's osteo-anconeus flap is immobilised ~16 days. Triceps insufficiency is a recognised TEA complication.
CRITICAL — lifelong lifting restriction numbers + sources¶
| Source | Repetitive limit | Single-event limit | Lifelong? |
|---|---|---|---|
| BWH Standard of Care (Thornhill) | no repetitive lifts > 5 lb | no single lift > 15 lb | yes — "no heavier than 15 lb for life"; "no tennis or throwing for life" |
| Wiesel, Operative Techniques in Orthopaedic Surgery (2011) | > 5 lb (~2.3 kg) | > 10 lb (~4.5 kg) | yes (also no pushing/overhead × 3 months to protect triceps) |
| Toulemonde et al., Int Orthop 2015 (100 semi-constrained TEA) | > 1 kg | 5 kg | yes; all weight-lifting avoided entirely for the first 3 months |
| Kumar & Mahanta, Indian J Orthop 2013 | — | 5 kg | permanent restriction of strenuous activity |
Bottom line / patient-facing range: the canonical teaching is a lifelong restriction of roughly ~5 lb (2.3 kg) repetitive and ~10–15 lb (4.5–5 kg) single event. The exact ceiling varies by source: BWH allows up to 15 lb once; Wiesel caps single lift at 10 lb; the European series (Toulemonde) is most conservative at 1 kg repetitive / 5 kg single. Dr Hirpara quotes the conservative patient-facing range: do not repetitively lift more than ~2 kg, or lift more than ~5 kg in a single event, for life; no tennis/throwing/impact ever.
Key controversies / evidence quality¶
- Lifting-limit variation. Numbers range from 1 kg / 5 kg (Toulemonde 2015) to 5 lb / 15 lb (BWH). The restriction exists to protect against polyethylene wear and aseptic loosening, the dominant long-term failure mode — hence its permanence.
- Triceps-sparing vs reflected approach. Surgical handling of the triceps dictates early rehab: triceps-sparing (BWH default) permits earlier gentle AAROM; reflected approaches require protecting the reattachment with immobilisation nearer extension and delayed active/resisted extension. Triceps insufficiency/weakness is a recognised complication.
- Longevity and compliance. TEA was historically reserved for elderly low-demand patients owing to implant-longevity concerns (survivorship ~85–96% at 5 y, ~70–92% at 10 y in RA). As indications expand to younger, more active and post-traumatic patients, non-compliance with activity limits drives higher complication and failure rates — which is precisely why the lifelong limit is emphasised to every patient.
Evidence strength flags¶
- MODERATE–STRONG (published protocol + restriction numbers): the BWH institutional Standard of Care provides an explicit phased timeline with verbatim lifting limits, independently corroborated by multiple peer-reviewed primary sources (JBJS, JHS, JSES, Int Orthop, JAAOS) for the lifelong restriction and the triceps-protection rationale.
- MODERATE (ROM / strengthening cadence): phase timings and the isometric → light-isotonic progression are consensus/expert-driven; no high-level RCT dictates the rehab cadence. The exact lifting ceiling varies by source.
- CONSENSUS: the simple-sling (vs posterior-splint) choice and the precise functional-arc targets reflect surgeon practice and institutional protocols rather than trial data.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Toulemonde J, Ancelin D, Azoulay V, et al. Complications and revisions after semi-constrained total elbow arthroplasty: a mono-centre analysis of 100 cases. Int Orthop. 2015. (1 kg repetitive / 5 kg single; no weight-lifting first 3 months)
- Kumar S, Mahanta S. Primary total elbow arthroplasty. Indian J Orthop. 2013. (5-kg weight-lifting restriction)
- Schoch B, Wong J, Abboud J, et al. Results of total elbow arthroplasty in patients less than 50 years old. J Hand Surg Am. 2017. (longevity/survivorship driving the restriction)
- Seitz WH, Evans PJ, Bismar H, Peers S. Complications of total elbow arthroplasty in nonrheumatoid patients. J Hand Surg Am. 2014. (active patients, poor compliance → complications)
- Baghdadi YM, Veillette CJ, Malone AA, et al. Total elbow arthroplasty in obese patients. J Bone Joint Surg Am. 2014;96(9). (higher failure with high BMI)
- Barlow JD, Morrey BF, O'Driscoll SW, et al. Activities after total elbow arthroplasty. J Shoulder Elbow Surg. 2013;22(6):787–791.
- You D, King G, Dehghan N, et al. Optimizing outcomes in total elbow arthroplasty. J Am Acad Orthop Surg (JAAOS). 2025. (modern failure-reduction review)
- Burnier M, Nguyen NTV, Morrey ME, et al. Revision elbow arthroplasty using a proximal ulnar allograft with allograft triceps for combined ulnar bone loss and triceps insufficiency. J Bone Joint Surg Am. 2020;102(22). (triceps insufficiency complication)
- Na K, Song S, Lee Y, et al. Modified triceps fascial tongue approach for primary total elbow arthroplasty. J Shoulder Elbow Surg. 2018;27(5):887–893. (triceps weakness after TEA; approach effect)
- Wolfe SW, Ranawat CS. The osteo-anconeus flap: an approach for total elbow arthroplasty. J Bone Joint Surg Am. 1990;72(5). (triceps-continuity-preserving approach; ~16-day immobilisation)
- Ring D. Instability after total elbow arthroplasty. Hand Clin. 2008. (triceps/LCL reattachment and stability)
- Wiesel SW. Operative Techniques in Orthopaedic Surgery. 2011. (5 lb repetitive / 10 lb single; full-extension splint 24–36 h; no pushing/overhead × 3 months to protect triceps)
Published protocol (web)¶
- Brigham & Women's Hospital, Department of Rehabilitation Services. Total Elbow Arthroplasty Protocol (J. Sayles OTR/L, R.B. Wilcox III PT; reviewer T.S. Thornhill MD; 2010). https://www.brighamandwomens.org/assets/bwh/patients-and-families/rehabilitation-services/pdfs/elbow-total-elbow-arthroplasty-bwh.pdf
- Brigham & Women's Hospital — Physical Therapy Standards of Care index. https://www.brighamandwomens.org/patients-and-families/rehabilitation-services/physical-therapy-protocols