Patients › Rehabilitation
Medial Epicondylitis (Golfer's Elbow)
Loading-based rehabilitation for golfer's elbow (flexor-pronator tendinosis), with ulnar-nerve screening, eccentric reverse-Tyler-twist loading, and a separate post-operative pathway for the minority who need surgery.

This page guides your recovery from medial epicondylitis (commonly called golfer's elbow) under the care of Dr Kieran Hirpara at Mater Private Hospital Rockhampton. Most people recover fully without surgery, and the cornerstone of treatment is a steady, loading-based exercise program rather than rest. It begins with your home exercise program, followed by the structured clinical protocol written for your physiotherapist or hand therapist; bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your therapist may adjust the plan depending on how your recovery progresses.
If you develop pins-and-needles, numbness or weakness in your little and ring fingers, let the rooms or your therapist know; the ulnar nerve runs right behind the inner elbow and sometimes needs separate attention.
What to expect¶
Golfer's elbow is a wear-and-tear (degenerative) problem of the tendons on the inner side of the elbow: the flexor-pronator tendons, which bend the wrist and turn the palm down, where they attach to the bony bump called the medial epicondyle. Despite the old name "epicondylitis", it is not really an inflammation; the tendon has become weakened and disorganised from overload. That is why the modern treatment is not rest and anti-inflammatories, but a graded program that gently loads the tendon back to full strength.
Recovery takes patience. Golfer's elbow is generally self-limiting, but it can take 6 to 18 months to fully settle. The good news is that the great majority of people get better with a good conservative program and never need an operation. Surgery is only considered after at least six months of quality therapy has failed.
One feature that makes the inner elbow different from the outer (tennis) elbow is the ulnar nerve (the "funny bone" nerve), which runs in a groove immediately behind the medial epicondyle. Around half of people with golfer's elbow also have some irritation of this nerve, so your therapist will check it at each visit and may add specific nerve-gliding exercises.
Precautions and limitations¶
Do:
- Keep using the arm for normal daily tasks within comfortable limits.
- Modify, rather than completely stop, the activities that flare it up.
- Wear a counterforce brace over the forearm muscle during aggravating activity if it helps.
- Do your stretches and loading exercises regularly; consistency matters more than intensity.
Do not:
- Do not rest the elbow completely or put it in a cast; the tendon needs gentle load to heal.
- Avoid the heavy valgus-loading activities early on: golf, throwing (especially the cocking and acceleration phases), swimming and racquet sports, until your strength is rebuilt.
- Do not push any exercise into sharp pain, and do not push nerve glides into pins-and-needles or numbness.
- If your ulnar nerve symptoms (tingling or numbness in the little and ring fingers) get worse, ease back and seek review before progressing your loading.
Your exercises¶
Kieran Hirpara 4.0
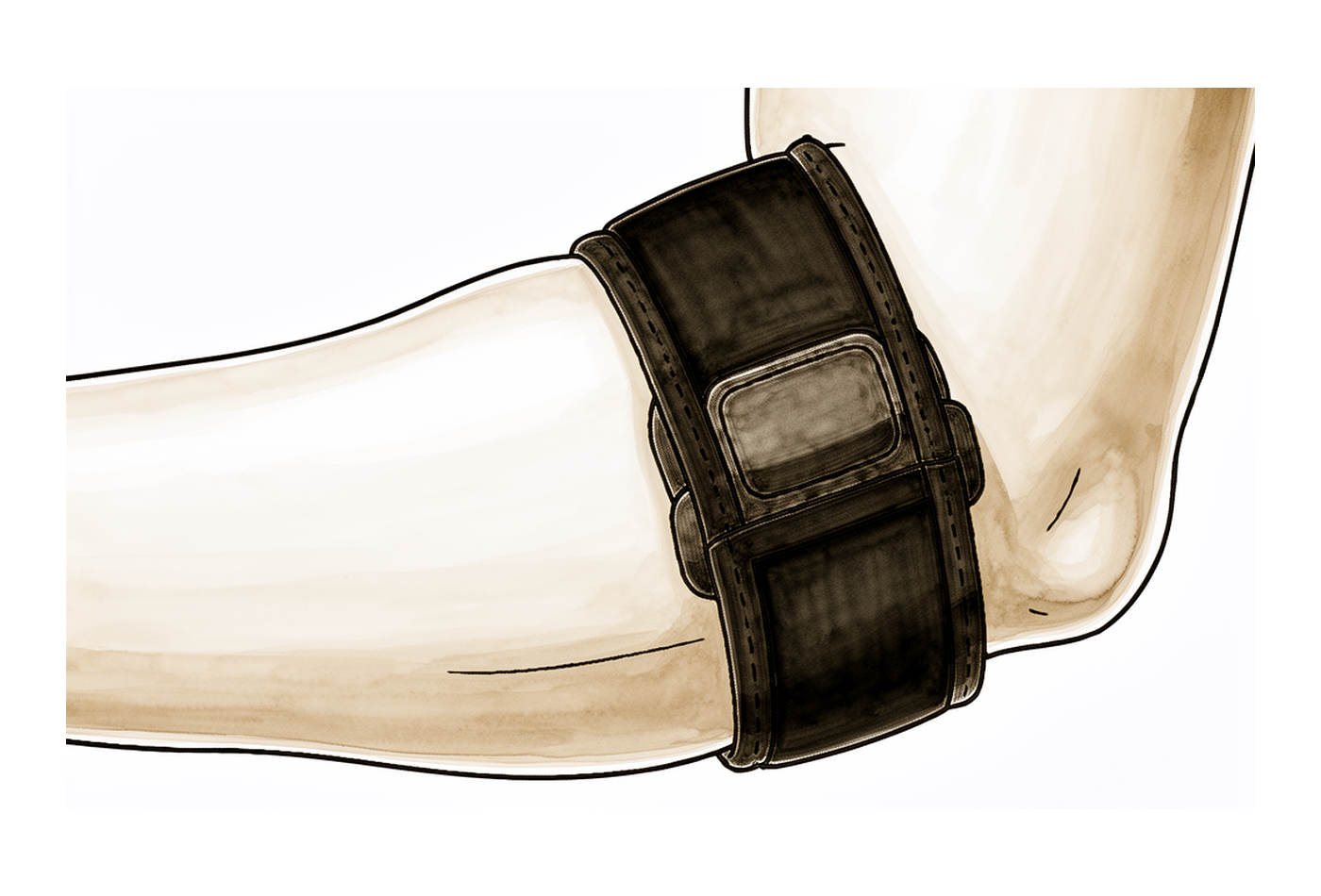
Counterforce brace
Wear the brace around your forearm a few centimetres below the inner elbow, over the muscle bulk — not over the bony bump itself. It should feel firm but not tight enough to make your hand tingle or go numb. Use it during aggravating activities (gripping, lifting, sport) in the early weeks, and wean off it as your symptoms settle.
During aggravating activity; wean as symptoms allow
Kieran Hirpara 4.0
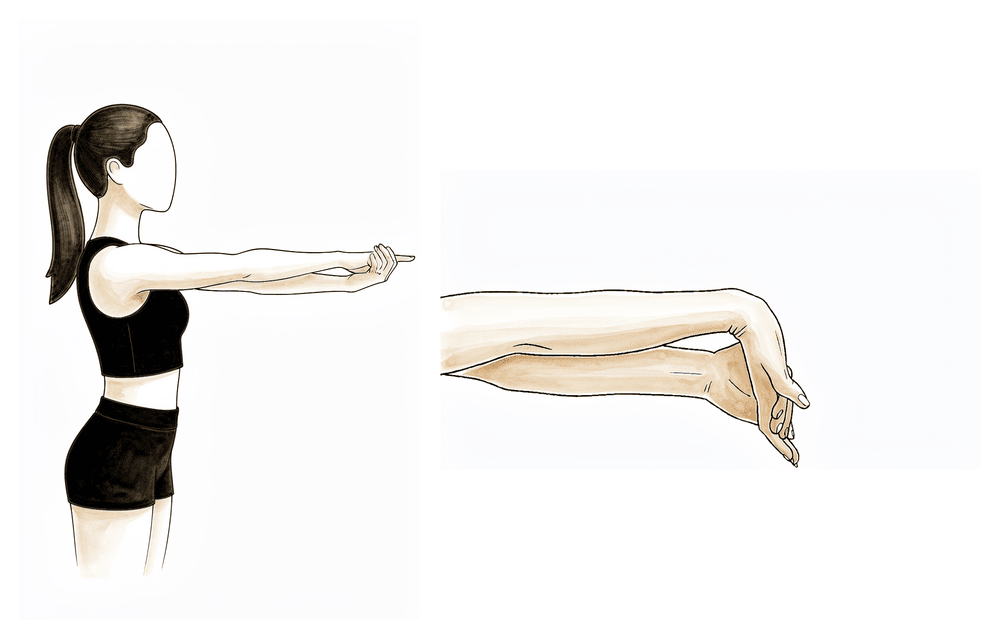
Wrist flexor stretch
Straighten your affected arm out in front of you with the palm facing up. With your other hand, gently pull your fingers and wrist down towards the floor until you feel a comfortable stretch along the inner forearm. Early on, keep the elbow bent to about 90°; as you improve, do the stretch with the elbow straight. Hold without bouncing.
Hold 20–30 seconds, 3–5 times, 2–3 times daily
Kieran Hirpara 4.0
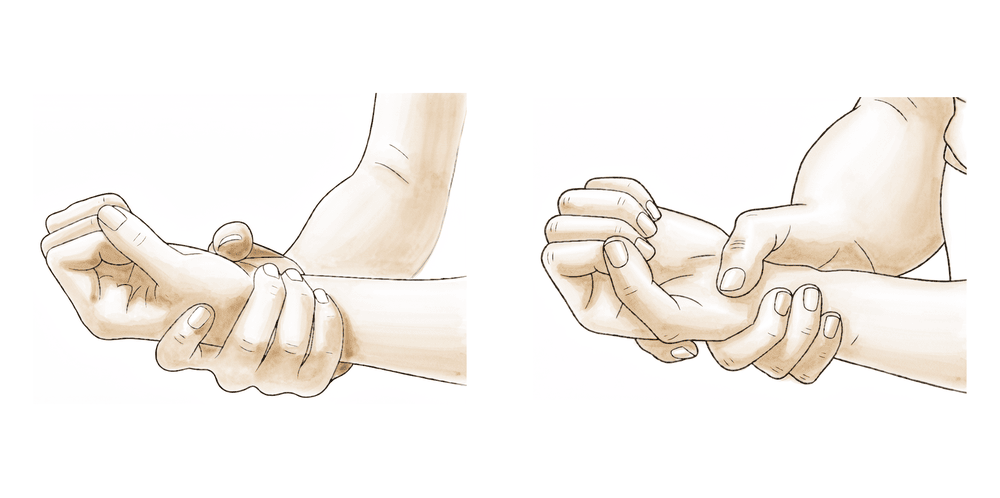
Pronator stretch
With your elbow tucked by your side, turn your palm to face the floor. Use your other hand to gently turn the forearm a little further into the palm-down position until you feel a mild stretch on the inner forearm. Keep it gentle and pain-free.
Hold 20–30 seconds, 3–5 times, 2–3 times daily
Kieran Hirpara 4.0
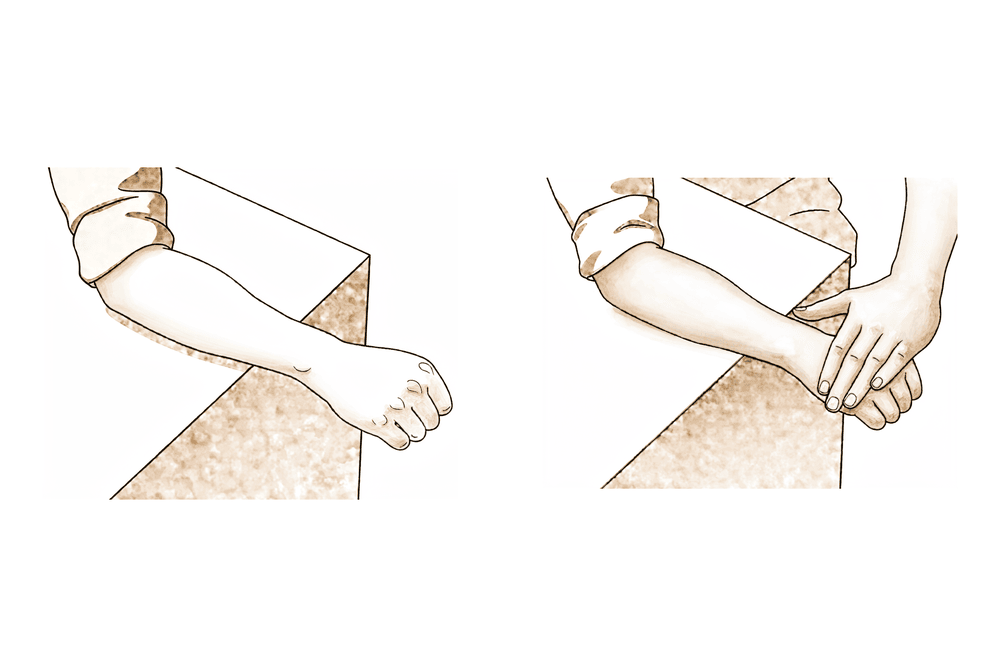
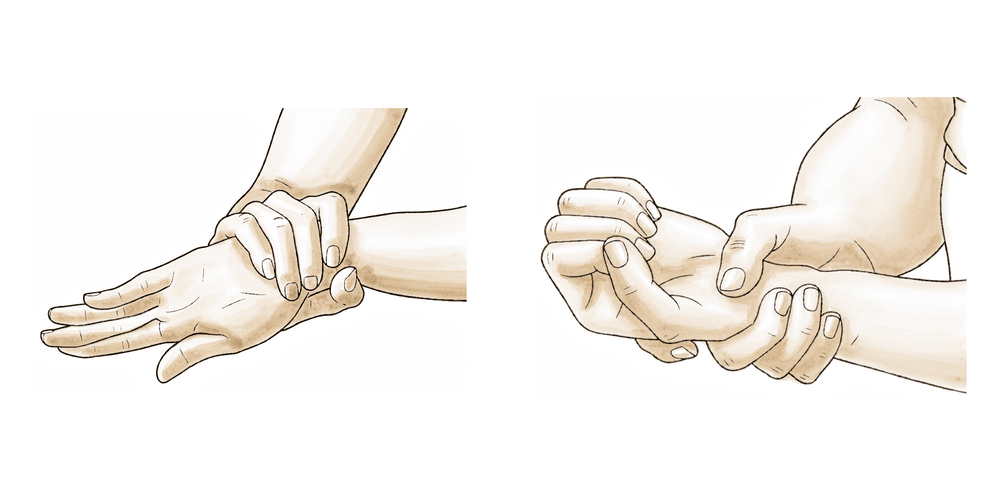
Wrist isometric (flexor) loading
Rest your forearm on a table with the palm facing up. Press the palm of your other hand against your fingers and try to curl your wrist up, but hold it still so the wrist does not actually move — a steady hold against resistance. This is an early-stage exercise to load the tendon gently and ease pain.
Hold 30–45 seconds, 5 holds, 1–2 times daily
Kieran Hirpara 4.0
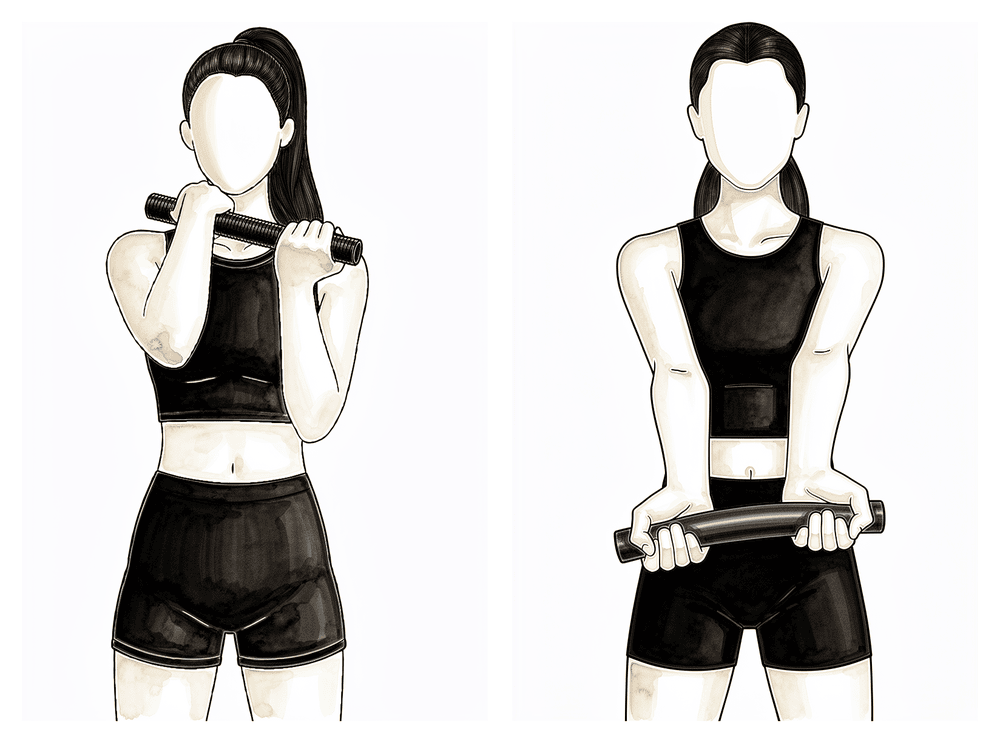
Reverse Tyler twist (eccentric flexor loading)
Hold a rubber exercise bar (FlexBar) in your affected hand with the wrist curled up (palm towards you), and twist the bar with your good hand. Bring the bar out in front of you, then slowly let your affected wrist uncurl in a controlled way over 3–4 seconds — your good hand does the twisting, your affected wrist does the slow controlled release (the 'eccentric' part). This is the key strengthening exercise for golfer's elbow and is introduced once early pain has settled (from about week 4).
3 sets of 15, once daily
Kieran Hirpara 4.0
Forearm rotation
With your elbow tucked by your side, slowly turn your palm up towards the ceiling, then down towards the floor, keeping the elbow still. This keeps the rotating muscles of the forearm moving and loads the pronators gently as you progress.
10 times each direction, 2–3 times daily

Kieran Hirpara 4.0
Grip strengthening
Squeeze a soft ball or therapy putty, hold briefly, then relax. Introduce this once your stretching and eccentric loading are comfortable — it builds the grip and forearm strength you need for daily tasks and sport. Stop short of sharp pain.
10–15 squeezes, 2–3 times daily
Kieran Hirpara 4.0
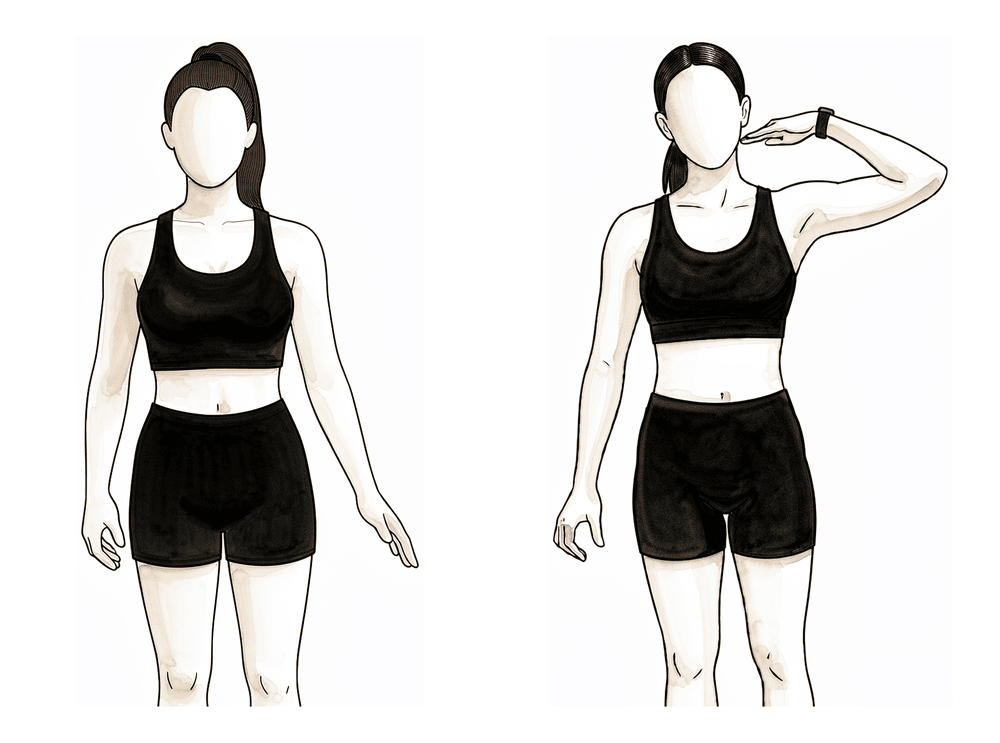
Ulnar nerve glide
The ulnar nerve runs in a groove just behind the bony bump on the inner elbow, and is often irritable in golfer's elbow. To keep it gliding freely: make an 'OK' ring with your thumb and index finger, then bring it up towards your face so the ring sits around your eye, with the elbow bent and the palm towards you. Move gently in and out of the position. Do NOT push into pins-and-needles or numbness — back off if your little and ring fingers tingle, and tell your therapist or the rooms if nerve symptoms are getting worse.
5–10 gentle glides, 2–3 times daily
These are the exercises from your handout. Start them as guided by Dr Hirpara and your therapist. In the early weeks the emphasis is on settling pain, gentle movement and the isometric holds; the eccentric reverse Tyler twist and grip strengthening are added as you improve. The ulnar-nerve glide is included because the nerve is so often involved on the inner elbow; keep it gentle.
Your clinical protocol¶
The rest of this page is the clinical rehabilitation protocol. This section is to be provided to your physiotherapist or hand therapist. It is criteria-gated rather than purely time-based: progress between phases depends on meeting the goals listed, not simply on the calendar. The ulnar nerve is screened at every visit (Tinel's sign, subluxation), as roughly 50–60% of medial cases have concomitant ulnar nerve symptoms, which are the leading reason conservative care fails.
There are two pathways below: the non-operative program (first-line, for the great majority) and the post-operative program (for the minority who proceed to surgery after failing conservative care).
Non-operative pathway¶
Phase I: Acute / pain control (0–2 weeks)
Goals: settle pain; restore full unloaded range of motion.
- Relative rest and activity modification: use pain as the limiter; avoid immobilisation. Modify golf, throwing, swimming, racquet sports, weightlifting and repetitive gripping.
- Optional counterforce brace over the common flexor mass; a wrist splint may be used if acutely painful.
- Pain-control adjuncts: ice, soft-tissue work / IASTM, gentle pain-free active range of motion (AROM), nerve glides.
- Screen the ulnar nerve (Tinel, subluxation).
- Criteria to progress: full unloaded AROM without pain; independent home program.
Phase II: Sub-acute / early loading (2–4 weeks)
Goals: begin flexor-pronator loading; address the proximal chain.
- Isometric wrist-flexor and pronator loading (light).
- Progressive stretching of the wrist flexors at 90° elbow flexion.
- Proximal kinetic chain: scapular stabilisers (serratus anterior, mid/lower trapezius) and rotator cuff, critical in throwers where medial elbow overload is valgus-driven.
- Criteria to progress: full ROM maintained; tolerates the 90° stretch; ~70% of contralateral strength.
Phase III: Strengthening / return (4–6+ weeks)
Goals: restore load tolerance and return to function and sport.
- Eccentric-concentric loading of wrist flexion and forearm pronation: the medial analogue of the Tyler twist is the "reverse Tyler twist" (eccentric wrist flexion on a FlexBar). Combined eccentric-concentric loading is favoured; isometrics remain useful for early analgesia.
- Mobilisation-with-movement; progress stretching towards the elbow-extended position.
- Grip strengthening, then sport-specific loading; for throwers, an interval throwing program; plyometrics last.
- Wean the counterforce brace as the elbow becomes asymptomatic; address equipment and technique.
- Return-to-sport criteria: ~90% of contralateral strength, pain-free function, self-management.
Post-operative pathway (flexor-pronator debridement ± repair ± ulnar nerve procedure)¶
Surgery is reserved for the minority failing ≥6 months of conservative care. The open Nirschl-type operation debrides the pathological flexor-pronator origin and commonly repairs/reattaches it; the ulnar nerve is assessed and protected, with decompression or anterior transposition performed concurrently in a proportion of cases.
Phase 1: Protect (0–2 weeks)
- Posterior long-arm splint (elbow + wrist) for 10–14 days; sling for community use.
- Elevation and oedema control; finger/tendon-glide AROM; active shoulder ROM; gentle cervical AROM.
- Precautions: NO lifting, pushing, pulling or forceful gripping: protect the repair.
Phase 2: ROM restoration (2–6 weeks)
- At the ~2-week visit: suture removal; transition to a neutral wrist orthosis full-time (off for hygiene); Tubigrip at the elbow for swelling.
- Begin AROM elbow flexion/extension (2–4 wk), then 4-way wrist AROM + forearm rotation and finger/thumb AROM (4–6 wk).
- Ulnar nerve glides introduced at weeks 4–6 (the medial-specific addition).
- Scapular stabilisation (gravity-resisted). No resistance strengthening until after 6 weeks.
Phase 3: Strengthening (6–12 weeks)
- Wean the orthosis as tolerated (night use may continue early on).
- Progressive resistive strengthening of wrist and forearm. No resisted supination/pronation early; begin lifting in supination/neutral, with light pronated lifting from ~week 9.
Phase 4: Return to activity / sport (12–16+ weeks)
- Progress lifting in all forearm positions as tolerated; full return to activity by ~12–16 weeks; sport-specific / interval throwing program for athletes. Full recovery is commonly 3–6 months.
Ulnar nerve precautions: if an anterior transposition was performed, limit end-range elbow flexion early and progress nerve excursion gradually. Persistent or worsening ulnar symptoms warrant surgeon review before advancing loading.
Getting back to work and activity¶
How quickly you return depends on which pathway you are on and the demands of your job and sport.
Non-operative. You can usually keep working and stay active throughout, modifying the tasks that flare the elbow rather than stopping completely. Golf, throwing sports, swimming and racquet sports are eased back in during the strengthening phase, once your strength is roughly 90% of the other side and function is pain-free. Because golfer's elbow is self-limiting, full resolution may take 6 to 18 months even though day-to-day function improves much sooner.
Post-operative. Light, restricted use begins early but heavier lifting and gripping are held back to protect the repair. Most people return to full activity by about 12 to 16 weeks, with full recovery commonly taking 3 to 6 months. Throwing athletes follow a graduated interval throwing program before returning to competition.
Driving: avoid driving while you are in a splint or sling, or while the elbow is too sore to control the car safely. Resume once you are out of the splint and can move the arm comfortably, as confirmed at your review.
After your protocol¶
This protocol works alongside the practice's general recovery advice; see managing post-operative pain, wound care and hand therapy basics. Golfer's elbow shares its loading-based approach with its outer-elbow counterpart, tennis elbow; ask your therapist if you would like the equivalent lateral epicondylitis guidance. Your ongoing recovery is guided individually by your physiotherapist or hand therapist according to how your elbow progresses.
Evidence & references
Medial Epicondylitis (Golfer's Elbow) — Flexor-Pronator Tendinosis: Conservative Loading & Post-operative Rehabilitation¶
Topic scope: (A) the loading-based non-operative rehabilitation of medial epicondylitis — a degenerative tendinopathy of the flexor-pronator origin (chiefly flexor carpi radialis and pronator teres) at the medial epicondyle — with mandatory ulnar-nerve screening; and (B) post-operative rehabilitation after open flexor-pronator debridement (± repair, ± concurrent ulnar nerve decompression/transposition), reserved for the minority failing ≥6 months of quality conservative care.
Defining principle: medial epicondylitis is not an inflammatory condition but a degenerative tendinosis, so the treatment is graded tendon loading, not rest. The protocol mirrors lateral elbow tendinopathy but with two practice-defining differences Dr Hirpara emphasises: (1) the loaded group is the wrist flexors/pronators (hence the eccentric "reverse Tyler twist" rather than the lateral Tyler twist), and (2) the ulnar nerve lies immediately behind the medial epicondyle, so concomitant ulnar neuritis (~50–60% of cases) is screened at every visit and is the leading reason conservative care fails. Surgery is a last resort after ≥6 months.
Medial epicondylitis is far less studied than its lateral counterpart — it is ~5–10× less common (prevalence ~0.4% vs 1.3%; ~10–20% of all epicondylitis). Most evidence is extrapolated from lateral elbow tendinopathy and from older operative case series; dedicated medial RCTs are sparse. Phase timelines below come from institutional Standard-of-Care protocols (Mass General Brigham combined medial/lateral; UVA medial debridement; Campbell's / Nirschl) plus operative series.
A. NON-OPERATIVE REHABILITATION (phased)¶
First-line; the majority resolve without surgery. Largely the SAME phased structure as the lateral elbow (Mass General Brigham publishes ONE combined medial/lateral protocol), with the loading target shifted to the flexor-pronator mass. Expected resolution 6–18 months (self-limited).
Phase I — Acute / pain control (~0–2 weeks). Relative rest + activity modification using pain as the limiter (avoid immobilisation). Aggravators to modify: golf, throwing (esp. late-cocking / acceleration valgus load), swimming, bowling, racquet sports, weightlifting, repetitive gripping. Optional counterforce brace over the common flexor mass; wrist splint if acutely painful. Pain-control adjuncts: ice, soft-tissue / IASTM, gentle pain-free AROM, dry needling, nerve glides. Screen the ulnar nerve (Tinel, subluxation). Criterion to progress: full unloaded AROM without pain; independent home program.
Phase II — Sub-acute / early loading (~2–4 weeks). Isometric wrist-flexor and pronator loading (minimal load). Progressive stretching of the wrist flexors at 90° elbow flexion. Proximal kinetic chain: scapular stabilisers and rotator cuff — critical in throwers, where medial elbow overload is valgus-driven. Criteria to progress: full ROM maintained; tolerates the 90° stretch; ~70% contralateral strength.
Phase III — Late / strengthening & return (~4–6+ weeks). Eccentric and concentric loading of wrist flexion and forearm pronation — the medial analogue of the Tyler twist is a "reverse Tyler twist" (eccentric wrist flexion on the FlexBar). Combined eccentric-concentric loading is favoured; isometrics for early analgesia. Mobilisation-with-movement; progress stretching to the elbow-extended position. Grip strengthening, then sport-specific loading; for throwers, an interval throwing program; plyometrics last. Wean counterforce brace as asymptomatic; equipment/technique modification. Return-to-sport criteria: ~90% contralateral strength, pain-free function, self-management.
B. POST-OPERATIVE REHABILITATION (flexor-pronator debridement ± repair, ± ulnar nerve procedure)¶
Surgery is for the minority failing ≥6 months of conservative care. The open Nirschl-type operation debrides the pathologic flexor-pronator origin (incision posterior to the medial epicondyle to spare the medial antebrachial cutaneous nerve), with repair/reattachment commonly by suture anchor. The ulnar nerve must be assessed and protected: ulnar neuritis is addressed concurrently (decompression or anterior transposition) in roughly 20–50% of operative series. The phase timeline blends the UVA "Golfer's Elbow Debridement (with tendon repair)" protocol and the Verma / Midwest-Orthopaedics-at-Rush medial/lateral debridement protocol.
Phase 1 — Protect / immobilise (Weeks 0–2). Posterior long-arm splint (elbow + wrist) for 10–14 days; sling for community use. Elevation; oedema control; finger/tendon-glide AROM; unaffected-joint motion; active shoulder ROM; gentle cervical AROM. Precautions: NO lifting / pushing / pulling / forceful gripping; protect the repair.
Phase 2 — ROM restoration (Weeks 2–6). At the 2-wk visit: suture removal; transition to a wrist orthosis in neutral full-time (off for hygiene); Tubigrip at the elbow for swelling. Begin AROM elbow flexion/extension (2–4 wk), then 4-way wrist AROM + forearm rotation, finger/thumb AROM (4–6 wk). Ulnar nerve glides introduced ~weeks 4–6 (the explicit medial-specific addition). Scapular stabilisation (gravity-resisted). No resistance strengthening until after 6 weeks.
Phase 3 — Strengthening (Weeks 6–12). Wean the orthosis as tolerated (consider night use early). Progressive resistive strengthening of wrist and forearm; per Verma, no resisted supination/pronation early, lifting begun in supination/neutral, with light pronated lifting from ~week 9.
Phase 4 — Return to activity / sport (Weeks 12–16+). Progress lifting in all forearm positions as tolerated; full return to activity by ~12–16 weeks; sport-specific / interval throwing program for athletes. Full recovery commonly 3–6 months.
Ulnar nerve precautions: if an anterior transposition was performed, limit end-range elbow flexion early and progress nerve excursion gradually; persistent or worsening ulnar symptoms warrant surgeon review before advancing loading.
C. PHASED TIMELINE SUMMARY¶
| Pathway | Phase | Window | Immobilisation | Loading / key actions | Criteria / milestone |
|---|---|---|---|---|---|
| Non-op | I — Pain control | 0–2 wk | None (avoid casting); optional counterforce brace | Activity modification; pain-free AROM; nerve glides; ulnar screen | Full unloaded AROM, pain-free |
| Non-op | II — Early loading | 2–4 wk | None | Isometric flexor/pronator load; 90° wrist-flexor stretch; scapular/cuff | ~70% contralateral strength |
| Non-op | III — Strengthen / return | 4–6+ wk | Wean brace | Reverse Tyler twist (eccentric); grip; sport-specific; throwers' interval program | ~90% strength, pain-free → RTS |
| Post-op | 1 — Protect | 0–2 wk | Posterior long-arm splint 10–14 d + sling | Finger glides, shoulder ROM; oedema control | No resistance; repair protected |
| Post-op | 2 — ROM restore | 2–6 wk | Neutral wrist orthosis | Elbow AROM → 4-way wrist + forearm rotation; ulnar glides wk 4–6 | No resistance until >6 wk |
| Post-op | 3 — Strengthen | 6–12 wk | Wean orthosis | Progressive resistance; supinated/neutral lifting → light pronated ~wk 9 | Restored strength in safe positions |
| Post-op | 4 — Return | 12–16+ wk | None | Lifting all forearm positions; interval throwing | Full return ~12–16 wk; recovery 3–6 mo |
D. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Sparse high-level evidence. Almost no medial-specific RCTs; recommendations are extrapolated from lateral elbow and from retrospective operative series (Kurvers & Verhaar 1995 remains a cornerstone). Strength of evidence is materially weaker than for lateral epicondylitis.
- Ulnar nerve is the dominant modifier. Concomitant ulnar neuropathy (reported 23–60%) worsens prognosis and is the leading reason conservative care fails; whether and how to address it surgically (decompression vs transposition vs medial epicondylectomy) is debated. Outcomes are reliably worse when ulnar symptoms coexist and are untreated.
- PRP may rival surgery for type-1 disease. Bohlen et al (OJSM 2020) found 2 leukocyte-rich PRP injections matched surgery for recalcitrant type-1 medial epicondylitis (29/33 success each) with faster recovery (pain-free ~56 vs ~108 days; full ROM ~42 vs ~96 days) — the surgical delay partly attributed to post-op bracing. Small evidence base.
- Corticosteroid: short-term only. As with the lateral elbow, steroid gives transient relief without durable benefit and risks recurrence; repeated injections show diminishing returns.
- Eccentric vs concentric. Same unsettled debate as the lateral elbow; combined eccentric-concentric flexor-pronator loading is the pragmatic standard, but direct medial trial data are minimal.
- Surgical technique. Open Nirschl debridement with repair is reliable in case series; arthroscopic medial debridement is emerging (claimed ulnar-nerve protection) but is technically demanding and under-evidenced. Debridement alone vs with repair remains unsettled.
E. EVIDENCE STRENGTH FLAGS (summary)¶
- MODERATE (non-operative rehab): the phased loading program — extrapolated largely from lateral elbow tendinopathy and combined medial/lateral institutional protocols; combined eccentric-concentric flexor-pronator loading is the pragmatic standard.
- LOW–MODERATE (post-operative rehab): phase timelines from institutional debridement protocols (UVA; Verma/Rush) and operative case series; no defining post-op rehab RCT.
- MODERATE (PRP for type-1 disease): single comparative study (Bohlen OJSM 2020) matching surgery with faster recovery; small sample.
- CONSENSUS / EXPERT: ulnar-nerve screening at every visit, ulnar-glide timing (wk 4–6 post-op), and the forearm-position lifting progression — drawn from surgeon-guidance protocols and operative practice rather than trial data.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Kurvers H, Verhaar J. The results of operative treatment of medial epicondylitis. J Bone Joint Surg Am. 1995. (ulnar neuritis coexistence 23–50%)
- Bohlen HL, et al. Platelet-rich plasma is an equal alternative to surgery in the treatment of type 1 medial epicondylitis. Orthop J Sports Med. 2020. DOI: 10.1177/2325967120908952
- Platelet-rich plasma versus Tenex in the treatment of medial and lateral epicondylitis. J Shoulder Elbow Surg. 2019.
- Ellenbecker TS, Nirschl R, Renstrom P. Current concepts in examination and treatment of elbow tendon injury. Sports Health. 2012.
- Rehabilitation of the thrower's elbow. Clin Sports Med. 2004.
- Nirschl surgical technique for concomitant lateral and medial elbow tendinosis. Am J Sports Med. 2011.
- Imaging of the elbow in the overhead throwing athlete. Am J Sports Med. 2003. (ulnar neuritis in ~60% of throwers with medial epicondylitis)
- Outcome of partial medial epicondylectomy for cubital tunnel syndrome. Clin Orthop Relat Res. 2006.
- Coonrad RW, Hooper WR. Tennis elbow: its course, natural history, conservative and surgical management (includes medial). J Bone Joint Surg Am. 1973.
- Green's Operative Hand Surgery. 2021. (medial vs lateral prevalence; combined treatment chapter; Nirschl technique)
- Campbell's Operative Orthopaedics. 2020. (Box 46.3 Rehabilitation Protocol for Epicondylitis [Wilk/Arrigo/Andrews]; Nirschl medial technique, posterior incision sparing the MABC nerve)
Published protocols (URLs)¶
- University of Virginia Orthopaedics — Medial Epicondyle (Golfer's Elbow) Debridement (with tendon repair), Rehabilitation Guidelines. https://med.virginia.edu/orthopaedic-surgery/wp-content/uploads/sites/242/2024/09/Medial-Epicondyle-Golfers-Elbow-Debridement-with-tendon-repair.pdf
- Midwest Orthopaedics at Rush (Nikhil Verma, MD) — Post-Operative Rehabilitation Guidelines for Medial/Lateral Epicondyle Debridement. https://www.sportssurgerychicago.com/patient-resources/rehab-manuals/mediallateral-epicondyle-debridement/
- Mass General Brigham Sports Medicine — Rehabilitation Protocol for Medial/Lateral Epicondylalgia (non-operative), rev. April 2021. https://www.massgeneral.org/assets/MGH/pdf/orthopaedics/sports-medicine/physical-therapy/rehabilitation-protocol-for-medial-lateral-epicondylitis.pdf