Patients › Rehabilitation
Flexor Tendon Repair
An early-active-motion recovery plan after repair of a flexor tendon in the finger, using the Manchester short splint to move the healing tendon gently and safely from the first week while protecting the repair for six weeks.
This protocol guides your recovery after surgical repair of a flexor tendon in the finger (the cord that runs down the palm side of the finger and bends it into the palm) with Dr Kieran Hirpara at Mater Private Hospital Rockhampton. It begins with your home exercise program, followed by the structured clinical protocol written for your hand therapist: bring this page or its PDF to your first therapy visit so your rehabilitation stays coordinated. Your hand therapist may adjust the plan depending on how your recovery progresses.
If you have any concerns about your wound after surgery, get in touch with the rooms. It is often helpful to take a photo of the wound and email it for review.
What to expect¶
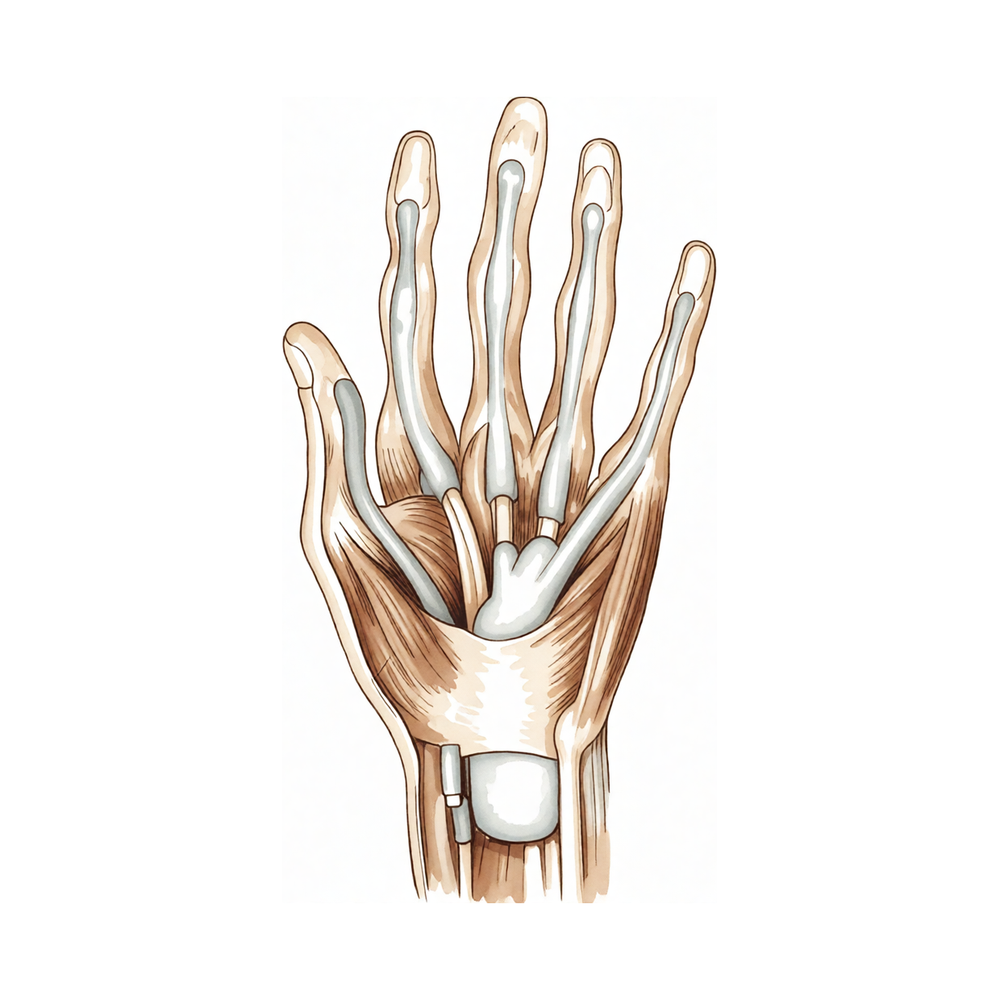
A flexor tendon repair stitches the cut ends of the tendon back together so the finger can bend again. The repair is strong enough to move gently straight away, but it is at its weakest in the first few weeks while the tendon knits, so the whole plan is built around moving it just enough to keep it gliding, without ever loading it hard enough to snap the stitches.
To do this, your hand is rested in a special lightweight splint called the Manchester short splint. Unlike older, bulkier splints, it is short, ending at the wrist crease, so your wrist is left free. It lets your wrist move fully forwards and back to about 45 degrees, while a small block holds your big knuckles from straightening past about 30 degrees and leaves your finger joints free to move. You wear it full-time for six weeks, taking it off only as instructed for exercises and washing.
The clever part is how the wrist is used. When you bend your wrist forwards, your finger straightens out almost by itself (this is called the tenodesis effect), and it lets you open the finger fully without your own muscles forcing it. When you bend your wrist back, it becomes easier and safer to gently curl the finger. Moving this way keeps the tendon sliding and, crucially, stops the finger from curling up into a stiff, bent position, the most common problem after this kind of repair.
The early exercises (from about day 4–5) are gentle and specific: bending the finger passively first, then a light active 'hook' curl starting at the fingertip, then straightening the finger with the wrist bent. There is no hard gripping and no forced movement for six weeks. The splint comes off at six weeks, light strengthening starts, and most people return to full unrestricted use of the hand by ten to twelve weeks.
Precautions and limitations¶
- Wear the Manchester short splint full-time for six weeks: take it off only for your exercises and washing, as instructed.
- Do NOT make a hard, tight fist and do NOT grip, lift, pull or carry anything with the operated hand for the first six weeks: heavy loading can rupture the repair.
- Do NOT force the finger straight or force it bent; keep every movement gentle, within the range you have been shown.
- You may use the hand for very light, safe tasks excluding the injured finger, as long as nothing pulls or strains it.
- A snap or sudden 'give' with loss of finger bending may mean the tendon has ruptured: contact the rooms straight away if this happens.
- Do NOT drive while you are in the splint; driving resumes after the splint is removed (about six weeks), once your grip and control are adequate and you have been cleared.
For wound, swelling and scar management, see the practice's wound care guidance.
Your exercises¶
Passive fist stretch (IP flexion)
Use your other hand to gently curl the operated finger all the way into a fist, bending the finger joints fully — keep the finger completely relaxed so your other hand is doing all the work. This is done FIRST in every session to keep the finger joints supple and ready to move. It does not pull on the repair because your own muscle stays switched off. Move slowly and stop short of pain.
10 times, at the start of each session, several sessions a day

Active hook fist from the DIP
With your wrist bent back (extended) in or out of the splint, curl your fingertip down first to make a 'hook' — bending the end and middle joints while keeping the big knuckle straight. Hold gently, then release. Starting the curl at the fingertip glides the healing tendon the way it needs to. Use only gentle effort — never force it and never make a hard, tight fist.
10 times, several sessions a day as guided

Kieran Hirpara 4.0
Tendon glides (hook to straight to full fist)
Move gently through the tendon-gliding sequence: fingers straight, then a hook fist (fingertip curl), then a soft full fist, then back to straight. This keeps both flexor tendons sliding smoothly past each other and the surrounding tissue so they do not stick down. Keep every position light and easy — these are gliding movements, not strengthening, so there should be no straining.
5 of each position, several sessions a day as guided

Finger straightening with the wrist bent (synergy)
Let your wrist drop forwards (flexed) and then actively straighten your finger out. Bending the wrist this way naturally helps the finger straighten, so the finger extends easily without forcing. This is the key move that stops the finger curling up into a permanent bend — do it faithfully. Straighten only as far as it goes comfortably with the wrist helping; do not lever it straight.
10 times, several sessions a day as guided

Place-and-hold
Use your other hand to gently place the operated finger into a light fist, then let go and hold that position with just a whisper of your own muscle — barely enough to keep the finger there. This wakes the repaired tendon up safely because the hard work of bending is done by your other hand, and your own muscle only has to hold, not pull. Keep the effort tiny; relax fully between repeats.
Hold a few seconds, 5–10 times, only as guided by your hand therapist

Kieran Hirpara 4.0
Blocking (later, if adhesions)
A LATER exercise — only if your tendon is sticking down and your hand therapist starts it. Steady your finger by holding the bone just below the joint you want to move, then actively bend that one joint on its own (for example, hold the middle of the finger still and curl just the fingertip). This concentrates the glide at a single joint to free a tendon that has become tethered. Do not start blocking on your own — it is more demanding and is added only when your therapist judges it safe.
As guided by your hand therapist (later phase, only if needed)
These are the exercises from your handout. Start them only as guided by Dr Hirpara and your hand therapist, staying within whatever range and limits you have been given. Every session follows the same safe order: gently bend the finger passively first, then do your active 'hook' curl and tendon glides, then straighten the finger with the wrist bent to keep it from stiffening into a curl. Keep all of it light: this is gliding, not strengthening. Place-and-hold and blocking belong to later phases and should only be started when your hand therapist introduces them. Stop anything that causes sharp pain over the repair, and never make a hard fist before you are cleared.
Your clinical protocol¶
The rest of this page is the staged clinical protocol for rehabilitation after flexor tendon repair using the Manchester short splint and an early-active-motion (EAM) regimen. This section is to be provided to your hand therapist, and each phase opens with a plain-English explanation of what is happening. The repair is at its weakest in the early weeks and is loaded by active and resisted finger flexion (a hard fist); the protocol therefore protects against forceful flexion while deliberately driving tendon excursion and active IP extension to prevent the flexion contracture that is the principal nuisance complication.
Prior to treatment, check the patient's operation report and past medical history, and liaise with the treating surgeon regarding the zone of injury, the core-suture configuration and strength of repair, any pulley venting, and concurrent digital nerve repair. Dr Hirpara's flexor repairs are managed in a Manchester short dorsal splint (ends at the wrist crease) permitting full wrist flexion and extension to 45°, with the MCP joints blocked at 30° of flexion and the IP joints free, worn full-time for six weeks. Night extension gutters are added only if an IP flexion deformity develops.
Phase I — early active motion in the Manchester short splint (weeks 0 to 6)¶
The first six weeks protect the knitting repair while keeping the tendon gliding and the finger from stiffening into a flexion contracture. The hand is splinted full-time in the Manchester short splint (full wrist flexion, extension to 45°, MCP block at 30°, IPs free). Active motion starts around day 4–5. Every session runs in a set order: passive IP flexion first, then active hook fist initiating at the DIP with the wrist extended, then active IP extension with the wrist flexed (synergistic, anti-contracture). No forced end-range and no resisted flexion.
For your hand therapist:
Education and precautions - Splint full-time in the Manchester short splint: full wrist flexion, extension to 45°, MCP blocked at 30°, IPs free; off only for exercises and hygiene - Begin EAM at day 4–5 - No forced end-range flexion and no resisted flexion; no gripping, lifting or pulling - Light "safe" use of the hand excluding the injured finger - Night extension gutter only if an IP flexion deformity begins to develop
Management - Wound: surgical dressings as directed; monitor for infection - Oedema: elevation, gentle digital oedema control, manage adhesion risk - Exercise sequence each session: (1) full passive IP flexion first; (2) active hook fist initiating at the DIP with the wrist extended to 45°; (3) active finger extension with the wrist flexed (synergistic / tenodesis, anti-contracture); add place-and-hold to a light fist as guided - Hand-therapy review weekly through this phase
Criteria to progress - Wound healed; repair intact at six weeks; tendon gliding maintained; no significant IP flexion contracture
Phase II — out of the splint, soft-tissue and scar work (week 6)¶
At six weeks the splint comes off. The focus shifts to recovering full passive and active range, releasing any early tightness, and managing the scar. Strengthening has not started yet; a night extension splint is used only if a residual flexion deformity remains.
For your hand therapist:
Assessments - Active and passive ROM at MCP/PIP/DIP; presence of any IP flexion contracture; tendon-gliding quality (assess for adhesion); scar and wound review
Education and precautions - Splint discontinued at six weeks (night extension splint only for a residual IP flexion deformity) - Progress light functional use; still no resisted gripping or loading
Management - Soft-tissue stretching to restore full composite flexion and extension; commence scar management once healed - Continue tendon glides; introduce blocking if adhesions are limiting differential glide - Progress light functional use of the hand
Criteria to progress - Wound and scar settled; near-full passive ROM; gliding maintained; ready for graded strengthening
Phase III — strengthening and return (weeks 6 to 12)¶
With the repair more mature, graded stretching and progressive strengthening begin and are built up steadily towards unrestricted use. Return to full, unrestricted activity is expected at around ten to twelve weeks, criterion-based.
For your hand therapist:
Assessments - Composite ROM and any residual contracture; grip and pinch versus the other side; response of the repair to graded loading
Education and precautions - Begin graded stretching and progressive strengthening from around six weeks; build load gradually - Avoid sudden maximal grip or resisted loading until strength is rebuilt
Management - Progressive grip and pinch strengthening (putty → graded resistance); continue stretching for any residual tightness; continue scar work as needed - Advance towards full / unrestricted activity at 10–12 weeks - Consider discharge once ROM and strength are functional and a suitable return of activity is achieved; refer back to the treating surgeon if recovery plateaus or a flexion contracture persists
Criteria for return to full activity - Functional composite ROM; adequate, near-symmetrical grip and pinch strength; pain-free unrestricted use, typically by 10–12 weeks
Getting back to work and activity¶
Light, safe use of the hand (excluding the injured finger) is encouraged from the start within the splint, as long as nothing pulls, grips or strains the repair. Plan for help in the early weeks, because there is no gripping, lifting or carrying with the operated hand for the first six weeks. The splint comes off at about six weeks, and light strengthening begins from then.
Because you must not drive while you are in the dorsal splint, arrange transport for the first six weeks. Driving resumes after the splint is removed (about six weeks), once your grip and finger control are adequate and you have been cleared at your review. Return to full, unrestricted activity, including firm gripping and heavier tasks, is expected around ten to twelve weeks, built up gradually and judged by Dr Hirpara and your hand therapist on how the finger is moving and how strong it is, not by the calendar alone.
After your protocol¶
This protocol works alongside the practice's general recovery advice; see also managing post-operative pain, wound care and scar management. The phased plan above reflects published early-active-motion rehabilitation guidance after flexor tendon repair, and your ongoing recovery is guided individually by Dr Hirpara and your hand therapist according to how your finger progresses.
Evidence & references
Flexor Tendon Repair — Procedure Outcomes & Post-operative Rehabilitation (Manchester Short-Splint Early Active Motion)¶
Topic scope: post-operative rehabilitation after primary surgical repair of a flexor tendon in the finger (especially zone II) with a robust multi-strand core repair, mobilised on an early-active-motion (EAM) regimen using the Manchester short splint. This is a repair of a divided structure that is at its weakest in the first weeks, so — unlike a decompression — the rehab is a carefully graded protected-but-moving pathway: enough controlled tendon excursion to prevent adhesion and flexion contracture, without the forceful flexion that ruptures the construct.
Defining principle of the rehab here: a repaired flexor tendon must glide to heal well but must not be loaded hard while it is weak. The two competing failures are rupture (from forceful or resisted flexion) and adhesion / PIP flexion contracture (from too little controlled motion). The Manchester short splint resolves this tension by leaving the wrist free: holding the wrist in 45° of extension minimises the work of flexion (Savage) so a gentle active hook fist glides the tendon at low tension, while permitting wrist flexion harnesses the extensor tenodesis effect to drive active IP extension — the single most effective lever against the PIP flexion contracture that is the characteristic nuisance complication of zone II repair. The deliberate sequence each session (passive IP flexion → active hook fist from the DIP, wrist extended → active IP extension, wrist flexed) is what makes the regimen safe and anti-contracture.
A. PROCEDURE / REPAIR OUTCOMES (early active motion vs passive mobilisation)¶
Flexor tendon repair is technically demanding and historically complication-prone (rupture and adhesion). Modern multi-strand core repairs combined with early active motion have shifted outcomes decisively toward better motion, with the central trade-off being a small rupture risk against markedly better range and function.
- Early active motion gives better finger motion than passive mobilisation, at a small rupture cost. A systematic review of controlled mobilisation after zone II repair found EAM regimens produced better total active motion than passive (Kleinert/Duran) protocols, with a modest increase in rupture (~5% vs ~4%) [Starr 2013]. The contemporary consensus favours active regimens with robust repairs. Moderate–strong (SR).
- The Manchester short splint specifically improves IP extension without increasing rupture. A clinical audit comparing the Manchester short splint (MSS) with a traditional full-length dorsal splint in uncomplicated zone II repairs found less PIP extension deficit (median 15° vs 28° at 6 weeks, p=0.003; 6° vs 18° at 12 weeks), a greater DIP flexion arc (59° vs 30°), and more excellent/good Strickland grades with the MSS. Rupture was not significantly different (2/45, 4.4% MSS vs 3/76, 3.9% traditional) [Peck 2014]. The headline advantage is the reduction in PIP flexion contracture. Moderate (single-centre non-randomised audit, Level III–IV).
- Forearm-based (wrist-blocking) splints constrain the very motion that prevents contracture. A comparison of splint designs found the Manchester short splint allowed greater PIP extension than forearm-based splints [Newington 2021], consistent with the mechanistic rationale that freeing the wrist enables the synergistic IP-extension move. Moderate.
- Mechanistic basis. Positioning the wrist in ~45° extension minimises the work of flexion required for active digital flexion, lowering the tension on the repair during the active hook fist [Savage 1988]; allowing wrist flexion recruits the extensor tenodesis effect to achieve full active IP extension at low cost — the anti-contracture engine of the regimen. Mechanistic.
B. REHABILITATION / THERAPY EVIDENCE¶
The rehab questions are (1) active vs passive early mobilisation, (2) splint design, and (3) how to structure the session to prevent both rupture and contracture. The evidence supports a robust repair mobilised with early active motion, a short wrist-free splint, and a fixed safe exercise sequence delivered through formal hand therapy.
- Early active motion is the modern default for robust repairs. Active regimens (partial-range combined passive/active, place-and-hold, true active flexion) outperform passive-only protocols on motion and are now standard where the core repair is strong enough to tolerate active glide [Tang 2021; Starr 2013]. Moderate–strong.
- A defined, low-tension active sequence is what makes EAM safe. Therapy guidance emphasises passive flexion first (preconditioning the joints), place-and-hold / active hook fist to glide the tendon at minimal tension, and synergistic wrist-flexion finger-extension to recover IP extension — the explicit structure of the Manchester regimen [Neiduski & Powell 2019; Saint John protocol]. Moderate (consensus + protocol cohorts).
- Splint design materially changes the contracture outcome. Shorter, wrist-free splinting that permits the synergistic extension move yields greater PIP extension than traditional or forearm-based dorsal splints [Peck 2014; Newington 2021]. Moderate.
- All flexor repairs are routed through formal hand therapy. The regimen is exercise-order- and tension-sensitive and is delivered with weekly hand-therapy review through the six-week splinted phase; it is not a self-directed pathway. Consensus / standard of care.
Recovery trajectory (expected, evidence-anchored)¶
| Phase | Window | Restraint | Hand use / therapy focus | Strength / load | Notes |
|---|---|---|---|---|---|
| I — Early active motion (in MSS) | Week 0–6 | Manchester short splint full-time (full wrist flexion, extension to 45°, MCP block 30°, IPs free) | Start day 4–5; each session: passive IP flexion → active hook fist from the DIP (wrist extended) → active IP extension (wrist flexed); place-and-hold as guided; weekly therapy | No resisted flexion, no gripping/lifting; light safe use excluding the injured finger | EAM drives glide + anti-contracture; rupture risk highest now |
| II — Splint off, soft-tissue / scar | Week 6 | Splint discontinued (night extension gutter only for residual IP flexion deformity) | Restore full passive/active ROM; scar management; tendon glides; blocking if adhesions | Still no resisted loading | PIP flexion contracture is the complication to chase down here |
| III — Strengthen / return | Week 6–12 | Restrictions progressively lifted | Graded stretching; progressive grip/pinch strengthening (putty → resistance) | Build grip/pinch gradually | Return to full / unrestricted activity 10–12 weeks, criterion-based |
(Phase windows mirror the precautions in the patient protocol; they are typical guides, not trial-derived deadlines.)
C. KEY CONTROVERSIES / EVIDENCE QUALITY¶
- Active vs passive early mobilisation. EAM gives better motion than passive Kleinert/Duran regimens at a small rupture-rate cost (~5% vs ~4%); it is the contemporary default for strong core repairs [Starr 2013; Tang 2021]. Moderate–strong.
- Manchester short splint vs traditional dorsal splint. The MSS audit shows clearly better IP extension and DIP flexion arc with no significant increase in rupture, but it is a single-centre, non-randomised audit (Level III–IV) — the authors themselves call for an RCT. The improvement is consistent with the mechanism (wrist-free synergistic extension), which raises confidence above the study design alone. Moderate; RCT recommended.
- The PIP flexion contracture is the outcome that discriminates protocols. Rupture rates are broadly similar across modern regimens; what separates them is residual PIP extension loss, and that is where the short, wrist-free splint and the synergistic-extension move earn their place [Peck 2014; Newington 2021]. Moderate.
- Repair strength gates the regimen. EAM is only safe with a robust multi-strand core repair; the protocol assumes that and is surgeon-confirmed per case (zone, suture configuration, pulley venting, concurrent nerve repair). Consensus.
D. EVIDENCE STRENGTH FLAGS (summary)¶
- MODERATE–STRONG (SR): early active motion produces better finger motion than passive mobilisation after zone II repair, at a small rupture-rate increase (~5% vs ~4%) [Starr 2013]; modern partial-range active regimens are the contemporary standard [Tang 2021].
- MODERATE: the Manchester short splint reduces PIP extension deficit (15° vs 28° at 6 wk, p=0.003) and improves DIP flexion arc without significantly increasing rupture (4.4% vs 3.9%) [Peck 2014]; greater PIP extension than forearm-based splints [Newington 2021]; defined low-tension exercise sequence [Neiduski & Powell 2019; Saint John].
- MECHANISTIC / CONSENSUS: wrist 45° extension minimises work of flexion [Savage 1988]; wrist flexion harnesses the extensor tenodesis effect for active IP extension (anti-contracture); exact phase timings are typical guides, not trial-derived; single-centre non-randomised MSS evidence — an RCT is recommended.
CITATIONS¶
RAG corpus (180,000+ Orthopaedic articles)¶
- Peck FH, et al. A comparative study of two methods of controlled mobilization of flexor tendon repairs in zone 2 (the Manchester short splint). Hand Ther. 2014. DOI: 10.1177/1758998314533306
- Starr HM, et al. Flexor tendon repair rehabilitation protocols: a systematic review. J Hand Surg Am. 2013. DOI: 10.1016/j.jhsa.2013.06.025
- Neiduski RL, Powell RK. Flexor tendon rehabilitation in the 21st century: a systematic review. J Hand Ther. 2019. DOI: 10.1016/j.jht.2018.06.001
- Tang JB. Rehabilitation after flexor tendon repair and others: a safe and efficient update. J Hand Surg Eur Vol. 2021. DOI: 10.1177/17531934211037112
- Tang JB, et al. (IFSSH flexor tendon committee report). J Hand Surg Eur Vol. 2014. DOI: 10.1177/1753193413500768
- Newington L, et al. Splinting after flexor tendon repair: comparison of the Manchester short splint with forearm-based splinting on PIP joint extension. Hand Ther. 2021. DOI: 10.1177/17589983211017584
Flexor tendon rehabilitation literature (URLs)¶
- Saint John flexor tendon protocol — early active motion regimen for zone II repair (protocol description and outcomes). PMC. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5142498/
- Savage R. The influence of wrist position on the minimum force required for active movement of the interphalangeal joints. J Hand Surg Br. 1988 (mechanistic basis: wrist extension minimises the work of flexion). https://doi.org/10.1016/0266-7681(88)90258-2