Patients › Rehabilitation
Extensor Tendon Repair
A recovery plan after repair of an extensor tendon on the back of the finger or hand (zones IV to VII), using a relative-motion (yoke) splint that lets you use the hand straight away while protecting the repair, then weaning the splint and building strength in careful stages.

This protocol guides your recovery after surgical repair of an extensor tendon (one of the tendons on the back of the finger or hand that straightens the finger) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It covers repairs across the back of the finger, hand and wrist (the zones surgeons call IV to VII). It does not cover a mallet finger (a repair right at the fingertip) or a central-slip / boutonnière repair over the middle knuckle; those follow different plans. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist. Bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
An extensor tendon repair stitches a divided tendon back together on the back of the finger or hand. The old way to protect that repair was to splint the hand still for several weeks, but that often left the fingers stiff and slow to recover. Instead, your recovery uses a clever, modern approach called relative-motion rehabilitation (the Merritt method).
The key is a small splint called a yoke, worn across the back of the hand. It holds the big knuckle of the repaired finger about 15 to 20 degrees more straightened than the knuckles of the fingers on either side. That small difference quietly takes the load off the healing tendon, so you can start using the hand straight away, gently and within comfort, instead of waiting weeks with it splinted still. Moving early in this protected way keeps the tendon gliding so it does not stick down, while the offset stops it being over-strained.
For most repairs (the common zones on the back of the finger and hand) the yoke on its own is all you need. For some repairs (those closer to the wrist, weaker repairs, or where extra protection is sensible) a wrist splint is added for the first few weeks as well. Your hand therapist will tell you if you also have a wrist splint.
The plan then opens up in careful stages: the yoke is worn full-time for about six weeks and weaned from around week five; coupled wrist-and-finger movement is added in the middle weeks; strengthening begins from about eight weeks; and full activity returns around ten to twelve weeks, once the repair is solid.
Precautions and limitations¶
- Wear your yoke splint full-time for about the first six weeks, including for exercises and everyday tasks, and only remove or wean it as your hand therapist directs. Your hand therapist will tell you if you also have a wrist splint.
- Do light everyday use of the hand in the splint from the start, within comfort. Do NOT do any lifting, forced gripping or resisted work for the first several weeks.
- Do NOT start grip or pinch strengthening until you are cleared, usually around eight weeks.
- Do NOT make a hard full fist or force the finger early; move only in the gentle, controlled ranges you are shown.
- Keep the smaller finger joints moving so they do not stiffen; gentle passive straightening helps with this.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises¶
Kieran Hirpara 4.0
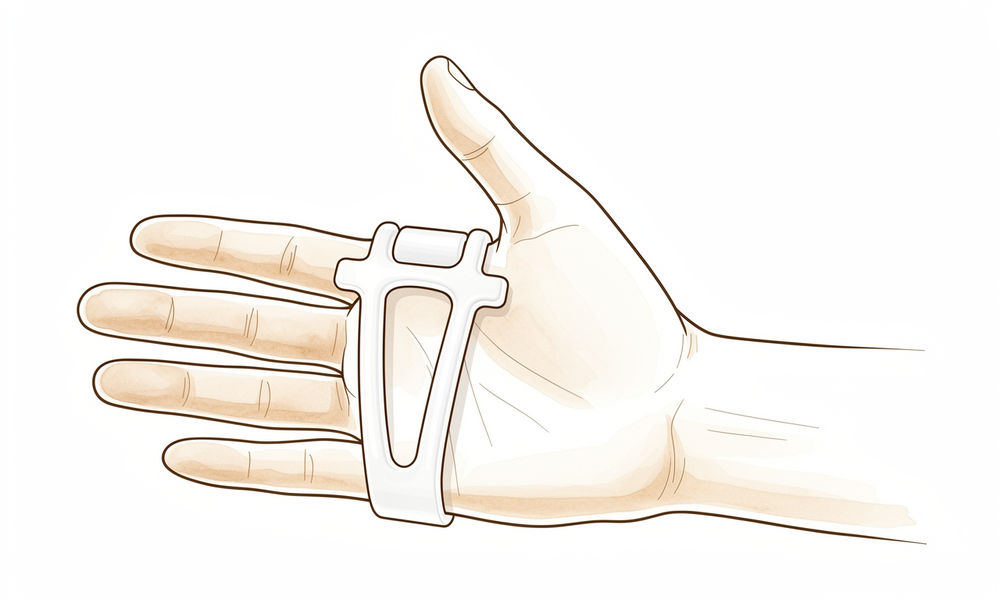
Wearing your relative-motion (yoke) splint
Your repaired finger is held in a small splint called a yoke (or relative-motion splint). It keeps the big knuckle (the MCP, where the finger meets the hand) of the repaired finger about 15 to 20 degrees more straightened than the fingers either side. This small difference takes the strain off the healing tendon, which is what lets you use the hand straight away. Wear it full-time for about six weeks — including for your exercises and for everyday tasks — and only take it off as your hand therapist directs. Your hand therapist will tell you if you also have a wrist splint.
Worn full-time for about 6 weeks, weaned from around week 5 as guided
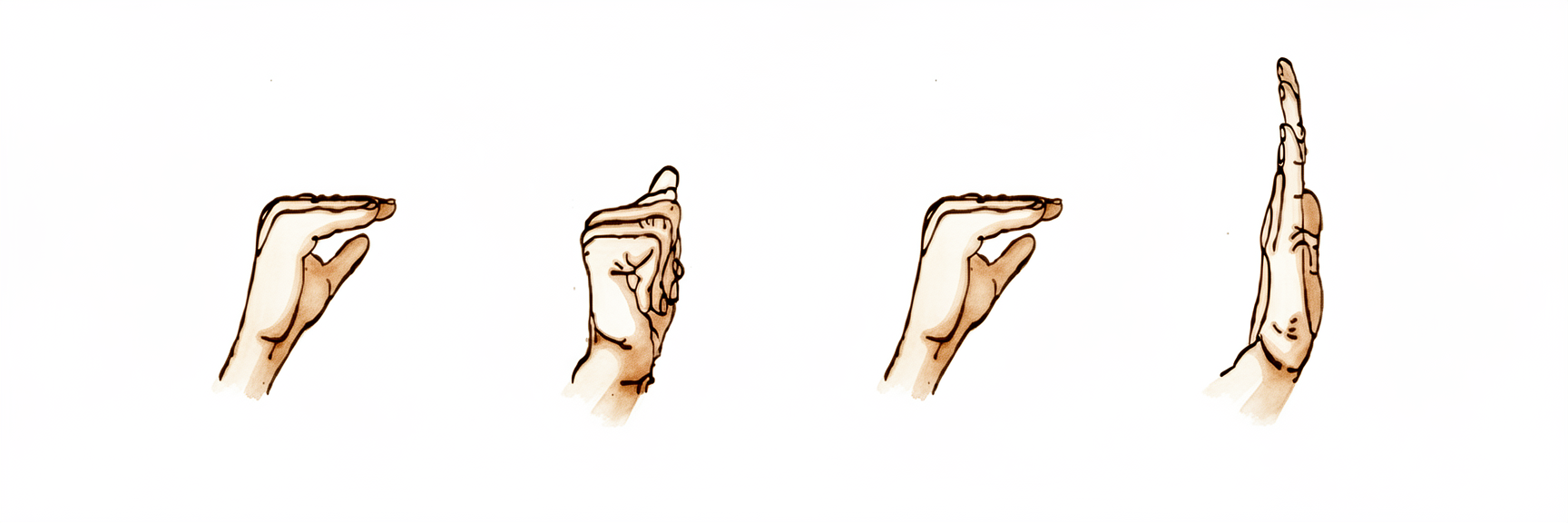
Knuckle-bend, fingers-straight (intrinsic-plus)
Keeping the splint on, bend at the big knuckles (where the fingers meet the hand) while keeping the rest of each finger straight — like making a flat 'tabletop' or 'shelf' shape. Then return to straight. Move smoothly within comfort. This glides the repaired tendon a safe, controlled amount so it does not stick down, without putting it under strain.
10 times, every couple of hours through the day

Knuckles-straight, finger-curl (intrinsic-minus / hook)
Keeping the splint on, keep your big knuckles straight and curl only the smaller joints of the fingers down into a hook (claw) shape, then straighten them again. This moves the repaired tendon through its other range, again in a safe and controlled way. Stay within comfort and do not force it.
10 times, every couple of hours through the day

Coupled wrist-and-finger motion (tenodesis)
A LATER exercise — added by your hand therapist from around three to six weeks. Gently tip the wrist back and let the fingers relax open, then let the wrist drop forward as the fingers gently close. The wrist and fingers move together as a pair. This naturally and safely glides the extensor tendons and is started once the repair is stronger.
10 times, 2 to 3 times a day (from ~3 to 6 weeks, as guided)
Kieran Hirpara 4.0
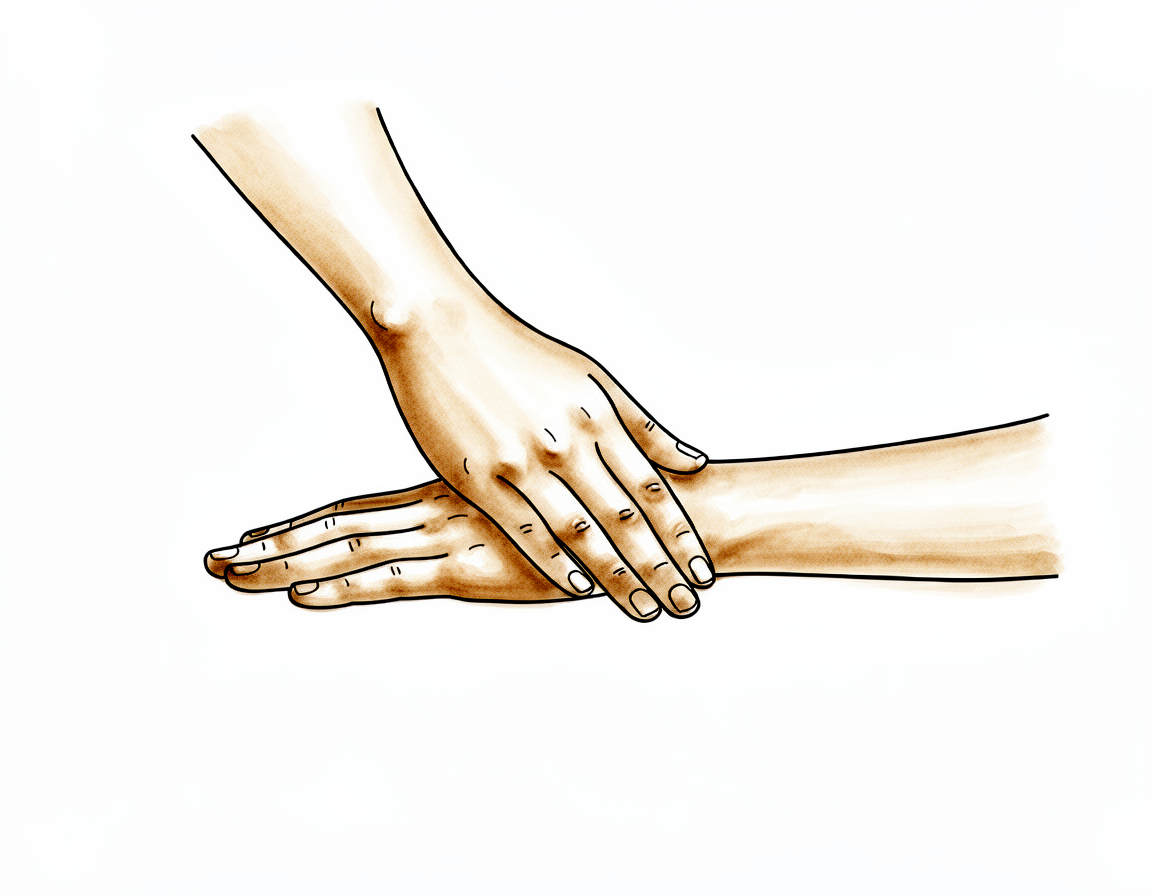
Passive finger straightening
Gently use your other hand to support and straighten the smaller joints of the repaired finger, helping it reach full straight without forcing. This keeps the finger from stiffening into a bent position while the tendon heals. Keep it gentle and pain-free, and only as your hand therapist guides.
Hold a few seconds, 5 to 10 times daily, as guided

Kieran Hirpara 4.0
Grip/pinch strengthening (from wk 8)
A LATER exercise — only from around eight weeks, once your hand therapist clears strengthening. Squeeze a soft ball or putty in the whole hand, and pinch it between your thumb and fingers, building the effort up gradually over several weeks. This rebuilds grip and pinch strength once the repair is solid. Do not start resisted gripping before you are cleared.
10 to 15 squeezes, 2 to 3 times a day (from ~8 weeks only)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever range and limits you have been given. The early exercises are done with the yoke splint on: gentle knuckle bends and finger curls that glide the repaired tendon a safe, controlled amount without straining it. The coupled wrist-and-finger movement and the grip/pinch strengthening belong to later phases and should not be started until you are specifically cleared. Stop anything that causes sharp pain over the back of the finger or hand.
Your clinical protocol¶
The rest of this page is the staged clinical protocol for rehabilitation after extensor tendon repair (zones IV to VII) using relative-motion extension (RME). This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. The repair is protected by a yoke splint that holds the repaired digit's MCP 15 to 20 degrees more extended than the adjacent digits, offloading active extensor excursion via the quadriga effect and the juncturae tendineae, so immediate active motion is safe.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the zone(s) repaired, tendon(s) involved, repair strength, and whether a supplementary wrist orthosis is indicated. Dr Hirpara's default for zones V to VI is yoke-alone (relative-motion extension splint, repaired MCP held 15–20° more extended than neighbours). A wrist orthosis (~20–25° extension, first ~3 weeks) is added for zone VII, weaker repairs, or non-compliant patients. This protocol is for dorsal extensor repairs zones IV–VII only, NOT mallet (zones I–II) or central-slip/boutonnière (zone III).
Phase I — yoke (± wrist splint), immediate active use (weeks 0 to 3)¶
The first three weeks protect the repair with the yoke while the patient uses the hand actively straight away. The relative 15–20° extension offset offloads the repair, so controlled active gliding is encouraged from the outset. Light functional use in the splint is permitted; no lifting or resisted grip.
For your hand therapist:
Education and precautions - Fit the yoke / relative-motion extension splint: repaired digit's MCP held 15–20° more extended than the adjacent digits; worn full-time - Add a wrist orthosis (~20–25° extension) for the first ~3 weeks ONLY for zone VII / weaker repairs / non-compliant patients (yoke-alone is the default for zones V–VI) - Light use of the hand in the splint is encouraged; NO lifting, forced gripping or resisted work - Avoid forced composite fisting; keep ranges controlled
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle digital pump, ice as needed - Exercises (in the splint, every ~2 h): active intrinsic-plus (MCP flexion with IPs extended) and intrinsic-minus / hook (MCP extension with IP flexion); passive IP extension daily to prevent IP stiffness - Commence scar management once the wound is healed
Criteria to progress - Wound settling; no extensor lag developing; comfortable controlled active motion in the splint at ~3 weeks
Phase II — wrist splint off, yoke continues, coupled motion (weeks 3 to 6)¶
From about three weeks any supplementary wrist splint is discontinued (the yoke continues full-time). Coupled wrist-and-finger (tenodesis) motion and composite active flexion/extension are added, increasing tendon excursion in a controlled, repair-safe way.
For your hand therapist:
Assessments - Active and passive ROM (MCP and IP), extensor lag, pain and swelling; wound/scar review
Education and precautions - Discontinue the supplementary wrist splint (if one was used); continue the yoke full-time - Progress motion gradually; still NO resisted grip or strengthening
Management - Exercises: add coupled wrist-and-finger motion (tenodesis) and composite active flexion/extension; continue intrinsic-plus / intrinsic-minus gliding and passive IP extension; light functional use in the yoke - Continue scar massage once healed
Criteria to progress - Composite active ROM progressing ~6 to 8 weeks; no extensor lag; pain settling
Phase III — wean the yoke, strengthen, return (weeks 6 to 12)¶
From around week five to six the yoke is weaned. Progressive grip and pinch strengthening begins from about eight weeks once the repair is solid, building gradually toward full activity at ten to twelve weeks.
For your hand therapist:
Assessments - Full active and passive ROM, extensor lag, grip/pinch strength versus the other side; functional and work-specific testing as appropriate
Education and precautions - Wean the yoke from ~week 5, off by around week 6 as motion and control allow - Introduce progressive grip/pinch strengthening from 8 weeks (not before) - Build resistance gradually toward full activity at 10 to 12 weeks
Management - Exercises: graded grip and pinch strengthening (ball/putty squeeze, pinch) from week 8; progressive resistance; continue any residual mobility and IP-extension work - Consider discharge once motion and strength are near-symmetrical and functional return is achieved - Consider referral back to the treating doctor if an extensor lag persists, motion plateaus, or there is a poor outcome
Criteria for return to full activity - Full painless ROM with no significant extensor lag; near-symmetrical grip/pinch; ~10 to 12 weeks
Getting back to work and activity¶
Light everyday use of the hand in the yoke splint (eating, writing, dressing, light self-care) is encouraged from the start, within comfort, as long as it does not involve lifting, forced gripping or resisted work. Strengthening begins from about eight weeks, and full, unrestricted activity returns around ten to twelve weeks once the repair is solid and your motion and strength are restored, judged by Dr Hirpara and your hand therapist, not by the calendar alone.
Driving: light use of the hand in the yoke is fine, so driving is not banned outright, but you must be able to grip the wheel and control the car safely, including in an emergency. For most people that means resuming as the yoke is weaned (around six weeks); it can be earlier if you can control the car comfortably, and your surgeon confirms when it is safe for you.
After your protocol¶
This protocol works alongside the practice's general recovery advice: see managing post-operative pain, wound care and scar management. The phased plan above reflects published rehabilitation guidance after extensor tendon repair using relative-motion extension, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your hand progresses.
Evidence & references
Extensor Tendon Repair — Procedure Outcomes & Post-operative Rehabilitation (Relative-Motion Extension, Zones IV–VII)¶
Topic scope: post-operative rehabilitation after primary repair of an extensor tendon on the dorsum of the finger, hand or wrist — zones IV to VII — managed by relative-motion extension (RME / Merritt yoke splint, the ICAM family of regimens). This is a tendon repair (a construct that must heal under controlled load), but the relative-motion approach lets that load be applied immediately and actively rather than after weeks of immobilisation. This page does not cover mallet finger (zones I–II) or central-slip / boutonnière repair (zone III), which follow different regimens.
Defining principle of the rehab here: a yoke (relative-motion) splint holds the repaired digit's MCP joint 15–20° more extended than its neighbours. By the quadriga effect and the juncturae tendineae, this small relative offset offloads the repaired tendon — it reduces the active extensor excursion demanded of the healing repair (from roughly 12 mm of excursion in normal active extension to about 6 mm within the splint). That residual ~6 mm is enough to keep the tendon gliding and prevent adhesions, but too little to rupture the repair — which is why immediate active motion is safe. The single common branch point is whether a supplementary wrist orthosis (~20–25° extension, first ~3 weeks) is added for zone VII, weaker repairs, or non-compliant patients; the yoke alone is the default for zones V–VI.
A. PROCEDURE / REPAIR OUTCOMES (relative-motion vs immobilisation)¶
Extensor tendon repair on the back of the hand is reliable; the principal modern question is how to rehabilitate it — protected immobilisation versus an early-active programme such as relative-motion extension — not whether repair works.
- The mechanism that makes immediate active motion safe is well established. The 15–20° relative MCP-extension offset offloads the repair via the quadriga effect and the juncturae tendineae, cutting active extensor excursion from ~12 mm (normal) to ~6 mm within the splint — enough to prevent adhesions, too little to rupture. Cadaveric and mechanistic work underpins this rationale [Merritt, Wong & Lalonde 2020]. Strong (mechanistic + cadaveric).
- Relative-motion regimens match or improve on traditional early-active and immobilisation pathways. A randomised controlled trial in zones V–VI found relative-motion extension delivered earlier return of hand function and higher patient satisfaction with equivalent total active motion (TAM) versus the comparator early-active programme [Collocott RCT 2020]. A systematic review reported earlier return to work with equivalent range of motion and complication rates [Collocott review 2017]. Moderate–strong (1 RCT + SR; RME studies of generally lower methodological quality).
- Yoke-alone (no wrist splint) is supported for the common zones. Case series of relative-motion extension without a supplementary wrist orthosis for zones IV–VI report no ruptures, supporting yoke-alone as the default for these zones with the wrist orthosis reserved for zone VII / weaker / non-compliant repairs [Hirth 2021; Howell ICAM]. Moderate.
- The functional gain over immobilisation is large and practical. Early-active relative-motion programmes report return to work at roughly 17–25 days, versus the 3–4 months typical of immobilisation regimens — the headline advantage that has driven adoption [Collocott review 2017; Howell ICAM]. Moderate.
B. REHABILITATION / THERAPY EVIDENCE¶
The central rehab questions are (1) immobilise or move early, (2) is a wrist splint needed in addition to the yoke, and (3) how long must the splint stay on. The evidence favours early relative motion, supports yoke-alone for zones V–VI, and suggests splint duration can be shorter than the traditional six weeks without penalty.
- Early active motion via relative-motion extension is the modern default. The original technique description [Merritt 2014] and the clinical scheduling / yoke construction work [Lutz 2015] established a reproducible programme: immediate active intrinsic-plus and intrinsic-minus motion in the yoke, progressing to coupled (tenodesis) motion, weaning, then strengthening. Moderate (technique + cohort).
- A supplementary wrist splint is optional, not mandatory. Yoke-alone case series for zones IV–VI report no ruptures; the wrist orthosis (~20–25° extension, first ~3 weeks) is added selectively for zone VII, weaker repairs, or poor compliance [Hirth 2021; Howell ICAM]. Moderate (selective use).
- Splint duration may be shortened. A comparison of 4-week versus 6-week splinting found no difference in outcome, suggesting the traditional six-week full-time period can be safely abbreviated in selected patients [Svens 2015]. This page keeps full-time wear ~6 weeks (weaned from ~wk 5) as the conservative default while acknowledging the shorter option. Moderate (1 comparative study).
- The field is moving toward wider use of relative motion. A recent international consensus endorses broader application of relative-motion rehabilitation, including beyond its original zone V–VI indication [Tang consensus 2025]. Consensus.
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Splint / restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Yoke (± wrist splint), immediate active use | Week 0–3 | Yoke full-time (repaired MCP 15–20° more extended); wrist orthosis ~20–25° ext only for zone VII / weak / non-compliant | Active intrinsic-plus (MCP flex, IPs straight) and intrinsic-minus / hook every ~2 h; passive IP extension daily; light use in the splint | Light functional use only; no lifting / resisted grip | Relative offset offloads repair (~12 mm → ~6 mm excursion); active motion is safe from day one |
| II — Wrist splint off, yoke continues | Week 3–6 | Discontinue any wrist splint; yoke continues full-time | Add coupled wrist-and-finger (tenodesis) motion + composite active flexion/extension; light functional use; scar massage once healed | Still no resisted grip | Composite active ROM building; watch for extensor lag |
| III — Wean yoke, strengthen, return | Week 6–12 | Yoke weaned from ~wk 5, off ~wk 6 | Progress full active motion; commence grip/pinch strengthening from week 8 | Graded strengthening from wk 8 → full activity ~10–12 wk | Return to work as early as ~17–25 days reported; full unrestricted activity ~10–12 wk |
(Phase windows mirror the precautions and recovery structure in the patient protocol; they are typical guides, not trial-derived deadlines. Splint duration may be safely shortened toward 4 weeks in selected patients.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Relative motion vs traditional immobilisation / other early-active regimens. One RCT (zones V–VI) and a systematic review favour relative-motion extension for earlier hand function, earlier return to work, higher satisfaction, with equivalent TAM and complications — though RME studies are generally of lower methodological quality, so the effect size is moderately rather than strongly certain. Moderate–strong.
- Wrist splint: needed or not? Yoke-alone gives good results with no ruptures in zone IV–VI series; the supplementary wrist orthosis is selective (zone VII / weaker / non-compliant). The defensible default is yoke-alone for the common zones — hence the page wording that the hand therapist will advise if a wrist splint also applies. Moderate.
- How long to splint. Traditional full-time wear is ~6 weeks; a 4-vs-6-week comparison showed no difference, so duration can be individualised and potentially shortened. Moderate.
- The 15–20° offset itself. The specific relative-extension increment is consensus-derived (it must offload enough to protect but leave enough excursion to glide); it rests on sound mechanism rather than a dose-finding trial. Consensus.
- Extending relative motion beyond zones V–VI (e.g. to sagittal-band injury and selected boutonnière/central-slip cases). The 2025 consensus endorses wider use, but evidence outside the core zones is weak–moderate, which is why this page deliberately scopes to zones IV–VII and excludes zone III. Weak–moderate.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- STRONG: the mechanism — relative 15–20° MCP-extension offset offloads the repair (quadriga + juncturae tendineae; ~12 mm → ~6 mm active excursion) making immediate active motion safe (mechanistic + cadaveric).
- MODERATE–STRONG: relative-motion extension is at least as good as other early-active-motion regimens (1 RCT zones V–VI: earlier hand function, higher satisfaction, equal TAM; SR: earlier return to work, equal ROM/complications) — tempered by the lower methodological quality of RME studies.
- MODERATE: wrist-splint-optional (yoke-alone, no ruptures in zone IV–VI series); 4-vs-6-week splint duration (no difference); return to work ~17–25 days vs 3–4 months for immobilisation.
- CONSENSUS: the specific 15–20° offset increment; broader application of relative motion (Tang 2025).
- WEAK–MODERATE: extension of the technique to sagittal-band / boutonnière (central-slip) injuries outside the core zones.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Merritt WH. Relative motion splint: active motion after extensor tendon injury and repair. J Hand Surg Am. 2014. DOI: 10.1016/j.jhsa.2014.03.015
- Merritt WH, Wong AL, Lalonde DH. Recent developments are changing extensor tendon management (relative motion / quadriga mechanism). Plast Reconstr Surg. 2020. DOI: 10.1097/prs.0000000000006556
- Lutz K, et al. Relative motion extension splinting for extensor tendon repair — clinical schedule and yoke. Hand Clin. 2015. DOI: 10.1016/j.hcl.2014.12.006
- Collocott SJF, et al. Relative motion flexion versus relative motion extension / early active motion after extensor tendon repair (zones V–VI): a randomized controlled trial. J Hand Ther. 2020. DOI: 10.1016/j.jht.2018.10.003
- Collocott SJF, Kelly E, Ellis RG. A systematic review of relative-motion orthoses for the management of extensor tendon repairs. Hand Ther. 2017. DOI: 10.1177/1758998317729713
- Svens B, et al. Four-week versus six-week immobilisation comparison after extensor tendon repair. J Hand Ther. 2015. DOI: 10.1016/j.jht.2014.07.006
- Hirth MJ, et al. Relative-motion approaches in extensor tendon rehabilitation. J Hand Ther. 2021. DOI: 10.1016/j.jht.2019.12.016
- Tang JB, et al. International consensus on relative-motion rehabilitation and extensor tendon management. J Hand Surg (Eur Vol). 2025. DOI: 10.1177/17531934251363138
Extensor tendon rehabilitation literature (URLs)¶
- Howell JW, Merritt WH, Robinson SJ. Immediate Controlled Active Motion (ICAM) following zone 4–7 extensor tendon repair. J Hand Ther / PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3574475/