How Cartilage Works (and Why It Struggles to Heal) PDF In-depth PDF¶
Cartilage is the smooth, glistening surface that caps the ends of the bones inside a joint. It is one of the most remarkable materials in the body — slipperier than ice, able to cushion a lifetime of loading — and yet, unlike bone and tendon, it has almost no ability to repair itself. That single fact explains why cartilage damage and osteoarthritis are such stubborn problems, and why protecting your cartilage matters so much. This page explains, in plain language, what cartilage is and why it heals so poorly — and then, for the curious, goes deeper into the beautiful engineering of this tissue and the active biology behind what we casually call "wear and tear".
What cartilage is and what it does¶
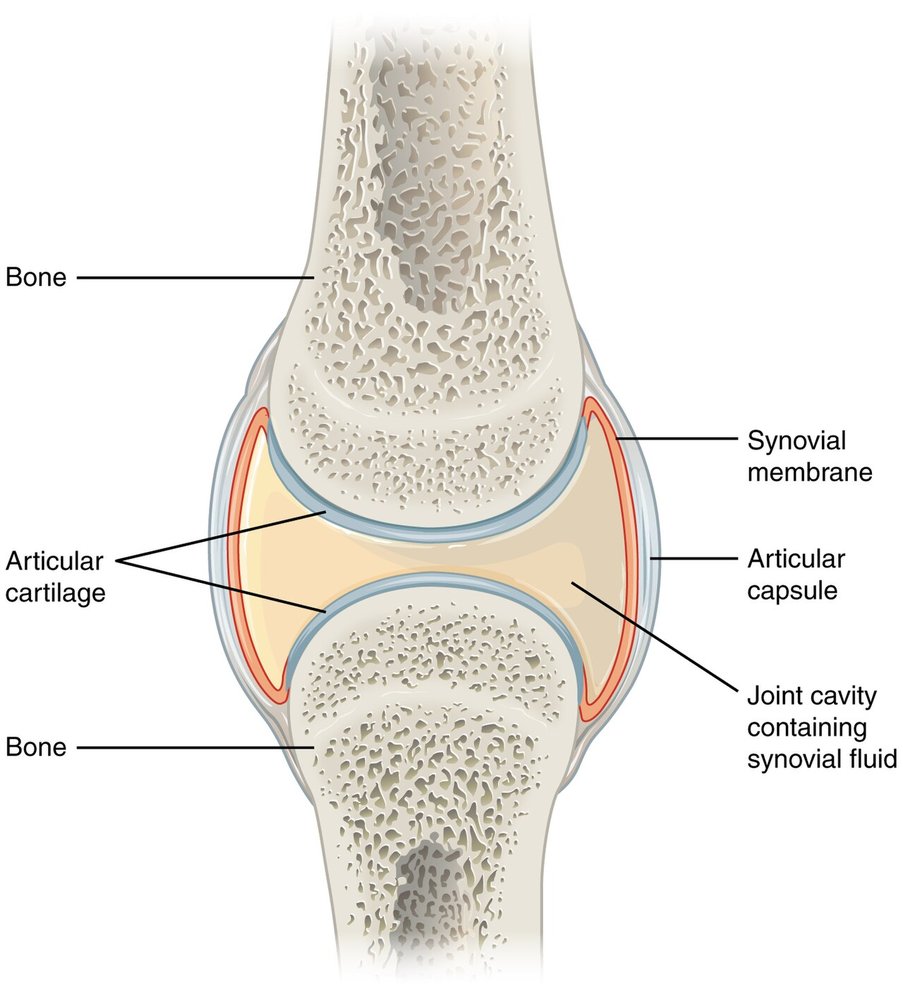
The cartilage we mean here — articular cartilage — is the firm, smooth, white coating just a few millimetres thick on the ends of bones where they meet in a joint. It does two things superbly:
- It is a near-frictionless gliding surface, so the bones of a joint slide over each other with almost no resistance.
- It is a cushion, spreading load across the joint and protecting the bone underneath from impact.
Cartilage is living tissue, but an unusual kind: it has no blood vessels and no nerves. The lack of nerves is why a worn cartilage surface itself doesn't hurt (the pain of arthritis comes from other structures). The lack of a blood supply is the key to its great weakness — it cannot heal the way skin or bone can.
Why cartilage struggles to heal¶
Almost everywhere else in the body, healing begins with bleeding — a clot forms, inflammatory cells arrive, and growth factors switch on repair. Cartilage has no blood supply, so an injury to it gets none of that. On top of that, its few resident cells are trapped in the surrounding material and cannot crawl to a wound to patch it.
The result is that a scrape or crack confined to the cartilage tends to simply stay there. Damage that goes deeper — through the cartilage and into the bone beneath — can fill in, but with a scar-like "fibrocartilage" that is weaker and less durable than the original. So cartilage damage tends to be permanent and slowly progressive, which is exactly why prevention and protection count for so much.
What helps protect your cartilage¶
- Keep moving. Cartilage is fed by joint fluid that is pumped in and out as you move; regular, comfortable activity nourishes it, while long periods of inactivity starve it.
- Keep a healthy weight. Every kilogram is extra load through the joint surfaces.
- Build the muscles around the joint. Strong muscles share the load and absorb shock, protecting the cartilage.
- Look after injuries. A wobbly or unstable joint wears its cartilage faster — treating instability protects the surface.
Advanced reading: the deeper science (optional)
This section steps up to a more detailed, student-level explanation of the biology. It isn't needed to understand a cartilage problem or its treatment — but if you're curious about how cartilage can be slipperier than ice, and why "wear and tear" is really an active disease, read on.
Cartilage as living tissue¶
Articular cartilage is a type called hyaline cartilage. It is built from a sparse scattering of cells — chondrocytes — surrounded by an enormous volume of matrix that those cells manufacture and maintain. The matrix is the secret to everything cartilage does. It is a meshwork of type II collagen fibres, filled with large, bottle-brush-shaped, intensely water-attracting molecules called proteoglycans (chiefly aggrecan), and roughly 70–80% water. The collagen net resists being pulled apart; the aggrecan sucks in water and generates a swelling pressure that resists being squashed. In effect, cartilage is a water-filled sponge held under tension inside a fibre net.
It is also uniquely isolated: no blood vessels, no nerves, no lymphatics. The chondrocytes sit in tiny chambers (lacunae), maintain their patch of matrix slowly, and — crucially — cannot move.
The near-frictionless bearing: how cartilage carries load¶
Cartilage is one of the slipperiest materials known: its coefficient of friction is around 0.001 — lower than ice sliding on ice. It achieves this with two mechanisms working together.
First, it is biphasic — a solid matrix soaked in fluid. When a joint is loaded, the trapped water cannot escape instantly, so it pressurises and carries the load — initially more than 90% of it. The fluid pressure, not the solid framework, bears the force, rather like standing on a water bed. As the contact point moves (because you keep moving), fluid weeps out ahead and is drawn back in behind. This interstitial fluid pressurisation is the main reason cartilage can bear huge loads with so little friction or wear.
Second, the surface carries a slippery boundary layer of molecules — lubricin (also called PRG4) and hyaluronic acid from the joint fluid — that forms a hydrated film keeping the two surfaces from ever touching directly.
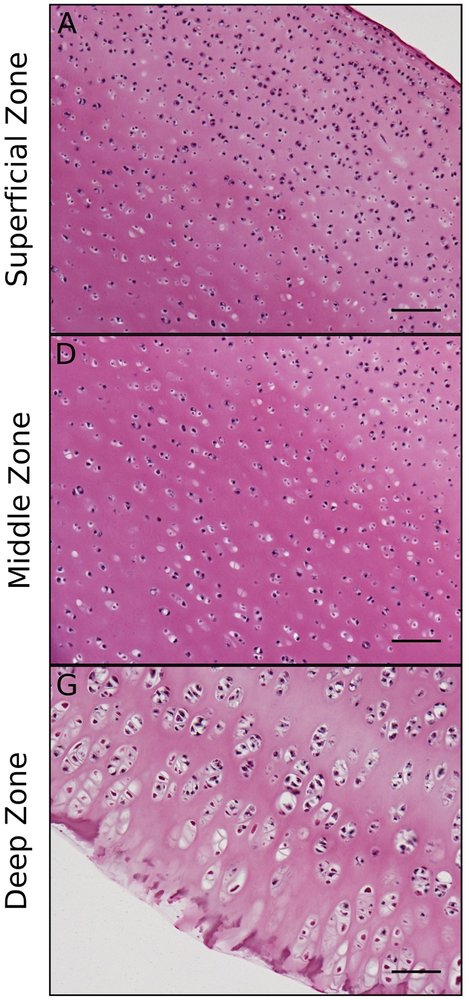
The matrix is also arranged in zones: collagen fibres run parallel to the surface in the top (superficial) zone, holding the lubricating layer and resisting shear; they become more random in the middle zone; and they anchor vertically in the deep zone, into a calcified cartilage layer (separated by a line called the tidemark) that bonds the soft cartilage firmly to the hard bone — the same engineering challenge of joining soft to hard that the tendon enthesis solves.
Why cartilage barely heals¶
Put the pieces together and the poor healing makes sense:
- No blood supply means no clot, no inflammatory cells, and none of the growth factors that drive repair elsewhere.
- The cells can't help much: chondrocytes are few, walled into the matrix, and don't migrate or multiply enough to fill a gap.
- Depth decides the response. A partial-thickness defect — confined to the cartilage — never reaches blood or marrow, so it gets essentially no repair response at all. A full-thickness defect that breaks through into the subchondral bone lets marrow cells and blood flood in, and these fill the gap — but with fibrocartilage (type I collagen, low in proteoglycan), which is mechanically inferior and wears out faster than true hyaline cartilage.
That is the central frustration of cartilage surgery: we can fill a hole, but not with the real thing.
How cartilage is fed¶
With no blood vessels of its own, cartilage is nourished by diffusion from the synovial (joint) fluid — and that diffusion is driven by movement and loading. Each time the joint is loaded and unloaded, fluid and nutrients are pumped in and out of the cartilage (much like the way finger movement feeds a healing flexor tendon). So cartilage genuinely needs cyclic loading to stay healthy: prolonged immobilisation or unloading degrades it, while moderate, regular activity maintains it. The physiotherapist's line that "motion is lotion" has a real biological basis here.
Osteoarthritis: when cartilage breaks down¶
Osteoarthritis (OA) is usually called "wear and tear", but that badly undersells it — it is an active biological process, not just mechanical erosion.
Set off by mechanical overload, injury, ageing or joint instability, the chondrocytes switch into a destructive mode. They ramp up matrix-digesting enzymes — MMPs (such as MMP-13) and aggrecanases (ADAMTS-4 and -5) — that chew through the type II collagen and aggrecan faster than they can be replaced. The matrix loses its water-holding proteoglycan, softens, and frays. The chondrocytes also change character (a shift called hypertrophy), the cartilage begins to calcify and admit blood vessels, the subchondral bone thickens and throws up bony spurs (osteophytes), and the joint lining (synovium) becomes mildly inflamed, releasing signals such as IL-1 and TNF that feed the cycle. Because cartilage cannot regenerate, this is largely a one-way street — which is why OA care centres on offloading, strengthening and weight management, and, when the cartilage is finally gone, joint replacement.
Repairing cartilage: why it's so hard¶
A range of operations try to restore a damaged surface, and the reason none is a perfect fix traces straight back to the biology above:
- Microfracture drills tiny holes into the subchondral bone to let marrow cells in. They form fibrocartilage — useful in the short term, but it tends to deteriorate after a couple of years.
- Osteochondral transfer (OATS / mosaicplasty) moves plugs of cartilage-and-bone from a lightly-loaded part of the joint. This is real hyaline cartilage, but supply is limited.
- Cell therapy (ACI / MACI) grows the patient's own chondrocytes in a laboratory and re-implants them — promising, but technically demanding and still imperfect.
None reliably recreates the original layered hyaline cartilage with its precise zonal architecture and lubrication. When the cartilage of a whole joint is worn out, the definitive answer remains joint replacement.
What helps and harms cartilage¶
- Movement and moderate loading nourish and maintain cartilage; prolonged immobilisation harms it.
- Excess weight and joint instability accelerate breakdown; strong surrounding muscles protect it.
- Injuries — especially those that destabilise a joint or damage the surface — raise the long-term risk of osteoarthritis.
- And the hard truth that runs through this whole page: once significantly damaged, cartilage does not grow back. For almost no other tissue does prevention matter more.
See also¶
- Osteoarthritis — what happens when cartilage breaks down across a joint
- How bone heals and remodels — the subchondral bone that lies beneath cartilage
- Staying active for joint health — why movement protects your joints
- Weight, obesity and joint health — how load affects cartilage