Patients › Rehabilitation
Wrist Ganglion Excision
An early-motion recovery plan after excision of a dorsal or volar wrist ganglion, using minimal immobilisation then prompt movement of the wrist in every direction to prevent the stiffness that is the most common problem after this operation.

This protocol guides your recovery after surgical removal (excision) of a wrist ganglion, a fluid-filled cyst that grows out of the wrist joint, with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist; bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
A wrist ganglion is a balloon-like, fluid-filled cyst that is connected by a narrow stalk to the lining of the wrist joint. Most appear on the back of the wrist (a dorsal ganglion); some appear on the front, thumb-side (a volar ganglion). At operation, Dr Hirpara removes the cyst together with its stalk, down to the wrist joint capsule, taking the root as well as the lump, because leaving the stalk behind is the main reason a ganglion can come back. The operation can be done open (through a small incision) or with keyhole (arthroscopic) instruments.
Because nothing has been repaired or reconstructed (a cyst has simply been removed), there is no healing tendon or ligament that needs to be protected for weeks. The recovery is therefore an early-motion plan, and its whole purpose is to get the wrist moving promptly:
- Stiffness is the most common problem after this operation, far more than the cyst coming back. The wrist that is rested too long after a ganglion excision can lose movement.
- So immobilisation is kept to a minimum: a soft dressing, sometimes with a light wrist splint just for comfort, for only a few days up to a week or two. Then you move the wrist early, in every direction.
Your fingers, which are not operated on, keep moving fully from day one. Movement of the wrist is opened up as the wound settles, then grip and load are built back gradually. Most people are back to ordinary activity by around four to six weeks.
Precautions and limitations¶
- Keep your fingers, thumb and elbow moving fully from day one; only the wrist needs any easing-in.
- Wear the soft dressing or comfort splint only as long as directed (commonly a few days up to one to two weeks). It is for comfort, not to hold the wrist still for a long time; early movement is the goal here, not rest.
- Do NOT soak the wound or get the dressing wet until you are told the wound is sealed; keep it clean and dry.
- Hold off on heavy gripping, lifting and load-bearing through the wrist for the first few weeks, and build them back gradually rather than all at once.
- If you had a volar (front-of-wrist) ganglion, the cyst can sit close to the radial artery (a pulse you can feel at the front of the wrist); let the rooms know promptly if you notice unusual swelling, coldness or colour change in the hand.
- Do NOT drive until you can comfortably control the wheel and are out of any splint, as confirmed at your review.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises¶
Kieran Hirpara 4.0
Wrist movement (all directions)
Gently move your wrist in every direction — bend it back (up), bend it forward (down), and tilt it side to side — moving it as far as is comfortable each way. This is the most important early exercise, because the wrist tends to stiffen after this operation, and moving it early keeps it supple. Do it slowly and stay within comfort; it should not be sharply painful.
10 times in each direction, 4-5 times a day, from the first few days
Kieran Hirpara 4.0
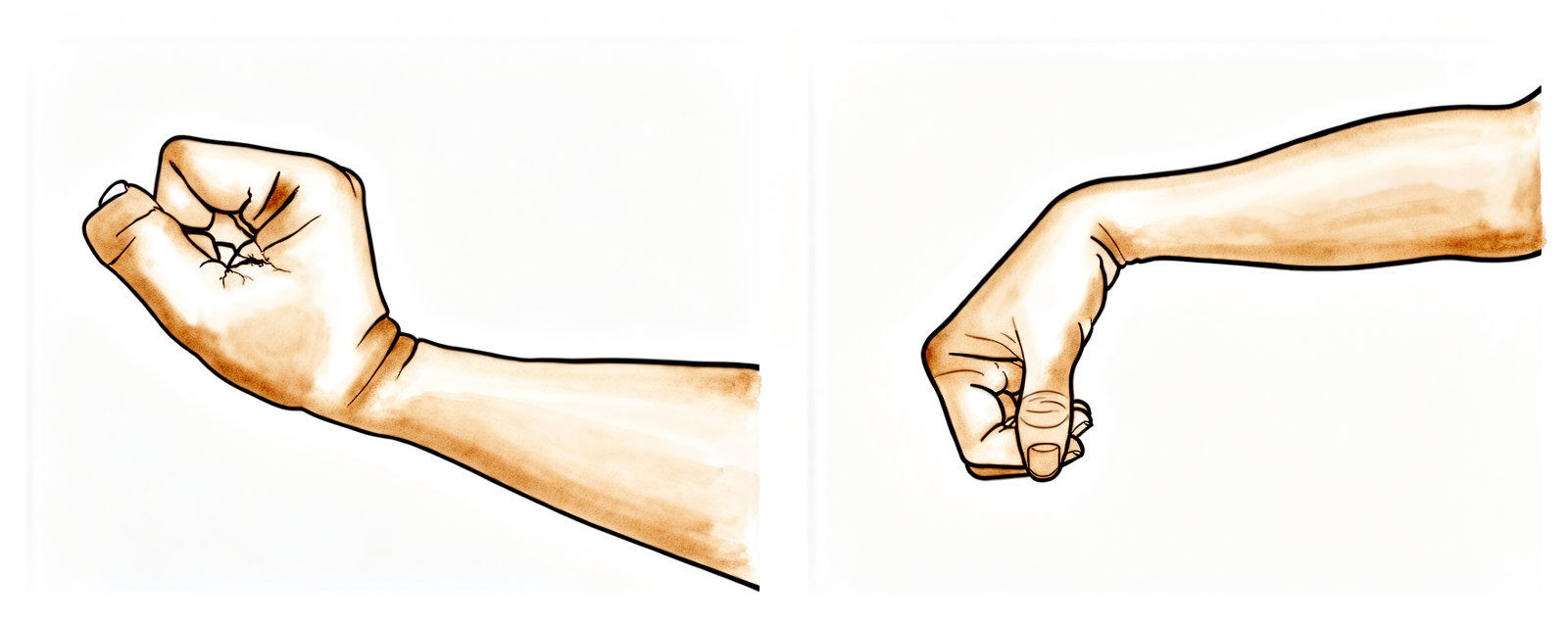
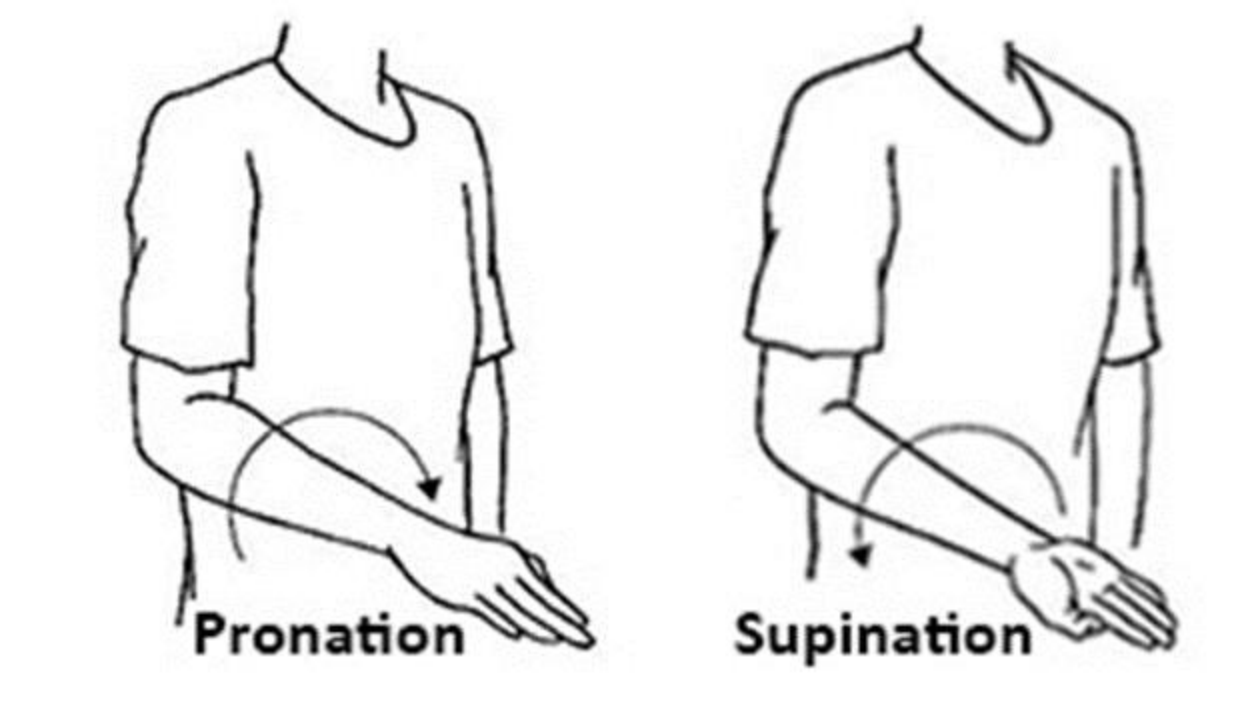
Forearm rotation (palm up / palm down)
Tuck your elbow in at your side and bend it to a right angle. Slowly turn your palm up towards the ceiling, then down towards the floor. Keep the elbow still so the movement comes from the forearm. This keeps the forearm and wrist turning freely while the wound settles.
10 times each direction, 3-4 times a day
Kieran Hirpara 4.0
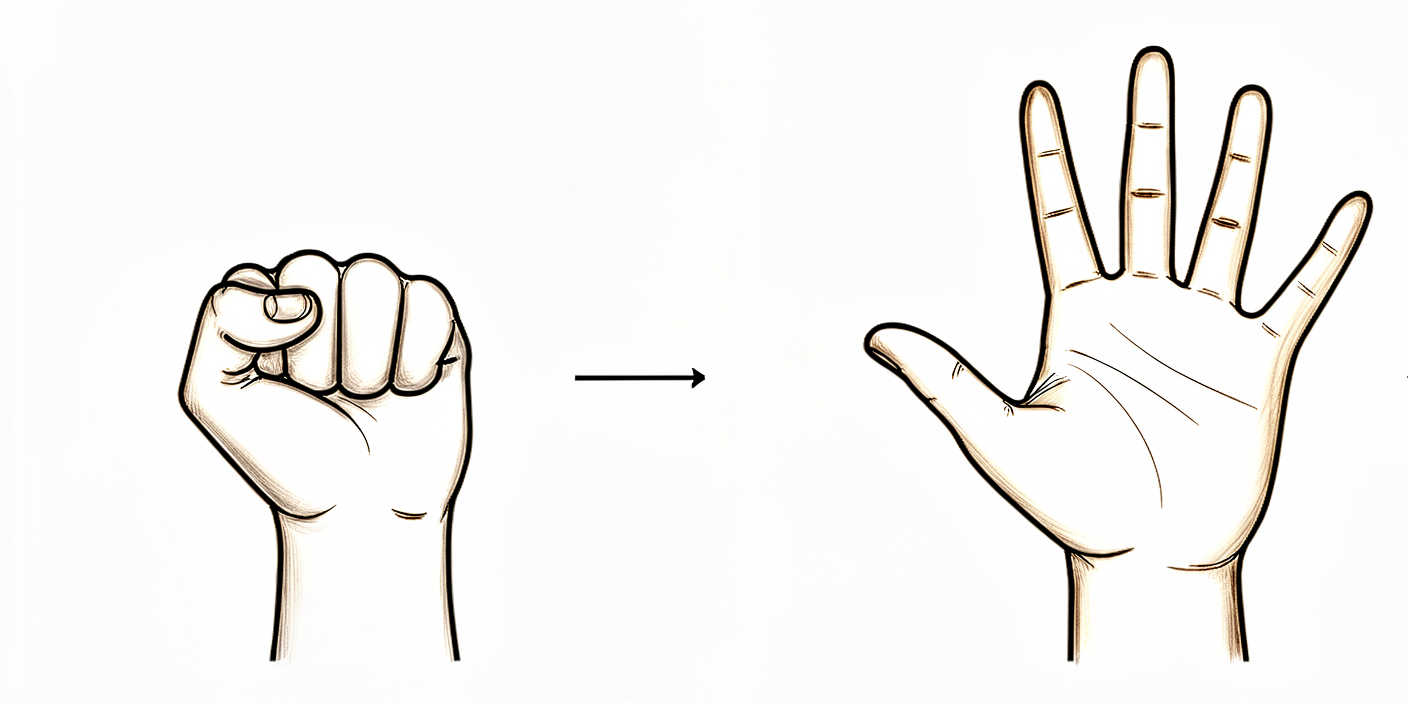
Finger movement
Make a full, slow fist so the fingertips curl into the palm, then open the hand and straighten the fingers out completely. The fingers are not operated on, so keep them moving fully from day one — this stops the hand stiffening and helps swelling drain away.
10 times, several times a day, from day one
Kieran Hirpara 4.0
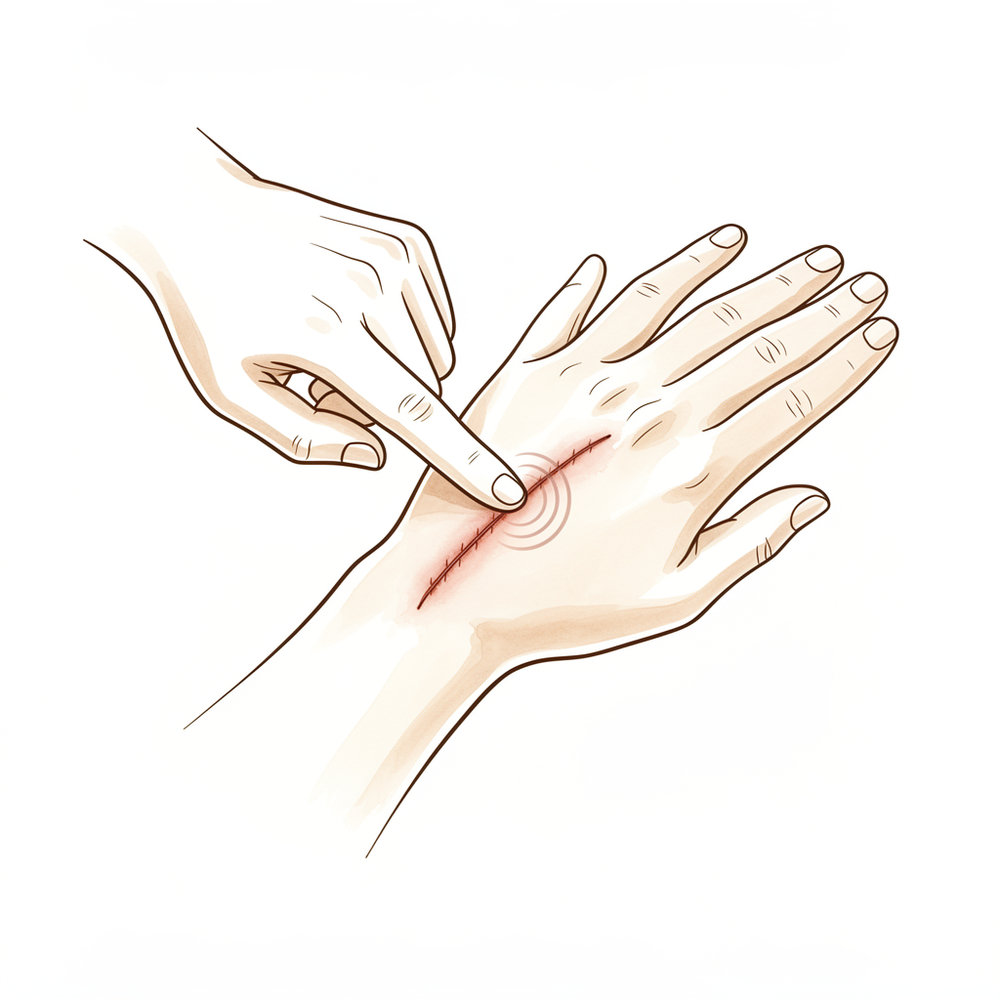
Scar massage
Once the wound is fully healed and the dressings are off (usually around two weeks), rub a little plain moisturiser into the scar with your fingertip, using small firm circles for a few minutes. This keeps the scar soft and mobile and stops it sticking to the tissues underneath, which can otherwise hold the wrist back. Do not start this on an unhealed or weepy wound.
A few minutes, twice a day, once the wound is fully healed

Kieran Hirpara 4.0
Grip strengthening
A LATER exercise, usually from around three to four weeks once the wound is settled and movement is comfortable. Squeeze a soft ball or therapy putty in your palm, hold for a few seconds, then relax. Build it up gradually. This restores the grip strength that often dips for a few weeks after the operation.
10-15 squeezes, 2-3 times a day, from around 3-4 weeks
These are the exercises from your handout. Start them as guided by Dr Hirpara and your hand therapist. The early exercises (wrist movement in all directions, forearm rotation and finger movement) are the heart of this recovery and begin within the first few days, because moving the wrist early is what prevents the stiffness that otherwise follows this operation. Scar massage starts once the wound is fully healed, and grip strengthening is added a little later as comfort allows. None of these should be sharply painful; ease off anything that is.
Your clinical protocol¶
The rest of this page is the staged clinical protocol for rehabilitation after wrist ganglion excision. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. This is an excision, not a repair: there is no construct to protect, so the governing principle is minimal immobilisation followed by early active wrist motion in all planes to prevent post-excision stiffness, which is the most common complication after this procedure.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the location (dorsal vs volar), the surgical approach (open vs arthroscopic), the integrity of the dorsal/volar capsule, and any concurrent finding. Dr Hirpara excises the cyst with its stalk down to the joint capsule. For volar ganglia, note the proximity of the radial artery. There is no protected arc and no construct to off-load; the only deliberate restraint is a short window of heavy-grip/load avoidance while the soft tissues settle.
Phase I — minimal immobilisation and early motion (days 0 to ~14)¶
The first phase protects the wound while getting the wrist moving early. Immobilisation is deliberately brief (a soft dressing, with a light wrist splint for comfort only if needed), and the wrist begins active motion in all directions within the first few days. The systematic-review evidence is that limited immobilisation of two weeks or less, or none at all, does not meaningfully change the outcome, while prolonged rest risks stiffness.
For your hand therapist:
Education and precautions - Soft dressing, with an optional light wrist splint for comfort only; wean over days, not weeks - No prolonged rigid immobilisation: limit any splinting to ≤2 weeks (commonly a few days) - Keep the wound clean and dry until sealed; full finger, thumb and elbow ROM from day one - Volar cases: be alert to the radial artery; report vascular concerns promptly
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle hand pump, ice as needed - Exercises: active wrist ROM in all planes (flexion/extension, radial/ulnar deviation) within comfort, started in the first few days; active/passive forearm pronation–supination; full active finger and thumb ROM; gentle shoulder ROM
Criteria to progress - Wound healing; settling oedema; improving, comfortable wrist arc; splint (if used) discontinued by ~2 weeks
Phase II — restoring full motion and scar management (weeks ~2 to 4)¶
From around two weeks the dressings are off and the wound is healed. The focus is regaining full, symmetrical wrist movement before stiffness has a chance to set in, and starting scar work so the scar stays mobile and does not tether the wrist.
For your hand therapist:
Assessments - Active and passive wrist ROM (compare to the other side); forearm rotation; oedema; wound/scar review
Education and precautions - Drive towards full wrist ROM in all planes; address any early loss promptly with active and gentle passive work - Begin scar management once the wound is fully healed (massage, silicone/moisturiser, desensitisation as needed) - Light functional hand use encouraged; defer heavy gripping and loading
Management - Exercises: progress to full active and gentle passive wrist ROM; continue forearm rotation; commence scar massage and desensitisation; light putty/grip work introduced toward the end of this phase as comfort allows
Criteria to progress - Full or near-full pain-free wrist ROM; healed, mobile scar; ready for graded loading
Phase III — strengthening and return to activity (weeks ~4 to 6 and beyond)¶
Once movement is restored, grip and load are built back gradually. For most patients ordinary activity returns by around four to six weeks; heavier manual demands follow a criterion-based progression.
For your hand therapist:
Assessments - Grip and pinch strength versus the other side; wrist ROM; response to graded loading; functional/work-specific testing as appropriate
Education and precautions - Progress grip and wrist strengthening (putty, ball, graded resistance) as comfort allows - Reintroduce lifting and load-bearing through the wrist gradually; full return guided by symptoms, not the calendar
Management - Exercises: progressive grip/pinch and wrist strengthening; graded loading and task-specific work; continue any residual mobility and scar work - Consider discharge once ROM is full, strength is near-symmetrical and function has returned - Consider referral back to the treating doctor if the wrist plateaus stiff, or if a recurrent swelling appears
Criteria for return to full activity - Full pain-free wrist ROM; near-symmetrical grip; comfortable with task- and work-specific loading
Getting back to work and activity¶
Light everyday hand use (eating, writing, light self-care) is encouraged from the start within comfort, and your fingers should be working fully from day one. Desk and light duties are often possible within a few days to a week or so, especially with the dominant hand free; jobs that involve heavy gripping, lifting or repeated forced wrist movement take longer and are built back over the first few weeks. Published series report only a short time off work after ganglion excision (on the order of about two weeks), though this varies with the side operated on and the demands of your job.
Because you must be able to comfortably control the wheel and be out of any splint, plan for help with transport in the very early days; driving resumes once you are comfortable and safe, as confirmed at your review. Most people are back to ordinary activity by around four to six weeks, with heavier manual work and sport built back gradually as movement and grip return, judged by how the wrist is doing, not by the calendar alone.
After your protocol¶
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and scar management. The phased plan above reflects published guidance after wrist ganglion excision, where the priority is early movement to prevent stiffness; your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your wrist progresses.
Evidence & references
Wrist Ganglion Excision — Procedure Outcomes & Post-operative Rehabilitation (Dorsal / Volar, Open or Arthroscopic)¶
Topic scope: post-operative rehabilitation after surgical excision of a wrist ganglion — removal of the cyst together with its capsular stalk down to the wrist joint, performed open or arthroscopically, for a dorsal (scapholunate-origin) or volar (radiocarpal/scaphotrapezial) ganglion. This is an excision, not a reconstruction: nothing is repaired or tightened, so the rehab is an early-motion pathway built around minimal immobilisation, prompt wrist movement in all planes, and scar care — not months of protected healing.
Defining principle of the rehab here: ganglion excision removes a cyst and its stalk; it does not create a construct that needs protecting. The most frequent adverse outcome is therefore not failure of any repair but wrist stiffness / loss of motion, which prolonged immobilisation makes worse. So the deliberate stance is minimal immobilisation (soft dressing ± brief comfort splint, ≤2 weeks) followed by early active wrist motion in every plane, with the only restraint a short window of heavy-grip/load avoidance while the soft tissues settle. The principal branch points are (1) dorsal vs volar (volar ganglia sit adjacent to the radial artery and carry a higher neurovascular-complication profile) and (2) open vs arthroscopic access (similar recurrence; arthroscopic may have a gentler early course). Importantly, the recurrence and outcome literature is far better developed than the rehabilitation literature, which is largely expert-consensus and low-level.
A. PROCEDURE OUTCOMES (open vs arthroscopic; dorsal vs volar)¶
Ganglion excision is a reliable, low-morbidity operation. The principal outcome debate is over recurrence and over access (open vs arthroscopic), not over whether excision works.
- Excision markedly out-performs aspiration for durable cure. Pooled across treatments, mean recurrence is roughly 6% arthroscopic, ~20–21% open, ~59% aspiration; surgical excision confers a large reduction in recurrence versus aspiration. Reported open-excision recurrence is wide (0–31%), the lowest classic series (Angelides & Wallace) reporting <1% with meticulous stalk excision [Zoller 2023 JAAOS review; Gant 2011 review]. Moderate (reviews of heterogeneous series).
- Removing the stalk down to the capsule is the key technical determinant of recurrence. Leaving the capsular stalk behind is the main reason a ganglion recurs; stalk resection is repeatedly advocated as the critical step [Gant 2011; Rizzo 2004]. Mechanistic / consensus.
- Open and arthroscopic excision give similar recurrence. A retrospective comparison and a systematic review found no significant difference once low-quality/high-bias studies are excluded (pooled ~8% arthroscopic vs ~10% open); a prospective randomised dorsal-ganglion trial (Kang) reported 11% vs 9%. Arthroscopic access may offer a cosmetic/early-recovery edge but is not proven superior for recurrence [Konigsberg 2023 HAND; Crawford 2018 SR; Gant 2011 citing Kang]. Moderate (SR + retrospective + one RCT).
- Wrist stiffness is the most common complication after carpal ganglion excision, ahead of recurrence; other risks are infection, scar problems, neurovascular injury and (rarely) injury to the scapholunate ligament [Gant 2011]. Moderate (review).
- Volar ganglia carry a distinct neurovascular risk. They are adherent to / immediately adjacent to the radial artery; radial-artery injury during volar excision is described as "quite common," and an MRI-based study identifies anatomical position as a risk factor for operation-related complications after arthroscopic volar ganglionectomy [Rocchi 2008; Oh 2025 BMC; operative-technique texts]. Moderate (cohort + anatomical).
B. REHABILITATION / THERAPY EVIDENCE¶
The central rehab questions are (1) should the wrist be immobilised afterwards, and (2) does a particular therapy regimen change the outcome. The best available evidence — a systematic review of post-excision immobilisation — answers that brief or no immobilisation is appropriate, with early motion the means of preventing the dominant complication (stiffness). There is no high-level trial evidence for any specific exercise protocol; rehab content is consensus.
- Limited or no immobilisation does not worsen outcome — and protects against stiffness. A systematic review and surgeon survey of dorsal ganglion excision found practice split roughly evenly between rigid splinting and soft dressings; immobilisation durations ranged from 48 hours to 2 weeks (open) and 5 days to 3 weeks (arthroscopic). The explicit conclusion: "limited immobilization of 2 weeks or less or no immobilization after surgery does not meaningfully affect patient outcome." Prolonged rigid immobilisation is the avoidable driver of stiffness (one 2-week bulky-dressing series reported 11.5% with ≥20° ROM loss, versus normal ROM in 100% of a short-immobilisation series) [Wong 2023 HAND SR]. Moderate (systematic review of low-level studies).
- Early active wrist motion in all planes is the core of the programme. Because there is no repair to protect and stiffness is the commonest problem, the consensus is to move the wrist early through flexion/extension and radial/ulnar deviation, with full finger and forearm motion from day one. The adhesion/stiffness-prevention rationale is mechanistic and consensus rather than trial-proven. Weak–moderate (mechanism strong, outcome data absent).
- Recovery is usually quick and time off work short. Series report on the order of ~2 weeks off work after open wrist ganglion excision (longer for volar than dorsal, and longer than aspiration), with most patients back to ordinary activity by ~4–6 weeks [Suen 2013 citing Dias 2007]. Moderate (cohort).
- Recurrent ganglia are re-excisable with good function, and physical therapy is routinely recommended in re-excision series — underlining that therapy here is supportive (motion + scar), not a construct-protecting protocol [re-excision outcome series]. Low (small series).
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Minimal immobilisation & early motion | Days 0–~14 | Soft dressing ± comfort splint only (≤2 wk) | Full finger/thumb/elbow ROM from day 1; active wrist ROM in all planes within the first few days; forearm rotation; elevation for oedema | Light functional use only | Brief or no immobilisation does not worsen outcome; prolonged rest → stiffness |
| II — Restore full motion & scar care | Week ~2–4 | None routine (splint weaned) | Drive to full wrist ROM; scar massage once wound healed; desensitisation | Light grip/putty toward end | Stiffness is the complication to pre-empt; address early ROM loss promptly |
| III — Strengthening & return | Week ~4–6+ | Restrictions lifted | Progress grip/pinch + wrist strengthening; task-specific loading | Graded grip and load to symmetry | Most back to ordinary activity ~4–6 wk; manual/volar cases a little longer |
(Phase windows mirror the precautions in the patient protocol; they are typical guides, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- To splint or not. Practice is genuinely split, but the systematic-review evidence is that limited (≤2 weeks) or no immobilisation does not change outcome — and that prolonged rigid immobilisation is the avoidable cause of stiffness. This page's brief-immobilisation, early-motion default reflects that finding. Moderate (SR of low-level data).
- Open vs arthroscopic. Similar recurrence once bias is accounted for; arthroscopic may give a cosmetic/early-recovery edge. Choice is largely surgeon/patient preference. Moderate.
- What drives recurrence. Incomplete stalk excision, not rehab, is the main recurrence determinant; no mobilisation regimen has been shown to affect recurrence. Consensus / mechanistic.
- Stiffness is the real enemy, not the cyst coming back. Wrist stiffness is the commonest complication; framing recovery around early motion (rather than protective rest) is the evidence-aligned stance. Moderate.
- Volar ganglia are different. Radial-artery proximity raises the neurovascular-complication profile of volar excision; this is an operative/anatomical caution rather than a rehab variable, but it shapes early monitoring. Moderate.
- Rehab evidence is thin. Recurrence and procedure outcomes are well studied; the specific exercise programme is expert-consensus with no controlled trials. The defensible position is a simple early-motion + scar home programme with selective hand therapy. Weak / consensus.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG (RCT / SR): none specific to rehab. (Procedure-side: superiority of excision over aspiration for recurrence is robust across reviews.)
- MODERATE: systematic-review evidence that ≤2-week or no immobilisation does not worsen outcome (Wong 2023); similar recurrence open vs arthroscopic (Crawford SR, Konigsberg, Kang RCT); stiffness as the commonest complication; volar radial-artery risk; short time off work.
- WEAK / CONSENSUS: the specific early-motion, all-plane wrist ROM + scar therapy programme (mechanistically rationalised — stiffness prevention — with no controlled outcome trials); exact phase timings (typical, not trial-derived).
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Gant J, Ruff M, Janz BA. Wrist ganglions. J Hand Surg Am. 2011;36(3):510–512. DOI: 10.1016/j.jhsa.2010.11.048
- Zoller SD, Benner NR, Iannuzzi NP. Ganglions in the Hand and Wrist: Advances in 2 Decades. J Am Acad Orthop Surg. 2023;31(2). DOI: 10.5435/JAAOS-D-22-00105
- Rizzo M, Berger RA, Steinmann SP, et al. Arthroscopic resection in the management of dorsal wrist ganglions: results with a minimum 2-year follow-up period. J Hand Surg Am. 2004;29(1):59–62. DOI: 10.1016/j.jhsa.2003.10.018
- Konigsberg MW, Tedesco LJ, Mueller JD, et al. Recurrence Rates of Dorsal Wrist Ganglion Cysts After Arthroscopic Versus Open Surgical Excision: A Retrospective Comparison. Hand (N Y). 2023;18(1). DOI: 10.1177/15589447211003184
- Crawford C, Keswani A, Lovy AJ, et al. Arthroscopic versus open excision of dorsal ganglion cysts: a systematic review. J Hand Surg Eur Vol. 2018;43(6). DOI: 10.1177/1753193417734428
- Mathoulin C, Gras M. Arthroscopic Management of Dorsal and Volar Wrist Ganglion. Hand Clin. 2017;33(4). DOI: 10.1016/j.hcl.2017.07.012
- Oh W, Kim H, Kim D, et al. Anatomical location of volar wrist ganglion in preoperative MRI is a risk factor for operation-related complications after arthroscopic ganglionectomy. BMC Musculoskelet Disord. 2025;26(1). DOI: 10.1186/s12891-025-08766-x
- Gray J, Zuhlke T, Eizember S, et al. Dry Arthroscopic Excision of Dorsal Wrist Ganglion. Arthrosc Tech. 2017;6(2). DOI: 10.1016/j.eats.2016.09.018
Wrist ganglion excision & post-operative care literature (URLs)¶
- Wong CR, Karpinski M, Hatchell AC, et al. Immobilization of the Wrist After Dorsal Wrist Ganglion Excision: A Systematic Review and Survey of Current Practice. Hand (N Y). 2023;18(2):254–263. DOI: 10.1177/15589447211014631. https://pmc.ncbi.nlm.nih.gov/articles/PMC10035098/
- Suen M, Fung B, Lung CP. Treatment of Ganglion Cysts. ISRN Orthop. 2013;2013:940615. DOI: 10.1155/2013/940615. https://pmc.ncbi.nlm.nih.gov/articles/PMC4045351/
- Rocchi L, Canal A, Fanfani F, et al. Articular ganglia of the volar aspect of the wrist: arthroscopic resection compared with open excision — a prospective randomised study. Scand J Plast Reconstr Surg Hand Surg. 2008;42(5):253–259. DOI: 10.1080/02844310802210897. https://pubmed.ncbi.nlm.nih.gov/18791910/
- Ganglions — Treatment & Management (recurrence by treatment modality; surgical technique). Medscape Reference. https://emedicine.medscape.com/article/1243525-treatment